Before the widespread use of vaccines, countless preventable deaths occurred annually due to infectious diseases such as smallpox, polio, measles, and influenza. These illnesses ravaged populations, particularly children and the elderly, leaving behind devastating societal and economic impacts. Vaccines have since emerged as one of the most effective public health interventions, drastically reducing mortality rates and eradicating some diseases entirely. Examining the historical toll of these preventable deaths highlights the transformative power of vaccination and underscores the importance of continued global immunization efforts to protect future generations.
Explore related products

$16.99





What You'll Learn
![]()
Pre-vaccine era mortality rates
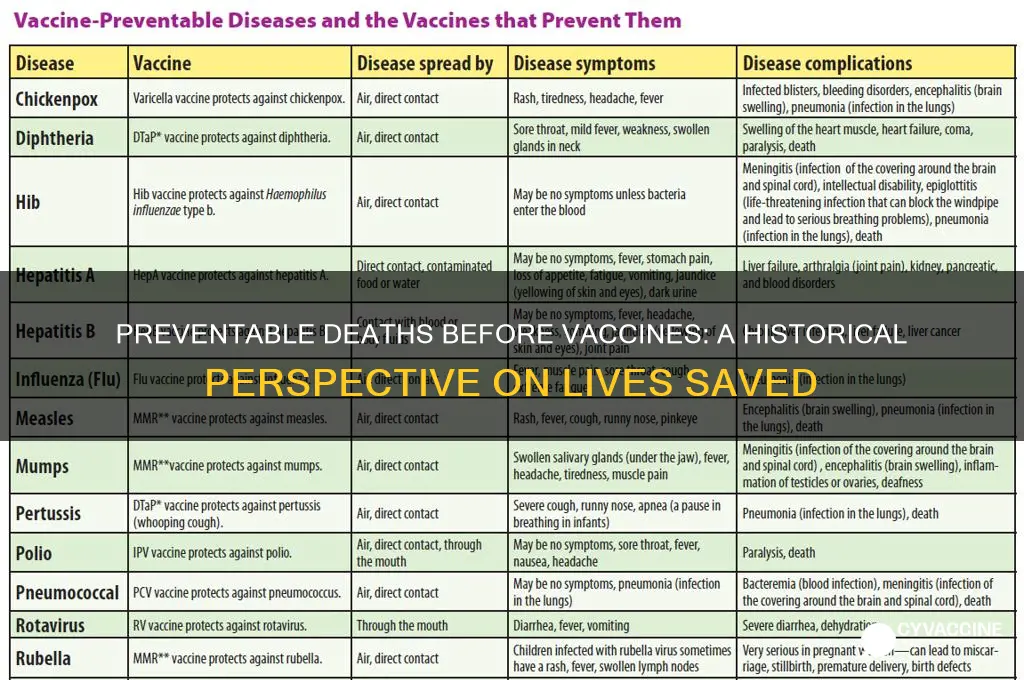
Before the advent of vaccines, mortality rates, particularly among children, were staggeringly high. Diseases like smallpox, polio, measles, and whooping cough ravaged populations, often leaving families bereft and communities scarred. For instance, in the early 20th century, measles alone caused an estimated 2.6 million deaths annually worldwide. These numbers underscore the pre-vaccine era’s grim reality: infectious diseases were not just common—they were expected, and their deadly outcomes were accepted as inevitable.
Consider the case of smallpox, a disease that once killed 30% of its victims and left survivors disfigured or blind. In the 18th century, it was responsible for an estimated 400,000 deaths annually in Europe alone. The introduction of the smallpox vaccine in 1796 by Edward Jenner marked a turning point, but its impact was gradual. By the mid-20th century, smallpox still claimed 2 million lives annually before global vaccination campaigns eradicated it by 1980. This example highlights how pre-vaccine mortality rates were not just numbers but reflections of widespread suffering and societal vulnerability.
