The vaccination of the elderly population has been a critical focus in global health efforts, particularly in the wake of the COVID-19 pandemic. As one of the most vulnerable groups to severe illness and complications, ensuring high vaccination rates among the elderly is essential for reducing hospitalizations, deaths, and the overall burden on healthcare systems. Governments and health organizations worldwide have implemented targeted campaigns, mobile vaccination units, and outreach programs to increase accessibility and address hesitancy. While significant progress has been made, disparities in vaccination rates persist across regions, influenced by factors such as socioeconomic status, geographic location, and vaccine availability. Understanding the current vaccination coverage among the elderly is crucial for identifying gaps and tailoring strategies to protect this high-risk demographic effectively.
Explore related products






What You'll Learn
![]()
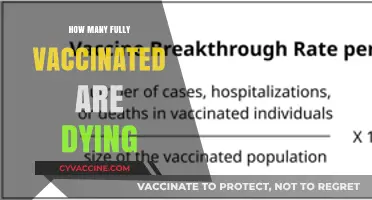
Vaccination rates by age group
Elderly populations, typically defined as individuals aged 65 and older, have been a primary focus of vaccination campaigns due to their heightened vulnerability to severe illness from infectious diseases like COVID-19. As of recent data, vaccination rates among this age group have shown significant progress globally, though disparities persist across regions and demographics. For instance, in the United States, over 90% of seniors have received at least one dose of a COVID-19 vaccine, with booster uptake slightly lower at around 70%. These figures highlight both the success of targeted outreach efforts and the ongoing need to address hesitancy and access barriers.
Analyzing vaccination rates by age group reveals a clear trend: older adults consistently outpace younger cohorts in vaccine acceptance and completion. This phenomenon can be attributed to several factors, including higher risk perception, stronger adherence to public health recommendations, and more efficient healthcare access. For example, in the European Union, vaccination coverage for those aged 70–79 often exceeds 90%, compared to 60–70% in the 25–49 age bracket. However, within the elderly group itself, there are nuances. Those aged 80 and above sometimes lag slightly behind their younger counterparts due to mobility challenges, cognitive barriers, or living in long-term care facilities with inconsistent vaccine delivery systems.
To improve vaccination rates among the elderly, practical steps can be implemented. First, mobile vaccination clinics should be deployed to residential communities, senior centers, and long-term care facilities to eliminate transportation barriers. Second, clear, culturally sensitive communication about vaccine safety and efficacy is essential, particularly for addressing misinformation. Third, involving trusted figures like local doctors or community leaders in outreach efforts can enhance trust and participation. For instance, in Japan, leveraging local physicians to endorse vaccines led to a 10% increase in uptake among seniors within three months.
A comparative analysis of global vaccination trends underscores the impact of policy and infrastructure on elderly vaccination rates. Countries with robust healthcare systems and proactive policies, such as Israel and Singapore, achieved near-universal coverage among seniors early in the COVID-19 vaccine rollout. In contrast, low-income nations with limited resources and fragmented healthcare systems often report rates below 50% for this age group. This disparity highlights the need for international collaboration to ensure equitable vaccine distribution and support for logistical challenges in underserved regions.
Finally, while high vaccination rates among the elderly are encouraging, maintaining immunity through booster doses remains critical. Health authorities recommend that seniors receive additional doses every 6–12 months, depending on local guidelines and circulating variants. Practical tips for caregivers and family members include scheduling reminders, assisting with transportation, and monitoring for side effects post-vaccination. By sustaining these efforts, societies can continue to protect their most vulnerable populations and reduce the overall burden of vaccine-preventable diseases.
Pneumococcal Vaccine Frequency for Older Adults: What's Recommended?
You may want to see also
Explore related products






![]()
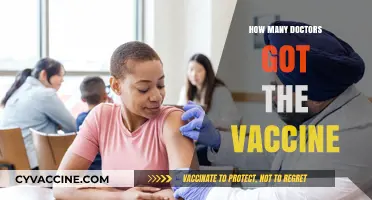
Regional elderly vaccination coverage
Elderly vaccination rates vary significantly across regions, influenced by factors like healthcare infrastructure, vaccine availability, and cultural attitudes. For instance, as of late 2023, Europe reported that over 85% of individuals aged 65 and older had received at least one dose of a COVID-19 vaccine, with countries like Portugal and Spain leading at over 95% coverage. In contrast, parts of Africa and Southeast Asia lag behind, with rates often below 50% due to supply chain challenges and vaccine hesitancy. These disparities highlight the need for targeted strategies to improve global equity in elderly vaccination.
