As of the latest global health reports, the number of people vaccinated against COVID-19 has surpassed 13 billion doses administered worldwide, marking a significant milestone in the fight against the pandemic. This figure reflects the collective efforts of governments, healthcare organizations, and communities to curb the spread of the virus and protect populations. While vaccination rates vary widely across regions, with some countries achieving high coverage and others facing challenges such as vaccine hesitancy, supply chain issues, and infrastructure limitations, the global vaccination campaign has undoubtedly saved millions of lives and reduced the severity of infections. Monitoring vaccination numbers remains crucial for assessing progress, identifying disparities, and guiding future public health strategies to ensure equitable access and sustained immunity.
Explore related products






What You'll Learn
![]()
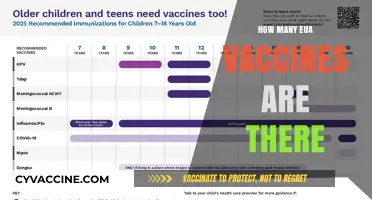
Global vaccination rates by region
As of the latest data, global vaccination rates vary significantly by region, reflecting disparities in healthcare infrastructure, economic resources, and policy priorities. North America and Europe lead with vaccination rates exceeding 70% for at least one dose, driven by robust distribution networks and public health campaigns. In contrast, Africa lags behind, with only about 25% of its population receiving at least one dose, due to limited vaccine supply and logistical challenges. These regional differences highlight the need for targeted global efforts to ensure equitable access to vaccines.
Analyzing the data reveals that high-income regions have not only secured larger vaccine stocks but also administered booster doses more effectively. For instance, over 50% of the eligible population in North America and Europe has received booster shots, compared to less than 10% in many low-income countries. This gap underscores the importance of dose-sharing initiatives like COVAX, which aims to distribute vaccines to underserved regions. However, COVAX has faced challenges in meeting its targets, emphasizing the need for wealthier nations to accelerate donations and support local manufacturing capabilities in low-resource settings.
Instructively, regions like Southeast Asia and Latin America offer valuable lessons in balancing limited resources with effective vaccination strategies. Countries like India and Brazil have leveraged local vaccine production to increase coverage, with India administering over 2 billion doses domestically. These examples demonstrate that regional manufacturing hubs can play a critical role in scaling up vaccine access. For policymakers, investing in such infrastructure and fostering international collaborations could be key to bridging the global vaccination gap.
Persuasively, the disparity in vaccination rates is not just a health issue but a moral and economic imperative. Unvaccinated populations remain vulnerable to outbreaks, which can lead to new variants that threaten global progress. For instance, the Omicron variant emerged in regions with low vaccination rates, underscoring the interconnectedness of global health. Prioritizing equitable vaccine distribution is not only ethically sound but also economically prudent, as it reduces the risk of prolonged pandemics and associated costs.
Comparatively, the success of vaccination campaigns in the Middle East and parts of Asia highlights the impact of strong government mandates and public trust. Countries like the UAE and Singapore achieved over 90% vaccination rates through mandatory policies and efficient rollout plans. In contrast, regions with lower trust in government or health systems, such as parts of Eastern Europe and Africa, have struggled to reach similar levels. Building public confidence through transparent communication and community engagement is essential for improving uptake in these areas.
Descriptively, the global vaccination landscape is a patchwork of progress and stagnation. While some regions approach herd immunity, others remain far behind, creating a fragile equilibrium. Practical steps to address this include simplifying vaccine delivery in remote areas, using mobile clinics, and providing multilingual information to diverse populations. For individuals, staying informed about local vaccination drives and encouraging eligible family members to get vaccinated can contribute to collective immunity. The goal is clear: a globally coordinated effort to ensure that no region is left behind in the fight against pandemics.
Mormon Vaccine Beliefs: Exploring LDS Church Stance on Vaccinations
You may want to see also
Explore related products






![]()
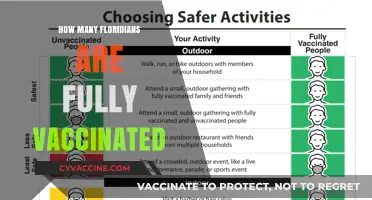
Vaccination trends over time (2020-2023)
The global vaccination campaign against COVID-19 began in December 2020, marking a pivotal moment in the fight against the pandemic. By the end of 2020, just over 1 million doses had been administered worldwide, primarily to healthcare workers and high-risk individuals in a handful of countries. This initial rollout was slow and uneven, constrained by limited vaccine supply and logistical challenges. However, it laid the groundwork for an unprecedented scale-up in 2021, as more vaccines received emergency approvals and production ramped up.