Whooping cough (pertussis) offers another stark example. In the 1930s, before the pertussis vaccine became widely available, the U.S. reported over 200,000 cases annually, with fatality rates as high as 4% among infants. This translates to roughly 8,000 preventable deaths each year in the U.S. alone. Globally, the toll was far higher. The vaccine, introduced in the 1940s, reduced cases by 80% within two decades, illustrating the dramatic shift in mortality rates once immunization became routine.
Analyzing these trends reveals a clear pattern: pre-vaccine mortality rates were not only high but disproportionately affected the young and vulnerable. For example, polio, which primarily struck children under 5, caused paralysis in 1 out of every 200 infected individuals, with 5–10% of those paralyzed dying. In the U.S. alone, polio outbreaks in the 1940s and 1950s resulted in over 15,000 cases of paralysis annually. The introduction of the polio vaccine in 1955 led to a 99% reduction in cases globally, saving countless lives and preventing long-term disabilities.
The takeaway is undeniable: pre-vaccine mortality rates were a testament to humanity’s vulnerability to infectious diseases. Vaccines have not only reduced these numbers but transformed them, turning once-deadly illnesses into rare occurrences. For parents today, ensuring children receive vaccines like the MMR (measles, mumps, rubella) or DTaP (diphtheria, tetanus, pertussis) is a practical step to protect them from the devastating outcomes that were once commonplace. Understanding this history underscores the importance of vaccination as a cornerstone of public health.
Global Vaccine Rollout: Tracking Speed and Distribution Challenges
You may want to see also
Explore related products






![]()
Disease-specific preventable deaths
Before the advent of vaccines, certain diseases exacted a staggering toll on global health, claiming millions of lives annually. Among the most notorious were smallpox, polio, measles, and pertussis. Smallpox alone was responsible for an estimated 300 million deaths in the 20th century before its eradication in 1980 through vaccination. These disease-specific preventable deaths highlight the transformative impact of vaccines, turning once-deadly illnesses into rare occurrences in many parts of the world.
Consider measles, a highly contagious virus that caused approximately 2.6 million deaths annually before the introduction of the measles vaccine in 1963. Today, global deaths have plummeted to around 140,000 per year, primarily in regions with low vaccination coverage. This stark contrast underscores the vaccine’s efficacy: a single dose is 93% effective, while two doses provide 97% protection. For children under five, who are most vulnerable, timely vaccination is critical—the first dose is typically administered at 12 months, followed by a second dose at 4–6 years.
Pertussis, or whooping cough, offers another compelling example. In the pre-vaccine era, it caused around 200,000 deaths annually, predominantly in infants. The introduction of the DTaP vaccine (diphtheria, tetanus, and pertussis) reduced this figure by over 90%. However, waning immunity and incomplete vaccination schedules have led to resurgences in some regions. Pregnant women are advised to receive the Tdap vaccine during each pregnancy to pass antibodies to their newborns, who cannot be vaccinated until 2 months of age.
Polio, once a global scourge causing 350,000 cases of paralysis annually, has been reduced by 99.9% since 1988 due to the oral polio vaccine (OPV) and inactivated polio vaccine (IPV). The success of polio eradication efforts demonstrates the power of disease-specific interventions. Children require a series of 3–4 doses of IPV, starting at 2 months, to build full immunity. Despite challenges like vaccine hesitancy and accessibility, these examples illustrate how targeted vaccination programs can drastically reduce preventable deaths.
In summary, disease-specific preventable deaths reveal the profound impact of vaccines on global health. From smallpox eradication to the near-elimination of polio, these successes serve as a testament to the importance of continued vaccination efforts. Practical steps, such as adhering to recommended vaccine schedules and addressing gaps in access, are essential to sustain progress and protect future generations.
Vaccine Mandates: Ontario's Healthcare Worker Requirements
You may want to see also
Explore related products






![]()
Global vaccine impact statistics
Before the advent of vaccines, millions of lives were lost annually to preventable diseases. The introduction of global vaccination programs has dramatically shifted this landscape, saving an estimated 154 million lives over the past five decades, according to the World Health Organization (WHO). This staggering figure underscores the transformative impact of vaccines on global health, reducing mortality rates from diseases like measles, polio, and tetanus by over 99% in some regions.
