The rollout of COVID-19 vaccines has been a monumental global effort, with billions of doses administered worldwide since the first vaccines became available in late 2020. As of recent data, over 13 billion doses have been administered globally, with varying vaccination rates across countries due to factors like access, infrastructure, and public acceptance. While many high-income nations have achieved high vaccination coverage, disparities persist in low- and middle-income countries, where vaccine distribution and hesitancy remain significant challenges. Tracking the number of people vaccinated is crucial for understanding the progress of immunization campaigns and their impact on public health, particularly in reducing severe illness, hospitalizations, and deaths.
Explore related products






What You'll Learn
![]()
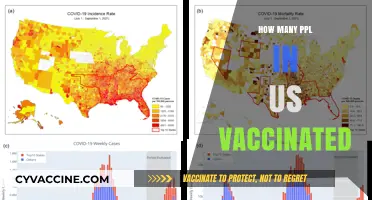
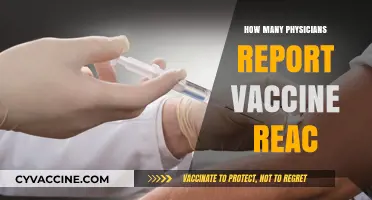
Global vaccination rates by country
As of the latest data, global vaccination rates vary dramatically by country, influenced by factors like healthcare infrastructure, economic status, and public trust in vaccines. For instance, high-income countries like Canada and the United Kingdom have administered booster doses to over 50% of their populations, while many low-income nations in Africa struggle to reach 20% full vaccination coverage. This disparity highlights the inequities in global vaccine distribution and access.
Analyzing the data reveals a clear correlation between a country’s GDP and its vaccination rate. Wealthier nations have not only secured larger vaccine supplies but have also implemented efficient distribution systems. For example, the United States has administered over 670 million doses, with 70% of its population fully vaccinated. In contrast, countries like Haiti and South Sudan have vaccinated less than 10% of their populations, often due to logistical challenges and limited resources. This gap underscores the need for global cooperation to address vaccine inequity.
From a practical standpoint, countries aiming to boost vaccination rates can learn from successful models. India’s CoWIN platform, a digital vaccine delivery system, has enabled the administration of over 2.2 billion doses, making it one of the largest vaccination drives globally. Similarly, Brazil’s mobile vaccination units have reached remote areas, increasing coverage among rural populations. These examples demonstrate that technology and innovative strategies can overcome barriers to vaccine access.
Persuasively, it’s critical to address vaccine hesitancy, which remains a significant obstacle in many countries. In France, for instance, initial skepticism led to slower uptake, but targeted campaigns featuring healthcare workers and simplified messaging helped increase full vaccination rates to over 75%. Countries struggling with hesitancy should invest in culturally sensitive communication strategies and engage local leaders to build trust. Without addressing this, even the most robust vaccine supplies will fall short of their potential impact.
Comparatively, the success of vaccination campaigns in Southeast Asia offers valuable lessons. Singapore, with 92% of its population fully vaccinated, stands out due to its clear communication, mandatory health passes, and incentives for vaccination. Meanwhile, the Philippines, with only 60% coverage, faced challenges like supply chain issues and public mistrust. This comparison emphasizes the importance of comprehensive planning, transparency, and adaptability in achieving high vaccination rates. By studying these regional differences, countries can tailor their approaches to maximize effectiveness.
Global Vaccination Leader: Which Country Tops the Immunization Chart?
You may want to see also
Explore related products






![]()
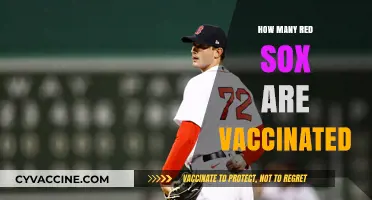
Age groups with highest vaccination coverage
As of recent data, older adults, particularly those aged 65 and above, consistently show the highest vaccination coverage across most countries. This trend is no accident; it’s the result of targeted public health campaigns emphasizing the heightened risk of severe illness and mortality from vaccine-preventable diseases in this demographic. For instance, during the COVID-19 pandemic, over 90% of individuals in this age group received at least one vaccine dose in countries like the U.S. and the U.K., compared to approximately 70% in the general population. This disparity highlights the success of tailored messaging and accessibility measures, such as mobile vaccination clinics and prioritized scheduling, aimed at seniors.