Analyzing regional trends reveals that high-income countries have consistently outpaced low-income nations in vaccinating their elderly populations. In North America, the U.S. and Canada achieved over 90% coverage among those aged 70 and above, thanks to robust distribution networks and public awareness campaigns. Meanwhile, in South Asia, countries like India and Bangladesh have struggled to reach even 70% coverage in the same age group, despite having large elderly populations. This gap underscores the importance of international collaboration to address resource limitations and logistical hurdles.
Practical steps can be taken to improve regional elderly vaccination coverage. First, governments should prioritize dose allocation to rural and underserved areas, where access is often limited. Second, mobile vaccination clinics can be deployed to reach homebound seniors, as seen in successful initiatives in Brazil and Mexico. Third, community health workers can play a crucial role in dispelling myths and encouraging vaccine uptake, particularly in regions with high hesitancy. For example, in sub-Saharan Africa, local leaders have been instrumental in increasing trust and participation.
Comparing regional strategies offers valuable lessons. In East Asia, countries like Japan and South Korea achieved high elderly vaccination rates by combining mandatory registration systems with incentives like priority access to healthcare services. Conversely, some European nations relied on voluntary participation but bolstered efforts with multilingual campaigns and accessible vaccination sites. These approaches demonstrate that cultural sensitivity and tailored solutions are key to overcoming regional challenges.
Finally, monitoring and adapting strategies based on real-time data is essential. For instance, regions with lower coverage should track vaccination rates by age subgroups (e.g., 65-74 vs. 75+) to identify specific barriers. Booster dose administration, particularly for mRNA vaccines requiring two initial doses followed by periodic boosters, must also be prioritized to maintain immunity. By learning from regional successes and addressing local needs, global efforts can ensure that elderly populations everywhere receive the protection they need.
Where to Get Yellow Fever Vaccination in Conroe: Top Location
You may want to see also
Explore related products






![]()
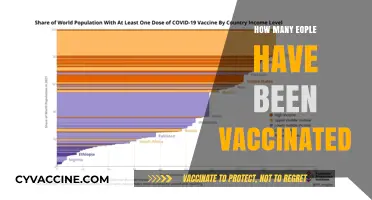
Vaccine type distribution among seniors
The distribution of vaccine types among seniors varies significantly across regions, influenced by factors such as availability, national health policies, and clinical recommendations. For instance, in the United States, the majority of seniors aged 65 and older have received mRNA vaccines, specifically Pfizer-BioNTech or Moderna, due to their high efficacy and early approval. These vaccines require a primary series of two doses, administered 3–4 weeks apart, followed by booster shots to maintain immunity. In contrast, countries like the United Kingdom have also utilized the Oxford-AstraZeneca vaccine, a viral vector-based option, particularly in earlier phases of their vaccination campaigns. Understanding these regional differences is crucial for assessing global vaccination strategies and their impact on elderly populations.
From an analytical perspective, the choice of vaccine type for seniors often hinges on safety profiles and efficacy in older adults. mRNA vaccines have demonstrated over 90% efficacy in preventing severe COVID-19 in clinical trials involving participants aged 65 and above. However, some seniors with specific medical conditions, such as severe allergies to vaccine components, may require alternative options like the Novavax vaccine, a protein subunit vaccine approved in certain countries. Healthcare providers must weigh these factors when recommending vaccines, ensuring both safety and optimal protection for this vulnerable demographic.
For those involved in administering vaccines to seniors, practical considerations are key. For example, the storage requirements of vaccine types play a significant role in distribution. mRNA vaccines like Pfizer require ultra-cold storage (-70°C), which can pose logistical challenges in rural or under-resourced areas. In such cases, vaccines like Moderna, which can be stored at standard freezer temperatures (-20°C), or single-dose options like Johnson & Johnson, may be more feasible. Additionally, ensuring clear communication about dosage intervals and booster schedules is essential to maximize vaccine effectiveness in this age group.
A comparative analysis reveals that while mRNA vaccines dominate in many Western countries, other regions have adopted diverse strategies. For instance, China has primarily administered inactivated virus vaccines like Sinovac and Sinopharm to its elderly population, with a focus on accessibility and ease of distribution. Meanwhile, some European countries have shifted to heterologous prime-boost strategies, combining different vaccine types (e.g., AstraZeneca followed by an mRNA booster) to enhance immune responses. These variations highlight the importance of tailoring vaccine distribution to local contexts and available resources.
