Sexually transmitted diseases (STDs) pose significant public health challenges worldwide, and while many are treatable with antibiotics, the development of vaccines to prevent them is a critical area of medical research. Currently, there are only a few vaccines specifically designed to protect against STDs, with the most well-known being the vaccines for hepatitis B and human papillomavirus (HPV). The hepatitis B vaccine has been widely available since the 1980s and is highly effective in preventing infection, which can lead to chronic liver disease and cancer. The HPV vaccine, introduced in the early 2000s, targets certain strains of the virus that cause cervical cancer, genital warts, and other health issues. Despite these advancements, vaccines for other common STDs, such as gonorrhea, chlamydia, syphilis, and herpes, remain in various stages of development or are not yet available. The limited number of STD vaccines underscores the ongoing need for research, innovation, and public health strategies to combat these infections effectively.
Explore related products






What You'll Learn
- HPV Vaccine: Protects against human papillomavirus, reducing risk of genital warts and certain cancers
- Hepatitis B Vaccine: Prevents hepatitis B, a sexually transmitted infection causing liver disease
- No HIV Vaccine: Despite research, no vaccine currently exists for HIV/AIDS prevention
- Herpes Vaccine Research: Ongoing studies aim to develop vaccines for genital herpes (HSV-2)
- Syphilis & Gonorrhea: No vaccines available yet, but research continues for prevention options
![]()
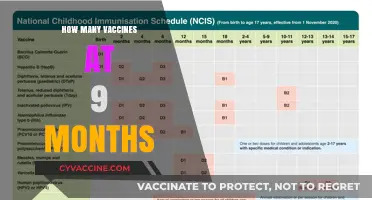
HPV Vaccine: Protects against human papillomavirus, reducing risk of genital warts and certain cancers
The HPV vaccine stands as a cornerstone in the fight against sexually transmitted infections, offering protection against a virus linked to significant health risks. Human papillomavirus (HPV) is one of the most common STIs, with certain strains causing genital warts and, more critically, cancers of the cervix, anus, penis, and throat. Unlike many STIs, HPV often presents no symptoms, making vaccination a proactive measure rather than a reactive one. This vaccine is unique in its ability to prevent both the immediate discomfort of genital warts and the long-term threat of cancer, setting it apart from other STI vaccines.
Administered in a series of shots, the HPV vaccine is most effective when given before potential exposure to the virus. The Centers for Disease Control and Prevention (CDC) recommends it for preteens at age 11 or 12, though it can be given as early as age 9. For those who missed this window, catch-up vaccination is advised up to age 26. Adults aged 27 to 45 may also benefit but should consult a healthcare provider to weigh the risks and benefits. The standard regimen involves two doses, spaced six to 12 months apart, for those vaccinated before their 15th birthday. Those vaccinated later or with specific health conditions may require three doses.
The HPV vaccine’s impact is measurable and profound. Since its introduction, rates of HPV infections and related conditions have plummeted. For instance, in countries with high vaccination coverage, cervical cancer rates have dropped significantly, and genital warts have become less prevalent. This success underscores the vaccine’s dual role: preventing individual suffering and reducing the public health burden of HPV-related diseases. It’s a testament to how targeted prevention can transform health outcomes on a large scale.
Practical considerations are key to maximizing the vaccine’s benefits. Side effects are typically mild, such as soreness at the injection site, fever, or dizziness, and last only a few days. Scheduling the vaccine alongside other routine immunizations can simplify the process for adolescents. For parents and caregivers, initiating conversations about the HPV vaccine early can normalize it as a routine part of healthcare. Schools and clinics often host vaccination drives, making access convenient. Ultimately, the HPV vaccine is not just a medical intervention but a tool for empowerment, offering protection against a pervasive and often silent threat.
Race for a Vaccine: Which Pharma Giant Leads the Charge?
You may want to see also
Explore related products





