Childhood vaccinations are a cornerstone of public health, protecting children from a range of serious and potentially life-threatening diseases. The number of recommended childhood vaccinations varies by country and healthcare guidelines, but in the United States, the Centers for Disease Control and Prevention (CDC) advises a comprehensive schedule that typically includes vaccines for diseases such as measles, mumps, rubella, polio, whooping cough, tetanus, diphtheria, hepatitis B, chickenpox, and influenza, among others. Altogether, children may receive up to 14 different vaccines by the age of 6, often administered in multiple doses to ensure full immunity. These vaccinations not only safeguard individual children but also contribute to herd immunity, reducing the spread of infectious diseases within communities. Understanding the full scope of childhood vaccinations is essential for parents and caregivers to make informed decisions about their child’s health and well-being.
Explore related products






What You'll Learn
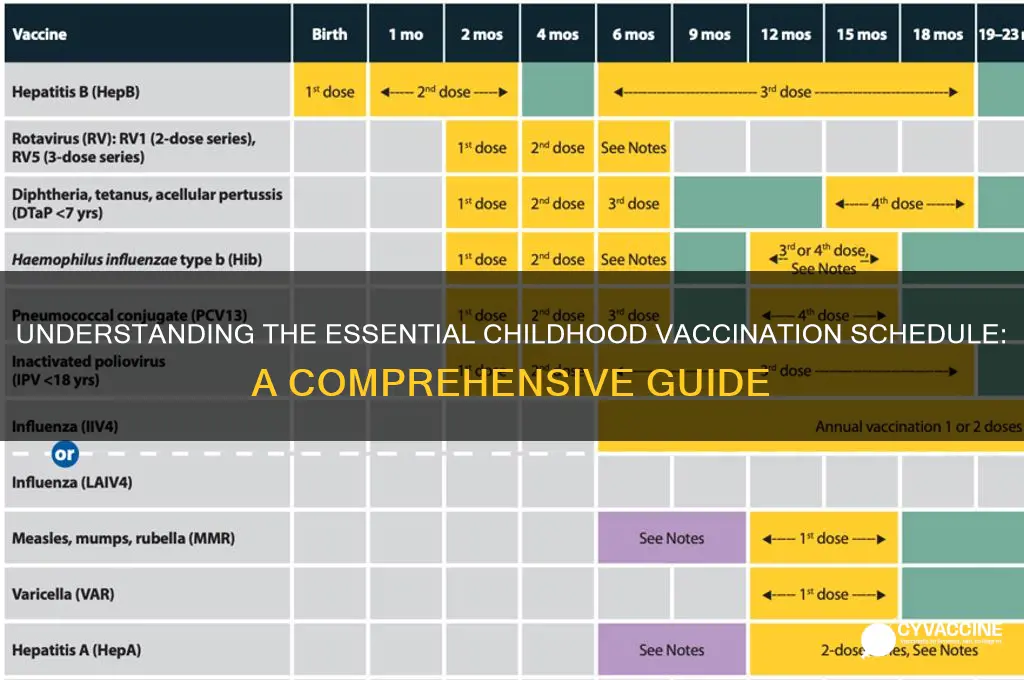
- Vaccine Schedule Overview: Standard timeline for childhood vaccinations from birth to adolescence
- Mandatory vs. Optional: Vaccines required by law versus those recommended but not compulsory
- Common Childhood Vaccines: List of vaccines like MMR, DTaP, and polio
- Vaccine Combinations: How multiple vaccines are often combined into single shots for efficiency
- Global Variations: Differences in vaccination counts and schedules across countries
![]()
Vaccine Schedule Overview: Standard timeline for childhood vaccinations from birth to adolescence
Childhood vaccinations are a cornerstone of public health, protecting against serious diseases and ensuring community immunity. The standard vaccine schedule is meticulously designed to provide immunity when children are most vulnerable, balancing safety and efficacy. From birth to adolescence, this timeline is a critical roadmap for parents and healthcare providers alike.
Birth to 2 Months: The journey begins within hours of life. Newborns receive their first dose of the Hepatitis B (HepB) vaccine, safeguarding against a virus that can cause chronic liver disease. This initial dose is a proactive step, often administered before leaving the hospital. At 1 to 2 months, the schedule expands to include the first doses of essential vaccines: DTaP (Diphtheria, Tetanus, Pertussis), RV (Rotavirus), Hib (Haemophilus influenzae type b), PCV13 (Pneumococcal conjugate), and IPV (Inactivated Poliovirus). Each of these vaccines targets specific pathogens, from the whooping cough-causing pertussis to the potentially deadly pneumococcal bacteria. Parents should be aware that some vaccines, like RV, are administered orally, while others are given as injections, typically in the thigh muscle for infants.