Finally, seniors and their caregivers can take proactive steps to navigate vaccine type distribution effectively. First, stay informed about the vaccines available in your region and their specific recommendations for older adults. Second, consult healthcare providers to determine the most suitable vaccine based on individual health conditions and medical history. Third, keep track of booster schedules, as immunity wanes over time, particularly in seniors. By staying informed and proactive, elderly individuals can ensure they receive the most appropriate vaccine type for their needs, maximizing protection against severe illness.
Billing for Pneumonia Vaccines: A Guide to NY Medicaid Claims
You may want to see also
Explore related products






![]()
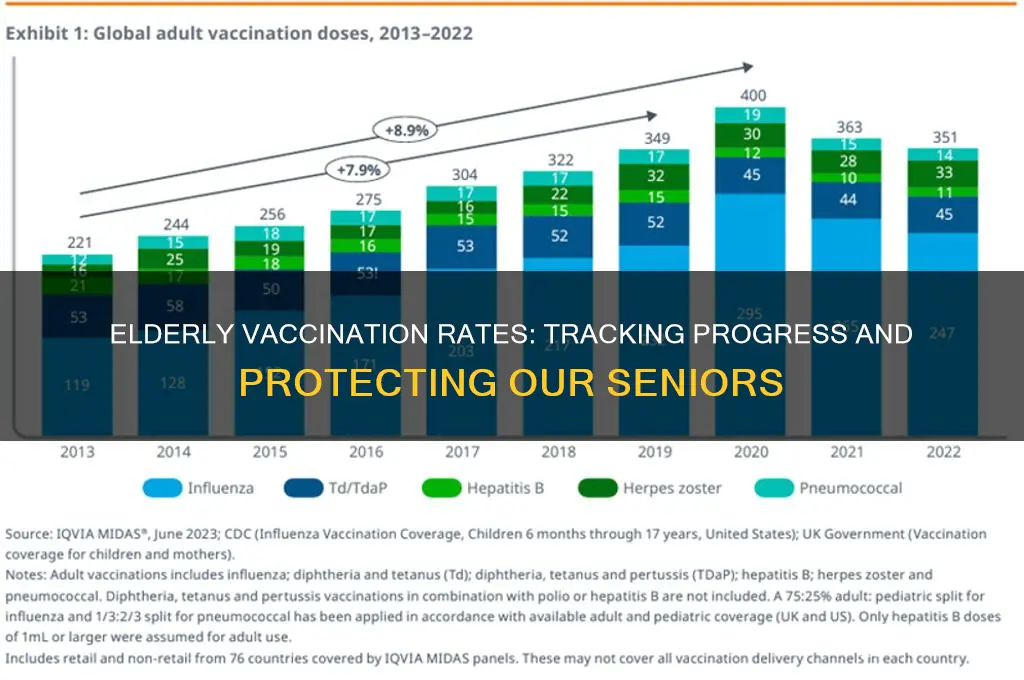
Challenges in elderly vaccination access
Elderly vaccination rates have climbed significantly since the onset of the COVID-19 pandemic, yet disparities persist. As of recent data, over 85% of individuals aged 65 and older in developed countries have received at least one dose, with booster uptake hovering around 70%. However, these figures mask critical access challenges that leave vulnerable seniors behind. Rural communities, for instance, often report rates 10-15% lower than urban areas due to logistical barriers, highlighting the need for targeted interventions.
One of the most pressing challenges is geographic isolation. Seniors in rural areas frequently face distances of 50 miles or more to reach vaccination sites, a hurdle exacerbated by limited public transportation. Mobile clinics have emerged as a solution, but their reach remains inconsistent. For example, a pilot program in Montana increased rural vaccination rates by 12% within six months, demonstrating the impact of localized efforts. Policymakers must prioritize funding for such initiatives, ensuring they are equipped with refrigerated storage for vaccines requiring 2-8°C, like Pfizer’s, or those stable at room temperature, such as Johnson & Johnson’s.
Another barrier is technological exclusion, particularly for those aged 80 and above. Online registration systems, often the primary method for scheduling appointments, alienate seniors who lack internet access or digital literacy. In the UK, 40% of individuals over 75 do not use the internet, forcing them to rely on overwhelmed phone lines or family assistance. Governments should implement hybrid systems, such as community-based registration drives or paper sign-ups at local pharmacies, ensuring no one is left behind due to a digital divide.