![]()
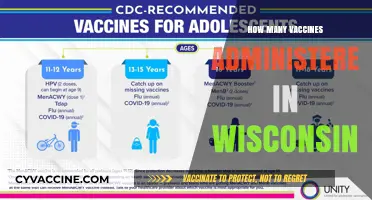
Hepatitis B Vaccine: Prevents hepatitis B, a sexually transmitted infection causing liver disease
The Hepatitis B vaccine stands as a critical tool in the prevention of a sexually transmitted infection that can lead to severe liver disease. Unlike many STDs, Hepatitis B has a highly effective vaccine, offering long-term protection with a simple series of shots. This vaccine is not just for high-risk groups; it’s recommended universally, starting in infancy, to ensure lifelong immunity. The typical regimen involves three doses: the first at birth (for infants), the second at 1–2 months, and the third at 6–18 months. For adults, the doses are spaced over six months, with the second dose given one month after the first and the third dose five months after the second. This schedule ensures robust antibody production, providing over 90% protection against the virus.
One of the most compelling aspects of the Hepatitis B vaccine is its dual role in prevention. Not only does it protect against sexual transmission, but it also guards against other routes of infection, such as contaminated needles or from mother to child during birth. This makes it a cornerstone of public health strategies, particularly in regions with high prevalence rates. For travelers or healthcare workers, the vaccine is especially crucial, as exposure risks can be unpredictable. It’s important to note that while the vaccine prevents Hepatitis B, it does not protect against other hepatitis viruses like Hepatitis C, which remains without a vaccine.
Despite its effectiveness, misconceptions about the Hepatitis B vaccine persist. Some worry about side effects, but these are typically mild—soreness at the injection site, low-grade fever, or fatigue—and resolve within a few days. Serious reactions are extremely rare. Another common myth is that the vaccine is only for promiscuous individuals or drug users. In reality, anyone can be exposed to Hepatitis B through everyday activities, making vaccination a prudent choice for all. Public health campaigns often emphasize this universality, aiming to normalize vaccination across age groups and lifestyles.
Practical tips for ensuring successful vaccination include scheduling doses in advance to avoid delays and keeping a record of completed shots for future reference. For parents, integrating the vaccine into the routine childhood immunization schedule is key. Adults who missed vaccination in childhood should consult a healthcare provider to start the series promptly. Additionally, combining the Hepatitis B vaccine with other vaccines, such as those for influenza or HPV, can streamline protection and save time. Ultimately, the Hepatitis B vaccine is a testament to the power of preventive medicine, offering a straightforward way to safeguard against a potentially life-threatening infection.
Understanding Vaccine Protection: How Long Until Immunity Takes Effect?
You may want to see also
Explore related products






![]()
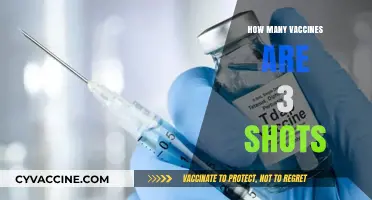
No HIV Vaccine: Despite research, no vaccine currently exists for HIV/AIDS prevention
Despite decades of intensive research, no vaccine currently exists to prevent HIV/AIDS. This stands in stark contrast to other sexually transmitted infections (STIs) like hepatitis B, where vaccination has become a cornerstone of prevention. While vaccines for hepatitis B, human papillomavirus (HPV), and others have transformed public health, HIV’s unique challenges have stymied efforts to develop an effective immunization. The virus’s rapid mutation rate, ability to evade the immune system, and complex integration into host cells have made it an elusive target for vaccine developers.
One of the primary obstacles in HIV vaccine development is the virus’s extraordinary genetic diversity. Unlike HPV, which has a relatively stable genome, HIV mutates rapidly, creating countless variants within a single infected individual. This variability complicates the creation of a broadly effective vaccine, as a single formulation must protect against multiple strains. Additionally, HIV targets and weakens the very immune cells—CD4 T cells—that vaccines typically rely on to mount a defense. This dual challenge of diversity and immune evasion has forced researchers to rethink traditional vaccine strategies.
Efforts to develop an HIV vaccine have explored innovative approaches, including mosaic vaccines, which combine fragments of different HIV strains to induce a broader immune response, and mRNA technology, inspired by its success in COVID-19 vaccines. Clinical trials, such as the RV144 trial in Thailand, have shown modest efficacy, but not enough to warrant widespread use. These partial successes highlight the complexity of the task and the need for continued investment in research. Until a breakthrough occurs, prevention relies on behavioral changes, antiretroviral therapy, and pre-exposure prophylaxis (PrEP), which, while effective, require consistent adherence.
The absence of an HIV vaccine underscores the disparity in medical advancements for different STIs. While HPV vaccines like Gardasil 9 protect against multiple strains with a three-dose regimen for individuals aged 9–45, HIV remains a global health crisis with no immunological solution. This gap highlights the urgent need for sustained funding, international collaboration, and public awareness to accelerate vaccine development. Until then, education and access to existing prevention methods remain critical in the fight against HIV/AIDS.
Preventing Exposure: BBP's Vaccine Breakthrough and Its Impact
You may want to see also
Explore related products