In 2021, vaccination rates accelerated dramatically, with over 8.5 billion doses administered globally by year-end. This surge was driven by the widespread availability of vaccines like Pfizer-BioNTech, Moderna, and AstraZeneca, as well as the introduction of single-dose options like Johnson & Johnson. Many countries implemented phased rollouts, prioritizing elderly populations, frontline workers, and those with comorbidities. For instance, the U.S. administered over 200 million doses by May 2021, with a focus on two-dose regimens requiring a 3- to 4-week interval. Despite this progress, disparities emerged, with high-income countries securing the majority of doses while low-income nations struggled to access supplies.
By 2022, the focus shifted to booster doses and vaccinating younger age groups. Over 12.5 billion doses had been administered globally, and many countries began offering third and even fourth doses to maintain immunity against emerging variants. For example, the CDC recommended boosters for individuals aged 12 and older, with a 5-month interval after the initial series. Pediatric vaccinations also gained momentum, with the Pfizer vaccine approved for children as young as 5 years old in many regions. However, vaccine hesitancy and misinformation became significant barriers, slowing uptake in some communities.
In 2023, the vaccination landscape has stabilized, with over 13 billion doses administered globally. The emphasis is now on sustaining immunity through annual boosters, similar to influenza vaccination campaigns. Practical tips for individuals include scheduling boosters during seasonal campaigns, staying informed about variant-specific vaccines, and ensuring children complete their primary series. While the pace of vaccination has slowed, ongoing efforts are critical to preventing future outbreaks and reducing the burden on healthcare systems. The trends from 2020 to 2023 highlight both the achievements and challenges of global vaccination efforts, offering lessons for future public health initiatives.
Vaccines: Empowering Our Immune System to Combat Pathogens Effectively
You may want to see also
Explore related products






![]()
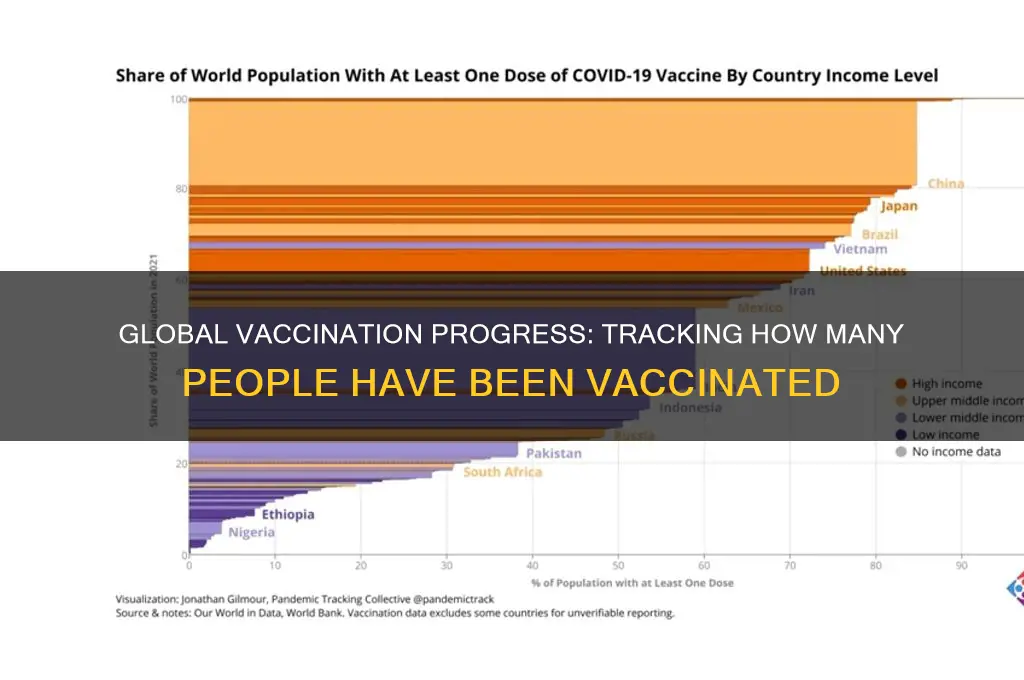
Age group distribution of vaccinated individuals
The age distribution of vaccinated individuals varies significantly across regions, influenced by factors like vaccine availability, prioritization strategies, and population demographics. In many countries, initial vaccine rollouts targeted older adults due to their higher risk of severe COVID-19 outcomes. For instance, in the United States, as of late 2023, over 90% of individuals aged 65 and older had received at least one vaccine dose, compared to approximately 70% of those aged 18-29. This disparity highlights the success of targeted campaigns but also underscores gaps in younger age groups.