Health literacy and misinformation further complicate access. Studies show that 30% of seniors in low-income areas express vaccine hesitancy, often fueled by myths about side effects or efficacy. Tailored educational campaigns, delivered through trusted sources like primary care physicians or local religious leaders, can address these concerns. For instance, emphasizing that common side effects—such as fatigue or mild fever—typically resolve within 48 hours post-vaccination can alleviate fears. Pairing education with accessible, walk-in clinics during weekends or evenings could significantly improve uptake.
Finally, physical and cognitive limitations pose unique challenges. Seniors with mobility issues or dementia require assistance that standard vaccination sites often lack. Home-based vaccination programs, though resource-intensive, have proven effective in countries like Israel, where they contributed to a 90% vaccination rate among homebound individuals. Training healthcare workers to administer doses in residential settings, including proper handling of multi-dose vials and single-dose administration, is essential. Additionally, caregivers should be educated on post-vaccination monitoring, such as observing for rare but serious reactions like anaphylaxis, which requires immediate epinephrine intervention.
Addressing these challenges demands a multi-faceted approach, combining logistical innovation, inclusivity, education, and personalized care. By dismantling these barriers, societies can ensure that elderly vaccination access is equitable, not just statistically impressive.
Sputnik V Vaccine Registration Guide for Hyderabad Residents
You may want to see also
Explore related products



![]()
Booster dose uptake in older adults
As of recent data, booster dose uptake among older adults has shown variability across regions, with factors like accessibility, awareness, and hesitancy influencing participation. In the United States, for instance, over 70% of adults aged 65 and older have received at least one booster dose, according to the CDC. However, this figure drops significantly in some low-income countries, where logistical challenges and vaccine supply constraints limit coverage. Understanding these disparities is crucial for tailoring interventions to improve booster uptake in this vulnerable population.
Analyzing the reasons behind booster hesitancy in older adults reveals a complex interplay of concerns. Some individuals worry about side effects, despite clinical trials demonstrating that booster doses are safe and well-tolerated, with common reactions limited to mild fatigue, headache, or soreness at the injection site. Others may mistakenly believe their initial vaccine series provides sufficient protection, overlooking the waning immunity observed 6–8 months post-vaccination. Addressing these misconceptions through clear, evidence-based communication is essential to encourage timely booster administration.
Practical steps can significantly enhance booster dose uptake among older adults. First, healthcare providers should proactively reach out to eligible individuals, using reminders via phone calls, emails, or postal mail. Mobile vaccination clinics and home-visit programs can overcome mobility barriers for those with limited access to transportation. Second, family members and caregivers play a pivotal role in encouraging vaccination by discussing its benefits and accompanying older adults to appointments. Lastly, integrating booster reminders into routine healthcare visits, such as annual flu shots or chronic disease management, can streamline the process and increase compliance.
Comparing booster uptake trends across age subgroups within the elderly population highlights opportunities for targeted strategies. While those aged 75–84 often show higher uptake rates due to increased awareness of health risks, the 65–74 age group may exhibit lower participation, possibly due to a perception of lower vulnerability. Tailored messaging that resonates with each subgroup—such as emphasizing independence and quality of life for younger seniors—can bridge this gap. Additionally, leveraging community leaders and peer influencers can foster trust and motivate action in hesitant populations.
In conclusion, boosting booster dose uptake in older adults requires a multifaceted approach that addresses barriers, dispels myths, and leverages practical solutions. By focusing on accessibility, education, and personalized outreach, stakeholders can ensure this critical demographic remains protected against evolving health threats. With over 50% of COVID-19 deaths occurring in individuals aged 65 and older, the stakes are high—making every effort to increase booster coverage a matter of urgent public health priority.
Does Tdap Vaccine Protect Against Tetanus? Understanding Its Benefits
You may want to see also
Frequently asked questions
As of the latest data, over 80% of individuals aged 65 and older worldwide have received at least one dose of a COVID-19 vaccine, though rates vary by country.
In the United States, approximately 95% of adults aged 65 and older have received at least one dose of a COVID-19 vaccine, with over 70% receiving a booster dose.
No, vaccination rates among the elderly vary significantly by country. High-income countries generally report higher rates (over 80%), while low-income countries often have much lower rates (below 50%).
COVID-19 vaccines are highly effective in reducing severe illness, hospitalization, and death among the elderly, with studies showing over 90% efficacy in preventing severe outcomes in this age group.