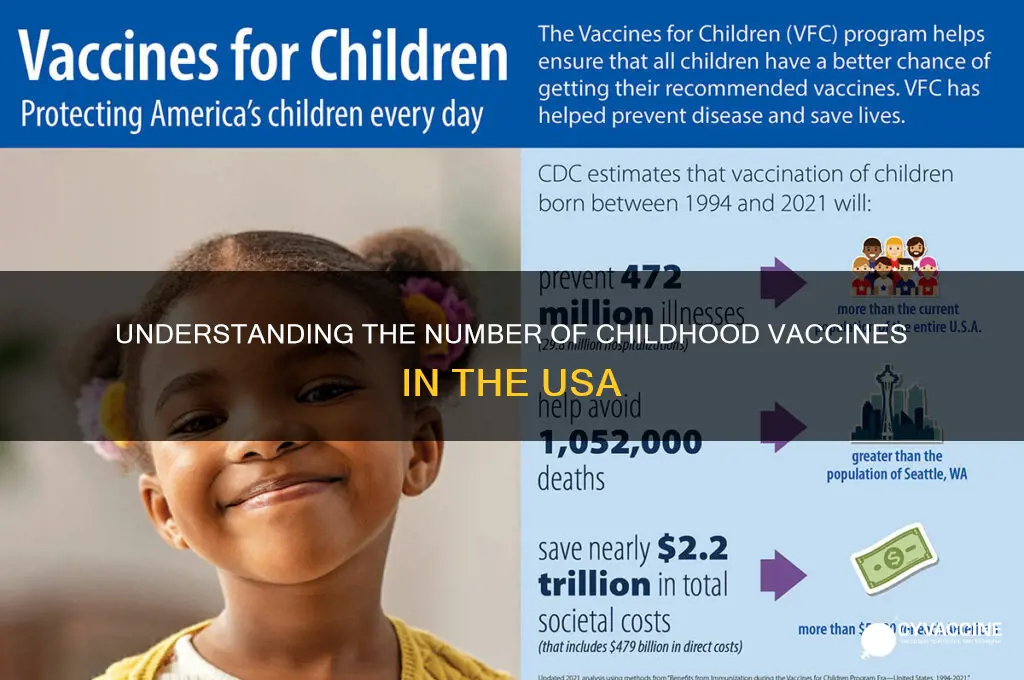
Childhood vaccination in the United States is a critical public health measure designed to protect children from preventable diseases and ensure community immunity. The Centers for Disease Control and Prevention (CDC) recommends a comprehensive schedule of vaccines for children from birth through adolescence, covering diseases such as measles, mumps, rubella, polio, whooping cough, and more. As of recent guidelines, the total number of doses administered during childhood can exceed 20, depending on the specific vaccines and their required series. This schedule is carefully crafted to provide immunity at the most vulnerable stages of life, balancing safety and efficacy to safeguard both individual health and public well-being. Understanding the number and timing of these vaccines is essential for parents, caregivers, and healthcare providers to ensure children receive the full benefits of immunization.
| Characteristics | Values |
|---|---|
| Total Recommended Childhood Vaccines (Birth to Age 18) | 16 (including combinations and series) |
| Vaccine Series (Multiple Doses) | DTaP (Diphtheria, Tetanus, Pertussis): 5 doses |
| Polio (IPV): 4 doses | |
| MMR (Measles, Mumps, Rubella): 2 doses | |
| Hepatitis B: 3 doses | |
| HPV (Human Papillomavirus): 2 or 3 doses (depending on age) | |
| Single-Dose Vaccines | Varicella (Chickenpox): 2 doses |
| Hepatitis A: 2 doses | |
| Meningococcal (MenACWY): 1–2 doses | |
| Meningococcal B (MenB): 2–3 doses (optional/recommended for high-risk) | |
| Influenza (Annual): 1–2 doses (starting at 6 months) | |
| COVID-19: 1–3 doses (depending on age and formulation) | |
| Age Range for Completion | Most vaccines completed by age 6; others (e.g., HPV, MenACWY) by 16 |
| Mandatory for School Entry | Varies by state but typically includes DTaP, MMR, Polio, Varicella |
| Optional/Recommended Vaccines | Meningococcal B, Hepatitis A (in some states) |
| Total Doses (Approximate) | 26–30 doses (depending on vaccine schedules and risk factors) |
| Source | CDC (Centers for Disease Control and Prevention), 2023 Immunization Schedule |
Explore related products