Analyzing the data further, the 50–64 age group often follows closely behind in vaccination rates, though with a noticeable drop-off. This cohort, often referred to as the "sandwich generation," balances caring for both children and aging parents, making them a critical bridge in community immunity. Vaccination campaigns targeting this group frequently emphasize not only personal health but also the protection of vulnerable family members. For example, flu vaccination rates in this age bracket typically hover around 60–70%, a figure that could improve with more workplace vaccination drives and family-centered incentives.
In contrast, younger age groups, particularly those aged 18–29, tend to lag in vaccination coverage, often due to perceived lower risk and competing priorities. However, exceptions exist, such as in college settings where vaccination mandates or on-campus clinics drive uptake. For instance, COVID-19 vaccination rates among college students surged to over 80% in institutions requiring proof of vaccination for enrollment. This example underscores the impact of structural incentives and convenience in boosting coverage among younger adults.
A comparative look at childhood vaccination rates reveals a different pattern. Children aged 5–11 often achieve high coverage, nearing 90% for routine immunizations like MMR, thanks to school entry requirements and pediatricians’ consistent recommendations. Yet, adolescents aged 12–17 show variability, particularly for newer vaccines like HPV or COVID-19, where parental hesitancy and lack of awareness play significant roles. Addressing this gap requires engaging both teens and their caregivers through school-based education and accessible, youth-friendly vaccination sites.
To maximize coverage across age groups, public health strategies must be age-specific and context-driven. For seniors, continue prioritizing accessibility and clear communication about risks. For middle-aged adults, leverage workplace programs and family-focused messaging. Among young adults, partner with educational institutions and use social media campaigns. Finally, for children and adolescents, strengthen school-based initiatives and involve parents in decision-making. By tailoring approaches to each group’s needs and behaviors, vaccination coverage can be optimized, ensuring broader community protection.
Vaccine Efficacy Against Double Mutant Variants: What You Need to Know
You may want to see also
Explore related products






![]()
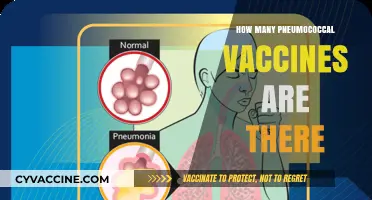
Vaccine distribution in rural vs urban areas
The COVID-19 pandemic highlighted stark disparities in vaccine distribution between rural and urban areas, with rural communities often lagging behind. Data from the CDC shows that as of late 2021, vaccination rates in rural counties were approximately 10-15% lower than in urban counties. This gap persists due to a combination of logistical challenges, limited healthcare infrastructure, and lower vaccine acceptance rates in rural populations. For instance, while urban areas often have multiple vaccination sites within a few miles, rural residents may need to travel over 50 miles to reach the nearest clinic, a significant barrier for those without reliable transportation.
Addressing this disparity requires tailored strategies. One effective approach is deploying mobile vaccination units to rural areas, which has been successfully implemented in states like Colorado and Kentucky. These units can administer vaccines at local community centers, churches, or even door-to-door, ensuring accessibility for elderly or immobile residents. Additionally, partnering with local pharmacies and clinics to offer walk-in appointments can increase convenience. For example, a single-dose vaccine like Johnson & Johnson’s was particularly beneficial in rural areas, as it eliminated the need for a follow-up visit, a critical factor for those with limited transportation options.