4 to 6 Months: As infants grow, so does their vaccine schedule. This period is marked by booster doses to reinforce immunity. The second doses of DTaP, Hib, PCV13, and IPV are administered, along with the second dose of RV. Additionally, the first dose of the Influenza vaccine may be introduced during flu season, emphasizing the importance of annual protection against this ever-evolving virus. It's crucial for caregivers to monitor for mild side effects like fever or soreness at the injection site, which are normal immune responses.
6 Months to 18 Months: This phase introduces new vaccines and continues the booster series. At 6 months, the third dose of DTaP, Hib, and PCV13 is given, along with the first dose of the MMR (Measles, Mumps, Rubella) vaccine, a critical defense against highly contagious diseases. The HepB series is completed with the third dose, and the annual flu vaccine continues to be a priority. By 12-15 months, children receive the fourth dose of Hib and PCV13, ensuring robust protection. This period also includes the introduction of the Varicella (Chickenpox) vaccine, typically given as a first dose, with a second dose recommended later in childhood.
Toddler to Early School Years (18 Months to 6 Years): As children become more mobile and interactive, their vaccine needs evolve. The DTaP, IPV, and MMR vaccines receive their final doses in this stage, solidifying long-term immunity. The second dose of Varicella is also administered, usually between ages 4-6. This period is crucial for catching up on any missed doses and ensuring a complete vaccination record before entering school, where close contact with peers increases disease exposure risks.
Adolescence (7 Years to 18 Years): The vaccine schedule extends into the teenage years, addressing new health concerns. At 11-12 years, preteens receive the Tdap booster, which includes protection against tetanus, diphtheria, and pertussis, with a focus on the latter to prevent whooping cough. The HPV (Human Papillomavirus) vaccine series is initiated, typically as a two-dose regimen for those starting the series before their 15th birthday, offering protection against cancers caused by HPV. The Meningococcal conjugate vaccine (MenACWY) is also administered, with a booster dose recommended at age 16. Additionally, annual flu vaccines remain a staple, and catch-up doses for any missed vaccines are crucial during these years.
In summary, the childhood vaccine schedule is a comprehensive, age-specific plan that builds immunity against a wide array of diseases. Each phase is tailored to the child's developmental stage, ensuring optimal protection with minimal risk. Adhering to this schedule not only safeguards individual health but also contributes to herd immunity, protecting vulnerable members of the community. Parents and caregivers play a vital role in this process, from keeping track of vaccine appointments to monitoring their child's response to each dose. With proper education and adherence, the vaccine schedule becomes a powerful tool in the fight against preventable diseases.
US Vaccination Progress: Tracking Total Inoculations to Date
You may want to see also
Explore related products






![]()
Mandatory vs. Optional: Vaccines required by law versus those recommended but not compulsory
Childhood vaccination schedules are a tapestry of mandatory and optional vaccines, each thread woven with the intent to protect against preventable diseases. In the United States, for instance, the Centers for Disease Control and Prevention (CDC) recommends 14 different vaccines by age 18, targeting diseases like measles, mumps, rubella, polio, and hepatitis B. However, the legal requirement for these vaccines varies by state and often hinges on school entry. This distinction between mandatory and optional vaccines raises critical questions about public health, individual choice, and community immunity.
Mandatory vaccines are those required by law for school or daycare attendance, typically enforced to prevent outbreaks of highly contagious diseases. For example, the MMR (measles, mumps, rubella) vaccine is compulsory in nearly all U.S. states, with exemptions granted only for medical, religious, or philosophical reasons in some jurisdictions. These vaccines are often administered in multiple doses, such as the DTaP series (diphtheria, tetanus, pertussis), which is given at 2, 4, 6, and 15–18 months, followed by boosters at 4–6 years and 11–12 years. The rationale behind mandating these vaccines is clear: diseases like measles can spread rapidly in unvaccinated populations, posing a threat not only to individuals but also to those who cannot be vaccinated due to medical conditions.
Optional vaccines, on the other hand, are recommended by health authorities but not legally required. Examples include the HPV (human papillomavirus) vaccine, which is advised for preteens and teens (typically starting at age 11 or 12), and the meningococcal vaccine, recommended for adolescents and young adults. These vaccines often target diseases that, while serious, may not pose the same immediate public health risk as measles or polio. The decision to administer optional vaccines frequently rests with parents and healthcare providers, who must weigh the benefits of protection against factors like cost, accessibility, and perceived risk.