Consider the case of smallpox, a disease that once claimed 300 million lives in the 20th century alone. Through a coordinated global vaccination campaign, smallpox was eradicated in 1980, marking the first and only time a human disease has been completely eliminated. This success story highlights the power of vaccines not just to prevent deaths but to eradicate entire diseases. Similarly, the measles vaccine has prevented an estimated 25.5 million deaths between 2000 and 2019, with a single dose offering 93% efficacy and two doses providing 97% protection.
However, the impact of vaccines extends beyond individual survival. Vaccination programs have also reduced the economic burden of healthcare systems by minimizing hospitalizations and long-term disabilities. For instance, the Haemophilus influenzae type b (Hib) vaccine has slashed meningitis cases in children by 70% in countries with high vaccination coverage, sparing families the financial and emotional toll of treating severe complications.
Despite these achievements, disparities in vaccine access persist. In low-income countries, only 1 in 5 children receive all recommended vaccines, compared to 1 in 2 in high-income nations. This gap underscores the need for equitable distribution and investment in global immunization efforts. Initiatives like Gavi, the Vaccine Alliance, have administered over 1 billion vaccine doses to children in the world’s poorest countries, demonstrating the potential for scalable solutions.
To maximize the impact of vaccines, practical steps include adhering to recommended dosage schedules, such as the 2-dose MMR (measles, mumps, rubella) series for children, and promoting community education to combat misinformation. Policymakers must also prioritize funding for vaccine research and infrastructure, ensuring that life-saving immunizations reach every corner of the globe. The data is clear: vaccines are one of humanity’s most powerful tools for preventing deaths and building a healthier future.
Add Your Digital Vaccine Record to Apple Wallet: A Quick Guide
You may want to see also
Explore related products






![]()
Historical pandemics and fatalities
Before the advent of vaccines, historical pandemics exacted staggering death tolls, often reshaping societies and economies. The 1918 Spanish Flu, for instance, claimed an estimated 50 million lives globally, with a mortality rate of 2.5%—far exceeding the typical seasonal flu rate of 0.1%. This pandemic disproportionately affected young adults aged 20–40, a demographic usually resilient to influenza, due to an overactive immune response known as a cytokine storm. Without vaccines or effective antiviral treatments, public health measures like quarantine and mask-wearing were the only defenses, though their implementation was inconsistent and often too late.
Contrast the Spanish Flu with the Justinian Plague of the 6th century, which killed an estimated 25–50 million people across the Byzantine Empire and Mediterranean region. Caused by the bacterium *Yersinia pestis*, this pandemic recurred in waves over two centuries, decimating up to half of the population in some areas. Unlike viral pandemics, bacterial infections like the plague could theoretically have been treated with antibiotics—had they existed. However, without such interventions, societies relied on isolation and rudimentary sanitation practices, which were largely ineffective in halting the spread.
The Black Death of the 14th century offers another grim example, killing approximately 75–200 million people, or 30–60% of Europe’s population. Transmitted by fleas on rats, this bubonic plague pandemic thrived in overcrowded, unsanitary conditions. Modern analysis suggests that a combination of quarantine, pest control, and, hypothetically, antibiotics could have mitigated its impact. Yet, in the absence of scientific understanding and medical tools, entire communities were left vulnerable, with death rates in some cities reaching 80%.
These historical pandemics underscore the preventable nature of millions of deaths before vaccines and modern medicine. For instance, smallpox, which killed 300 million people in the 20th century alone, was eradicated through global vaccination campaigns. Similarly, the 1957 Asian Flu and 1968 Hong Kong Flu pandemics, though deadly, had lower fatality rates than the Spanish Flu due to improved public health infrastructure and antiviral research. The lesson is clear: without vaccines, pandemics remain catastrophic, but with them, their impact can be drastically reduced.