Analyzing global trends reveals a stark divide between high-income and low-income countries. In wealthier nations, vaccination rates among older adults often exceed 80%, while younger populations lag slightly but still achieve moderate coverage. Conversely, in low-income regions, vaccine distribution remains uneven, with older adults and younger age groups alike facing significant barriers to access. For example, in sub-Saharan Africa, only about 30% of individuals over 60 have received a full vaccine series, compared to less than 20% of those aged 18-40. This disparity is compounded by limited healthcare infrastructure and vaccine hesitancy.
From a practical standpoint, understanding age distribution is crucial for tailoring public health strategies. For younger age groups, creative approaches such as pop-up vaccination clinics at schools, universities, and workplaces can improve accessibility. Additionally, addressing misinformation through targeted campaigns can boost confidence in vaccines among hesitant younger individuals. For older adults, ensuring easy access to booster doses and providing clear guidance on dosage intervals (e.g., a second booster 4-6 months after the first) remains essential to maintaining immunity.
Comparatively, countries with successful vaccination programs often share common strategies: prioritizing high-risk age groups first, leveraging digital platforms for appointment scheduling, and engaging community leaders to build trust. For instance, Israel’s rapid rollout achieved over 95% vaccination coverage in those over 60 by combining early procurement, efficient distribution, and public awareness campaigns. Such examples offer actionable insights for regions aiming to improve age-specific vaccination rates.
In conclusion, the age group distribution of vaccinated individuals reflects both successes and challenges in global vaccination efforts. By focusing on targeted strategies, addressing access barriers, and combating hesitancy, public health initiatives can work toward more equitable coverage across all age groups. Practical steps, such as localized outreach and clear communication, are key to bridging existing gaps and ensuring widespread protection.
Influenza Vaccine Out of Fridge: Immediate Steps to Take
You may want to see also
Explore related products

$16.86 $16.95





![]()
Vaccine types and their uptake rates
As of recent data, over 13 billion COVID-19 vaccine doses have been administered globally, yet the distribution and uptake of vaccine types vary widely. mRNA vaccines, such as Pfizer-BioNTech and Moderna, dominate in high-income countries, with uptake rates exceeding 70% in populations aged 12 and older. These vaccines require two primary doses, spaced 3–4 weeks apart, followed by boosters every 6–12 months for sustained immunity. Their high efficacy (90–95% against severe disease) and rapid development have made them a cornerstone of pandemic response, though cold chain requirements limit accessibility in low-resource settings.
In contrast, viral vector vaccines like Oxford-AstraZeneca and Johnson & Johnson have been pivotal in low- and middle-income countries due to their lower cost and easier storage. AstraZeneca’s vaccine, administered in a two-dose regimen 8–12 weeks apart, has been widely adopted in Europe, Africa, and parts of Asia, with uptake rates ranging from 40–60% in eligible populations. Johnson & Johnson’s single-dose approach offers convenience, particularly in hard-to-reach areas, but its uptake has been tempered by rare side effects, such as thrombosis with thrombocytopenia syndrome (TTS).
Protein subunit vaccines, exemplified by Novavax, emerged later but offer a familiar technology, appealing to those hesitant about newer platforms. Approved in over 40 countries, Novavax’s two-dose series (3 weeks apart) has seen moderate uptake, particularly among individuals preferring traditional vaccine methods. Its efficacy (90% against symptomatic disease) and lack of severe side effects position it as a viable alternative, though its rollout has been slower due to production delays and competition from established vaccines.
Inactivated vaccines, such as Sinopharm and Sinovac, are predominant in China and many developing nations, with billions of doses administered. These vaccines, requiring two doses 2–4 weeks apart, have uptake rates exceeding 80% in some regions. However, their lower efficacy (50–80% depending on strain) has necessitated additional doses or heterologous boosting strategies. Their affordability and stability at standard refrigeration temperatures make them critical for mass immunization campaigns in resource-constrained settings.