The divide between mandatory and optional vaccines highlights a tension between collective responsibility and individual autonomy. Mandatory vaccines prioritize herd immunity, ensuring that a high enough percentage of the population is immune to interrupt disease transmission. Optional vaccines, however, often address more nuanced risks, such as HPV’s link to certain cancers or meningococcal disease’s rarity but severity. For instance, the HPV vaccine is administered in a two-dose series for those starting the series before age 15, or a three-dose series for those starting later, yet its uptake varies widely due to its optional status and misconceptions about its necessity.
In practice, navigating this landscape requires informed decision-making. Parents should consult healthcare providers to understand the risks and benefits of both mandatory and optional vaccines, considering factors like their child’s health, community disease prevalence, and travel plans. For example, the hepatitis A vaccine, often optional, might be prioritized for children living in or traveling to regions with high disease rates. Similarly, the influenza vaccine, recommended annually for all children over six months, remains optional but is strongly advised to prevent seasonal outbreaks. By distinguishing between legal requirements and health recommendations, families can make choices that align with both public health goals and individual needs.
Chickenpox Vaccine Contagious Period: What You Need to Know
You may want to see also
Explore related products




![]()
Common Childhood Vaccines: List of vaccines like MMR, DTaP, and polio
Childhood vaccinations are a cornerstone of public health, protecting young lives from preventable diseases. Among the most critical are the MMR, DTaP, and polio vaccines, each targeting specific threats with proven efficacy. These vaccines not only safeguard individual children but also contribute to herd immunity, reducing disease outbreaks in communities. Understanding their purpose, schedule, and administration is essential for parents and caregivers.
The MMR vaccine, a combination shot against measles, mumps, and rubella, is typically administered in two doses. The first dose is given around 12 to 15 months of age, with the second dose following between 4 and 6 years. Measles, a highly contagious virus, can lead to severe complications like pneumonia and encephalitis, making vaccination crucial. Mumps and rubella, though less common, can cause serious issues such as deafness and birth defects if contracted during pregnancy. Parents should ensure timely vaccination, especially before children enter school, where close contact increases disease risk.
DTaP, another combination vaccine, protects against diphtheria, tetanus, and pertussis (whooping cough). The series begins at 2 months of age, with subsequent doses at 4 months, 6 months, and a booster between 15 and 18 months. A final dose is given before kindergarten entry, around 4 to 6 years. Pertussis is particularly dangerous for infants, causing violent coughing fits that can lead to breathing difficulties or even death. Tetanus, often called "lockjaw," enters the body through wounds and can cause muscle stiffness and spasms. Diphtheria affects the respiratory system, forming a thick coating in the throat that can block airways. Adhering to the DTaP schedule is vital to build immunity during early childhood.
Polio vaccination has nearly eradicated this once-feared disease globally. Inactivated poliovirus vaccine (IPV) is the standard in the U.S., given in four doses: at 2 months, 4 months, 6-18 months, and 4-6 years. Polio can cause paralysis and, in severe cases, death. While rare today, the virus still exists in some parts of the world, making vaccination essential for travelers and global health security. Parents should keep vaccination records updated, especially for international travel, where proof of immunization may be required.
Practical tips for vaccine administration include scheduling appointments during calm times of day and bringing a favorite toy or book to distract the child. After vaccination, monitor for mild side effects like soreness, fever, or fussiness, which can be managed with acetaminophen or a cool compress. Always consult a healthcare provider if severe reactions occur. By staying informed and following recommended schedules, parents can ensure their children receive the full benefits of these life-saving vaccines.
Neil deGrasse Tyson's Insights on Vaccines: Science and Safety
You may want to see also
Explore related products






![]()
Vaccine Combinations: How multiple vaccines are often combined into single shots for efficiency
Childhood vaccination schedules can seem overwhelming, with a long list of diseases to protect against. However, a clever strategy employed by healthcare providers is the combination of multiple vaccines into a single shot, streamlining the process and reducing the number of injections required. This approach not only simplifies the vaccination process but also improves compliance, as parents and children alike appreciate the reduced number of visits and needle pricks.
Consider the DTaP-IPV-Hib vaccine, a quintessential example of a combination vaccine. This single injection protects against five diseases: diphtheria, tetanus, pertussis (whooping cough), polio, and Haemophilus influenzae type b (Hib). Administered in a series of doses at 2, 4, 6, and 15-18 months of age, this combination vaccine reduces the number of injections from five to one per visit. The dosage remains consistent across age categories, with each 0.5 mL dose containing 20-30 units of diphtheria toxoid, 20 units of tetanus toxoid, 5-10 micrograms of pertussis toxoid, 3-5 micrograms of filamentous hemagglutinin, 5 micrograms of pertactin, 40 D-antigen units of inactivated polio vaccine, and 10 micrograms of Hib polysaccharide conjugated to tetanus toxoid.