Another critical factor is building trust within rural communities, where vaccine hesitancy is often higher. Local leaders, including doctors, clergy, and educators, play a pivotal role in dispelling myths and encouraging vaccination. In Iowa, for instance, a campaign featuring trusted farmers and ranchers sharing their vaccination experiences significantly boosted uptake among agricultural communities. Providing clear, culturally relevant information—such as explaining that vaccines do not interfere with fertility or contain microchips—can address specific concerns prevalent in rural areas.
Despite these efforts, challenges remain. Rural healthcare facilities often lack the staffing and resources to manage large-scale vaccination campaigns. For example, a rural clinic in Montana reported receiving only 100 doses per week, insufficient to meet demand. To overcome this, federal and state governments must allocate additional funding and resources to these areas, including hiring temporary staff and providing refrigeration units for vaccine storage. Incentives such as gift cards or discounts at local businesses can also motivate hesitant individuals to get vaccinated.
In conclusion, bridging the rural-urban vaccine gap demands a multi-faceted approach: improving accessibility through mobile units and local partnerships, fostering trust via community leaders, and addressing resource shortages. By prioritizing these strategies, public health officials can ensure equitable vaccine distribution and protect vulnerable populations, regardless of their zip code. Practical steps, such as offering single-dose options and leveraging local influencers, can make a measurable difference in closing this gap.
Understanding the Four Key Tiers in Global Vaccination Strategies
You may want to see also
Explore related products

$11.93 $21.99





![]()
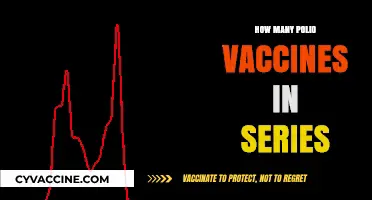
Impact of vaccine mandates on uptake
Vaccine mandates have been a polarizing tool in the effort to increase immunization rates, with their impact on uptake varying widely across regions and demographics. In countries like France, where a health pass system was implemented, vaccine uptake surged by over 20% within weeks of the mandate’s announcement. Similarly, in the U.S., states with stricter workplace vaccine requirements saw a 10-15% increase in fully vaccinated adults compared to states without such policies. These examples suggest that mandates can serve as a powerful catalyst, particularly among hesitant populations, by creating a sense of urgency and reducing the friction of decision-making. However, their effectiveness hinges on clear communication, equitable implementation, and the availability of accessible vaccination sites.
Consider the mechanics of how mandates influence behavior. For individuals, mandates often simplify complex decisions by framing vaccination as a necessity rather than a choice. For instance, a mandate requiring two doses of an mRNA vaccine for travel or employment removes ambiguity, prompting action. Employers, too, benefit from mandates by reducing workplace disruptions and healthcare costs. A study by the Kaiser Family Foundation found that companies with vaccine mandates reported a 90% vaccination rate among employees, compared to 72% in companies without such policies. Yet, mandates are not without challenges; they can provoke resistance, particularly in communities with historical mistrust of institutions. Balancing coercion with education is critical to ensuring mandates enhance rather than hinder long-term public health trust.
From a comparative perspective, the success of mandates often depends on the cultural and political context. In Singapore, where 92% of the population is fully vaccinated, mandates were paired with robust public health campaigns and incentives, creating a sense of collective responsibility. In contrast, countries like Sweden, which relied on voluntary vaccination, achieved high uptake through trust in public health authorities and a strong social contract. This highlights that mandates are most effective when they complement, rather than replace, community engagement and education. For policymakers, the takeaway is clear: mandates should be one tool in a multifaceted strategy, tailored to local needs and sensitivities.
Practical implementation of mandates requires careful consideration of exemptions and enforcement. Medical exemptions, for example, should be clearly defined, with guidelines specifying conditions like severe allergic reactions to polyethylene glycol, a component in some vaccines. Non-medical exemptions, such as religious or philosophical objections, must be balanced against public health goals. Enforcement mechanisms, whether fines or restricted access to public spaces, should be proportionate and transparent. For instance, Italy’s “Super Green Pass” system, which restricted unvaccinated individuals from restaurants and cultural venues, was paired with widespread testing options to ensure fairness. Such measures demonstrate that mandates can be both firm and flexible, maximizing uptake while minimizing alienation.