To contextualize, consider that the COVID-19 pandemic, despite its severity, had a global mortality rate of approximately 1% due to rapid vaccine development and deployment. In contrast, the Spanish Flu’s 2.5% mortality rate in a less interconnected world resulted in far higher absolute deaths. This comparison highlights the transformative power of vaccines in preventing fatalities and underscores the urgency of equitable vaccine distribution in future pandemics. Historical pandemics serve as a stark reminder of what happens when societies lack the tools to fight infectious diseases—and a call to action to ensure such tools are accessible to all.
Smallpox Vaccine: Edward Jenner's Revolutionary Discovery
You may want to see also
Explore related products






![]()
Vaccine accessibility disparities
Before vaccines, millions of lives were lost annually to preventable diseases like smallpox, polio, and measles. The introduction of vaccines has drastically reduced these numbers, saving an estimated 2-3 million lives each year. However, the benefits of vaccines are not equally distributed. Vaccine accessibility disparities persist, leaving vulnerable populations at risk. In low-income countries, only 1 in 5 children receive all recommended vaccines, compared to 9 in 10 in high-income nations. This gap highlights a critical issue: the lifesaving potential of vaccines is hindered by inequitable access.
Consider the logistical challenges in remote areas. Cold chain requirements for vaccines, such as the measles vaccine needing storage between 2°C and 8°C, are difficult to maintain in regions without reliable electricity. Solar-powered refrigerators, though a solution, are costly and not universally available. Additionally, transportation hurdles in rural areas mean that even when vaccines are available, they may not reach those who need them most. For instance, a child in a remote village in sub-Saharan Africa is 5 times less likely to receive the full course of the diphtheria-tetanus-pertussis (DTP) vaccine compared to a child in an urban area.
Financial barriers further exacerbate disparities. While the Global Alliance for Vaccines and Immunisation (GAVI) provides subsidised vaccines to low-income countries, out-of-pocket costs for transportation, missed work, and ancillary fees can deter families from seeking immunisation. In India, for example, a study found that indirect costs associated with vaccination accounted for 50% of the total expense for rural families. This economic strain forces difficult choices, often resulting in delayed or forgone vaccinations.
Cultural and informational gaps also play a significant role. Misinformation about vaccine safety, fueled by social media and local myths, can lead to hesitancy. In Pakistan, polio eradication efforts have been hindered by conspiracy theories, resulting in ongoing transmission of the disease. Community health workers trained to address these concerns and provide accurate information are essential but often underfunded. A single trained worker can educate hundreds of families, yet many regions lack even one.
Addressing these disparities requires a multi-faceted approach. First, invest in infrastructure to strengthen cold chain systems and transportation networks. Second, eliminate indirect costs through financial incentives or waivers for families. Third, fund community health programs to combat misinformation and build trust. Finally, leverage technology, such as mobile clinics and digital tracking systems, to improve outreach and monitoring. By tackling these barriers, we can ensure that the lifesaving power of vaccines reaches everyone, regardless of geography or income.
Subcutaneous Vaccine Administration: Which Vaccines Should Be Given This Way?
You may want to see also
Frequently asked questions
Before vaccines, millions of deaths occurred annually from diseases like smallpox, polio, measles, and diphtheria. For example, smallpox alone caused an estimated 300 million deaths in the 20th century before its eradication through vaccination.
Diseases such as smallpox, polio, measles, pertussis (whooping cough), and tetanus were among the leading causes of preventable deaths before vaccines were developed and widely distributed.
Vaccines have drastically reduced mortality rates by preventing infections and complications from diseases. For instance, the measles vaccine alone has prevented over 25 million deaths between 2000 and 2018, according to the WHO.
Vaccines save an estimated 2-3 million lives every year, primarily by preventing deaths from diseases like measles, tetanus, and pertussis, according to global health organizations.
Smallpox vaccination led to the eradication of the disease in 1980, preventing millions of deaths annually. Before eradication, smallpox killed approximately 30% of those infected, with up to 500 million deaths in the 20th century alone.