![]()
Herpes Vaccine Research: Ongoing studies aim to develop vaccines for genital herpes (HSV-2)
Currently, there are only vaccines for two sexually transmitted infections: hepatitis B and human papillomavirus (HPV). However, the landscape of STD prevention is evolving, with significant efforts directed toward developing vaccines for other persistent threats, including genital herpes caused by HSV-2. Despite decades of research, creating an effective herpes vaccine has proven challenging due to the virus’s ability to evade the immune system and establish lifelong latency. Yet, ongoing studies offer hope, with several candidates in clinical trials aiming to prevent infection, reduce viral shedding, or alleviate symptoms.
One promising approach involves subunit vaccines, which target specific HSV-2 proteins to stimulate an immune response. For instance, the vaccine candidate GEN-003 combines an immunotherapeutic protein (ICP0) with a proprietary adjuvant to boost T-cell activity. In Phase 2 trials, GEN-003 reduced viral shedding by 97% and genital lesions by 60% in individuals with symptomatic HSV-2. While not yet approved, these results suggest a potential breakthrough in managing the infection. Another strategy, pursued by Moderna, leverages mRNA technology to encode HSV-2 glycoproteins, mimicking the success of COVID-19 vaccines. Early-stage trials are underway to assess safety and immunogenicity, with hopes of broader protection against both HSV-1 and HSV-2.
Beyond prevention, therapeutic vaccines aim to help those already infected. These vaccines focus on reducing recurrence rates and transmission risk. For example, the Herpevac trial, though unsuccessful in preventing infection, demonstrated a 20% reduction in genital herpes symptoms among women already exposed to HSV-1. This highlights the complexity of vaccine development, as even partial efficacy could significantly improve quality of life for millions. Researchers are also exploring combination therapies, pairing vaccines with antiviral medications like valacyclovir, to maximize immune response and viral suppression.
Practical considerations for future herpes vaccines include dosage regimens, age-specific targeting, and accessibility. Clinical trials often involve 2–3 doses administered over several months, with booster shots potentially required to maintain immunity. Adolescents and young adults, who represent the highest-risk group for HSV-2 acquisition, would likely be prioritized for vaccination. However, cost and distribution challenges must be addressed to ensure global access, particularly in low-resource settings where HSV-2 prevalence remains high.
In conclusion, while a herpes vaccine is not yet available, ongoing research is closer than ever to turning this goal into reality. From subunit vaccines to mRNA innovations, these efforts reflect a multifaceted approach to tackling a persistent public health issue. As studies progress, the potential for a vaccine to prevent or control genital herpes offers a beacon of hope for reducing the burden of this lifelong infection. For now, individuals can protect themselves through safer sexual practices, regular testing, and open communication with partners—measures that remain critical until a vaccine becomes widely available.
Debunking the Myth: The Scientist Who Proved Autism Isn't Caused by Vaccines
You may want to see also
Explore related products






![]()
Syphilis & Gonorrhea: No vaccines available yet, but research continues for prevention options
Despite the existence of vaccines for several sexually transmitted diseases (STDs), such as hepatitis B and human papillomavirus (HPV), syphilis and gonorrhea remain without preventive inoculations. These two bacterial infections, caused by *Treponema pallidum* and *Neisseria gonorrhoeae* respectively, have proven particularly challenging for vaccine development due to their complex biology and ability to evade the immune system. While condom use and regular screening are effective preventive measures, the global burden of these infections—with millions of cases annually—highlights the urgent need for additional tools.
Research into syphilis and gonorrhea vaccines is active but fraught with obstacles. For syphilis, early-stage trials have explored subunit vaccines targeting specific proteins like TpF1, which plays a role in the bacterium’s attachment to host cells. However, translating these findings into a broadly effective vaccine has been slow, partly due to the disease’s long latency period, which complicates clinical trial endpoints. Gonorrhea presents an even greater challenge: the bacterium’s genetic diversity and ability to develop antibiotic resistance have made vaccine development a moving target. Efforts have focused on outer membrane proteins, such as PorB and Opa, but no candidate has yet progressed beyond phase 1 trials.
One promising approach for gonorrhea involves leveraging cross-protection from existing vaccines. For instance, the meningococcal group B vaccine (Bexsero) has shown some efficacy against gonorrhea in observational studies, likely due to shared antigens between the two pathogens. While not a dedicated solution, this finding suggests a potential interim strategy. Similarly, researchers are investigating whether a syphilis vaccine could also protect against other treponemal diseases, such as yaws, to broaden its appeal for development.
Practical considerations for future vaccines include dosage regimens and target populations. A syphilis vaccine might require a prime-boost strategy, with initial doses followed by periodic boosters to maintain immunity. For gonorrhea, a vaccine would ideally target adolescents and young adults, who bear the highest disease burden, but ensuring accessibility in low-resource settings remains a critical challenge. Until vaccines become available, combining behavioral interventions with improved diagnostics and treatment remains the cornerstone of prevention.
In conclusion, while syphilis and gonorrhea vaccines remain elusive, ongoing research offers hope for future breakthroughs. Collaborative efforts between scientists, public health officials, and pharmaceutical companies are essential to overcome technical and logistical hurdles. Until then, raising awareness about existing prevention methods and ensuring access to testing and treatment will remain vital in controlling these persistent infections.
Understanding How the Parvo Vaccine Protects Dogs from Parvovirus
You may want to see also
Frequently asked questions
There are currently three vaccines available for STDs: the HPV vaccine (Gardasil 9), the hepatitis A vaccine, and the hepatitis B vaccine.
No, vaccines are only available for a few STDs, specifically HPV, hepatitis A, and hepatitis B. There are no vaccines for common STDs like chlamydia, gonorrhea, syphilis, or HIV.
No, there is no single vaccine that protects against multiple STDs. Each vaccine targets a specific infection, such as HPV, hepatitis A, or hepatitis B.