Ultimately, the impact of vaccine mandates on uptake is a delicate interplay of authority and autonomy. While they can rapidly increase vaccination rates, their success depends on addressing underlying hesitancy and ensuring equitable access. For individuals, understanding the rationale behind mandates—whether for personal protection or community immunity—can transform compliance into conviction. For societies, mandates serve as a reminder that public health is a shared responsibility, requiring both individual action and collective support. When designed thoughtfully, mandates are not just a tool for coercion but a pathway to resilience.
Live Attenuated Vaccines: Understanding Weakened Viruses in Immunization
You may want to see also
Explore related products






![]()
Side effects reported post-vaccination statistics
As of recent data, billions of people worldwide have received COVID-19 vaccines, with over 13 billion doses administered across various platforms. This massive rollout has been accompanied by rigorous monitoring of side effects, which are typically mild and transient. Common reactions include pain at the injection site, fatigue, headache, and muscle pain, usually resolving within a few days. However, the rarity of severe side effects has been a critical focus of post-vaccination surveillance systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the U.S. and the Yellow Card scheme in the U.K. These systems rely on voluntary reporting, which, while essential, can sometimes overrepresent or underrepresent certain events due to biases in submission.
Analyzing the data, the incidence of severe side effects is strikingly low. For instance, anaphylaxis, a severe allergic reaction, occurs in approximately 2 to 5 people per million doses administered, predominantly within 15–30 minutes post-vaccination. This has led to guidelines recommending a 15-minute observation period after vaccination, especially for individuals with a history of allergies. Another rare but significant side effect is thrombosis with thrombocytopenia syndrome (TTS), associated primarily with adenovirus vector vaccines like Johnson & Johnson’s Janssen. TTS occurs in about 7 per 1 million doses among women aged 18–49, emphasizing the importance of age- and sex-specific risk communication.
Comparatively, mRNA vaccines (Pfizer-BioNTech and Moderna) have shown a slightly higher risk of myocarditis and pericarditis, particularly in adolescent males and young men after the second dose. The incidence is approximately 10 to 40 cases per million doses, with symptoms typically appearing within a week post-vaccination. Most cases are mild and resolve with rest and anti-inflammatory medications. This has prompted some countries to extend the interval between doses or offer a single dose to younger age groups, balancing the risk of rare side effects against the benefits of protection.
Persuasively, the statistics underscore the importance of transparency and context in interpreting side effect data. While any adverse event is concerning, the risks must be weighed against the far greater dangers of COVID-19 itself, including hospitalization, long-term complications, and death. For example, the risk of myocarditis from COVID-19 infection is significantly higher than from vaccination, particularly in severe cases. Public health messaging should emphasize this comparative risk, ensuring informed decision-making without undue alarm.
Practically, individuals can take steps to monitor and manage post-vaccination symptoms effectively. Keeping a symptom diary for 7–14 days post-vaccination can help identify any unusual reactions. Mild symptoms can be alleviated with over-the-counter pain relievers like acetaminophen or ibuprofen, though these should be avoided prophylactically unless symptoms arise. For severe or persistent symptoms, such as difficulty breathing, chest pain, or facial swelling, immediate medical attention is crucial. Staying informed through reputable sources and following local health guidelines remains the best approach to navigating post-vaccination experiences safely.
Proving Your Booster Vaccination Status: A Step-by-Step Guide
You may want to see also
Frequently asked questions
As of the latest data, over 13 billion doses have been administered globally, with approximately 5.5 billion people receiving at least one dose.
Over 220 million people in the U.S. have been fully vaccinated, representing about 67% of the total population.
Approximately 68% of the world’s population has received at least one dose of a COVID-19 vaccine.
Globally, over 2 billion people have received a booster or additional dose, though rates vary significantly by country.
Yes, several low-income countries, particularly in Africa and parts of Asia, have vaccination rates below 20%, with limited access to vaccines.