Practical considerations for vaccine uptake include age-specific recommendations, such as Pfizer’s authorization for children as young as 6 months, and tailored dosing for immunocompromised individuals, who may require three primary doses plus boosters. Public health strategies, like mobile clinics and workplace vaccination drives, have proven effective in boosting uptake, particularly in underserved communities. As new variants emerge, monitoring vaccine effectiveness and adapting formulations will be essential to sustain global immunization efforts.
Rotavirus Vaccine Spit-Up: What Parents Need to Know
You may want to see also
Explore related products






![]()
Impact of booster doses on total vaccinated numbers
Booster doses have significantly altered the landscape of vaccination statistics, introducing a new layer of complexity to the question of "how many people have been vaccinated." Initially, vaccination numbers were straightforward, reflecting the percentage of the population that had received a primary series (typically one or two doses). However, the introduction of boosters—additional doses administered months after the initial series—has shifted the metric from a binary "vaccinated/unvaccinated" to a spectrum of protection levels. For instance, as of late 2023, over 60% of the U.S. population had received at least one booster dose, but this figure varies widely by age group, with seniors over 65 leading at nearly 80% uptake compared to 40% among 18-29-year-olds. This disparity highlights how booster doses not only inflate total vaccination numbers but also create a tiered system of immunity within the population.
Analyzing the impact of boosters requires distinguishing between *cumulative doses* and *fully vaccinated individuals*. A person who has received three doses (two primary + one booster) contributes to both the total dose count and the "fully vaccinated" statistic, but their inclusion in the latter category depends on evolving definitions. For example, some countries now define "fully vaccinated" as having received a booster within the past six months, effectively excluding those whose immunity has waned. This dynamic means that while total doses administered may rise steadily, the "fully vaccinated" percentage can fluctuate, complicating public health messaging. In Israel, for instance, the rollout of a fourth dose for high-risk groups temporarily boosted total vaccination numbers but left policymakers debating whether to redefine "fully vaccinated" yet again.
From a practical standpoint, administering booster doses presents logistical challenges that influence vaccination numbers. Unlike the initial rollout, which prioritized mass vaccination sites, boosters often require targeted outreach to specific demographics—such as older adults or immunocompromised individuals—who may face barriers to access. For example, mobile clinics and home visits have become essential tools in the U.S. to reach homebound seniors, but these efforts are resource-intensive and unevenly implemented. Additionally, the timing of booster campaigns matters: a well-coordinated drive, like France’s winter 2022 campaign linking boosters to COVID health passes, can rapidly increase numbers, while delayed or fragmented efforts may stall progress.
Persuasively, the case for boosters rests on their ability to sustain population-level immunity, but their impact on vaccination numbers also underscores the need for clarity in communication. When booster doses are framed as optional or contingent on risk factors, uptake slows, and total vaccinated numbers plateau. Conversely, countries that integrate boosters into routine immunization schedules—such as annual flu shots—see steadier growth. For instance, Portugal’s approach of offering boosters alongside seasonal vaccines resulted in a 15% increase in total doses within three months. This strategy not only boosts numbers but also normalizes the concept of ongoing vaccination, setting a precedent for future public health initiatives.
In conclusion, booster doses have transformed vaccination metrics from a simple count to a dynamic, multi-dimensional measure of immunity. Their impact on total vaccinated numbers depends on factors ranging from policy definitions to logistical execution and public perception. As vaccination campaigns evolve, tracking not just doses but also their distribution and efficacy will be crucial. For individuals, staying informed about booster recommendations—such as the CDC’s guidance for a bivalent booster at least two months after the last dose—ensures both personal protection and contribution to collective immunity. Ultimately, boosters are not just additional shots but a critical tool in maintaining the momentum of global vaccination efforts.
Exploring Fungal Infections: Are There Vaccines to Combat Fungi?
You may want to see also
Frequently asked questions
As of 2023, over 13 billion COVID-19 vaccine doses have been administered globally, with more than 5 billion people receiving at least one dose.
Countries like Portugal, Singapore, and the United Arab Emirates have some of the highest vaccination rates, with over 90% of their populations fully vaccinated.
As of 2023, over 270 million people in the United States have received at least one dose of a COVID-19 vaccine.
Approximately 65% of the global population has been fully vaccinated against COVID-19, though rates vary significantly by region.
As of 2023, over 500 million children and adolescents (aged 5–18) have received at least one dose of a COVID-19 vaccine globally.