From an analytical perspective, the benefits of combination vaccines extend beyond convenience. By reducing the number of injections, healthcare providers can minimize the risk of administration errors, such as incorrect dosage or missed vaccinations. Moreover, combination vaccines can improve vaccine uptake, particularly in areas with limited access to healthcare services. A study published in the Journal of Pediatrics found that combination vaccines increased vaccination coverage rates by 10-15% in underserved communities. To maximize the benefits of combination vaccines, parents should ensure their child receives the recommended series of doses on schedule, allowing for optimal immune response and protection.
A comparative analysis of combination vaccines reveals their superiority over individual vaccines in terms of efficiency and cost-effectiveness. For instance, the MMRV vaccine, which combines measles, mumps, rubella, and varicella (chickenpox) vaccines, reduces the number of injections from four to one. This not only saves time and resources but also decreases the likelihood of vaccine hesitancy due to the reduced number of visits. However, it's essential to note that combination vaccines may have specific precautions and contraindications. Parents should inform their healthcare provider of any allergies, immune system disorders, or previous adverse reactions to vaccines, as these may affect the suitability of combination vaccines for their child.
In practice, parents can facilitate the vaccination process by keeping a record of their child's vaccination history, including the type, date, and dosage of each vaccine received. This information can be shared with healthcare providers to ensure accurate and timely administration of combination vaccines. Additionally, parents should be aware of the potential side effects of combination vaccines, such as mild fever, irritability, or soreness at the injection site, which are generally mild and resolve within a few days. By understanding the nuances of combination vaccines and working closely with healthcare providers, parents can help ensure their child receives the full benefits of these efficient and effective vaccination strategies.
Medicare Part B: Meningococcal Vaccine Coverage Explained
You may want to see also
Explore related products






![]()
Global Variations: Differences in vaccination counts and schedules across countries
The number of childhood vaccinations administered globally varies significantly, influenced by factors such as disease prevalence, healthcare infrastructure, and public health priorities. For instance, while the United States recommends up to 16 vaccine doses by age 2, covering diseases like measles, mumps, and hepatitis B, countries like India focus on fewer but high-impact vaccines, such as the pentavalent vaccine (DTwP-HepB-Hib), which protects against five diseases in a single shot. This disparity highlights how regional health challenges shape immunization schedules.
Consider the timing and dosage differences across nations. In the UK, the measles, mumps, and rubella (MMR) vaccine is given in two doses, starting at 12 months, whereas in Japan, the first dose is often delayed until 12–18 months, with a second dose at 5–7 years. Such variations reflect differing risk assessments and cultural preferences. For parents traveling internationally, understanding these schedules is crucial; consult a healthcare provider to ensure your child’s immunizations align with both home and destination country requirements.
Analyzing these global variations reveals a balance between standardization and adaptation. The World Health Organization (WHO) provides a framework for essential vaccines, but countries tailor schedules to local needs. For example, yellow fever vaccination is mandatory in many African and South American countries due to endemic risk, while it’s optional elsewhere. This localized approach ensures resources are allocated efficiently, but it can complicate cross-border health management. Travelers should verify vaccination certificates and carry documentation, especially for region-specific vaccines.
A persuasive argument for harmonizing schedules emerges when examining vaccine hesitancy. Inconsistent messaging across countries can fuel misinformation. For instance, Japan’s historically cautious approach to HPV vaccination led to lower uptake, while Australia’s comprehensive school-based program achieved high coverage. Standardizing schedules where scientifically appropriate could strengthen global trust in vaccines. Until then, parents must navigate these differences, prioritizing evidence-based decisions over conflicting advice.
Practically, families relocating internationally should plan ahead. Obtain a detailed vaccination record from your current provider and research the target country’s schedule. Some vaccines, like the inactivated polio vaccine (IPV), may require additional doses to meet new requirements. Use tools like the CDC’s Travelers’ Health website or WHO’s Vaccine Preventable Diseases portal for country-specific guidance. Proactive planning ensures continuity of care and protects children from preventable diseases, regardless of location.
Understanding Adverse Reactions: Vaccine Safety and Reported Side Effects
You may want to see also
Frequently asked questions
The exact number varies by country and specific health guidelines, but in the United States, the Centers for Disease Control and Prevention (CDC) recommends around 14 different vaccines by age 6, protecting against 16 vaccine-preventable diseases.
Most childhood vaccinations are required for school entry, but the specific requirements vary by state or country. Some vaccines may be optional or have exemptions based on medical, religious, or philosophical reasons.
Many childhood vaccinations are already combined into fewer shots to reduce the number of injections. For example, the MMR vaccine protects against measles, mumps, and rubella in one shot. However, reducing the number of vaccines further could leave children vulnerable to preventable diseases.