$11.93 $21.99




What You'll Learn
- Vaccine Schedule Overview: CDC-recommended timeline for childhood immunizations from birth to age 18
- Mandatory vs. Optional: State-specific requirements for school entry and exemptions
- Vaccine Types: List of common vaccines (e.g., MMR, DTaP, polio)
- Doses and Timing: Number of doses and age intervals for each vaccine
- Vaccine Safety: FDA approval process and monitoring for childhood vaccines
![]()
Vaccine Schedule Overview: CDC-recommended timeline for childhood immunizations from birth to age 18
The CDC's recommended vaccine schedule for children from birth to age 18 is a meticulously designed roadmap to protect against 14 preventable diseases. This timeline is not arbitrary; it's based on decades of research into immune system development, disease prevalence, and vaccine efficacy. For instance, the Hepatitis B vaccine is administered at birth, followed by a series of doses at 1-2 months and 6-18 months, to ensure protection during early childhood when the risk of infection is highest.
Birth to 6 Years: Building the Foundation
The first six years of life are critical for establishing immunity. The CDC recommends a series of vaccinations starting at birth, including Hepatitis B, Rotavirus (2-3 doses), and Diphtheria, Tetanus, and Pertussis (DTaP, 5 doses). For example, the DTaP vaccine is given at 2, 4, and 6 months, followed by booster doses at 15-18 months and 4-6 years. This staggered approach allows the immune system to build a robust response. Parents should be aware that some vaccines, like the Measles, Mumps, and Rubella (MMR) vaccine, are typically administered between 12-15 months, with a second dose at 4-6 years.
Ages 7 to 12: Maintaining Immunity
As children grow, the focus shifts to maintaining and boosting immunity. The CDC recommends the annual Influenza vaccine for all children aged 6 months and older. Additionally, the Human Papillomavirus (HPV) vaccine is recommended for both boys and girls aged 11-12, with a series of 2 doses (or 3 doses if started before age 15). This age range also includes catch-up vaccinations for any missed doses, such as the Varicella (Chickenpox) vaccine, which is typically given between 12-15 months and 4-6 years.
Ages 13 to 18: Preparing for Adulthood
The adolescent years are marked by a shift towards protecting against diseases that become more prevalent in adulthood. The CDC recommends the Meningococcal conjugate vaccine (MenACWY) at age 11-12, followed by a booster dose at age 16. The Serogroup B meningococcal (MenB) vaccine is also recommended for adolescents aged 16-18. Furthermore, teens should receive a single dose of the Tetanus, Diphtheria, and Pertussis (Tdap) vaccine if they haven't already, as well as a final dose of the HPV vaccine if they haven't completed the series. A practical tip for parents is to schedule these vaccinations during routine check-ups or sports physicals to minimize missed opportunities.
Practical Considerations and Tips
To ensure adherence to the CDC's vaccine schedule, parents should maintain a record of their child's vaccinations and share this information with all healthcare providers. Schools and daycare facilities often require proof of vaccination, so keeping these records handy is essential. If a child misses a scheduled dose, parents should consult their healthcare provider to determine the appropriate catch-up schedule. For example, if a child misses the 4-6 year booster dose of the DTaP vaccine, they can receive the dose as soon as possible, followed by the next dose 4-8 weeks later. By following the CDC's recommended timeline and staying informed about their child's vaccination status, parents can help protect their children from preventable diseases and contribute to community immunity.
Understanding Hyperimmune Responses: How Vaccines Trigger Enhanced Immunity
You may want to see also
Explore related products






![]()
Mandatory vs. Optional: State-specific requirements for school entry and exemptions
In the United States, the number of childhood vaccines required for school entry varies significantly by state, creating a patchwork of mandatory and optional immunization policies. While the Centers for Disease Control and Prevention (CDC) recommends a standardized schedule, states retain the authority to determine which vaccines are compulsory. For instance, all 50 states mandate the DTaP (Diphtheria, Tetanus, Pertussis) vaccine series, typically administered in five doses between 2 months and 6 years of age. However, requirements for vaccines like HPV (Human Papillomavirus) or Meningococcal vary widely, with some states making them mandatory for school entry and others leaving them optional or tied to specific grade levels.
Consider the contrasting approaches of California and Mississippi. California, known for its stringent vaccine laws, requires students to be fully immunized against 10 diseases, including measles, mumps, and rubella (MMR), unless a medical exemption is provided. In contrast, Mississippi allows exemptions only for medical reasons, resulting in one of the highest vaccination rates in the country. Meanwhile, states like Idaho permit exemptions for both medical and personal beliefs, leading to lower vaccination coverage and increased vulnerability to outbreaks. These disparities highlight the tension between public health goals and individual autonomy, with mandatory policies generally correlating to higher immunization rates and fewer disease outbreaks.
For parents navigating these requirements, understanding state-specific exemptions is crucial. Medical exemptions, typically issued for conditions like severe allergies or immunodeficiencies, are universally accepted but require documentation from a healthcare provider. Religious exemptions are allowed in 44 states, though the criteria for approval vary. Personal belief exemptions, once common, have been restricted or eliminated in many states due to concerns about vaccine hesitancy and outbreaks. For example, New York repealed non-medical exemptions in 2019 following a measles outbreak, underscoring the evolving nature of these policies. Parents should consult their state’s health department or school district for the most current requirements and exemption processes.
A practical tip for families moving between states is to review vaccination records well in advance of school enrollment. Some states may require additional doses or specific vaccines not mandated in others. For example, a child moving from a state without a Meningococcal vaccine requirement to one that does may need to receive the vaccine by age 11 or 16, depending on the state’s policy. Pharmacies and healthcare providers often offer catch-up schedules to ensure compliance without delaying school entry. Additionally, keeping a digital copy of immunization records can streamline the transition process and prevent delays.
Ultimately, the debate over mandatory versus optional vaccines reflects broader societal values regarding public health and personal freedom. While mandatory policies protect community immunity, they can face resistance from those who prioritize individual choice. Optional policies, on the other hand, risk lowering vaccination rates and increasing the spread of preventable diseases. As states continue to refine their requirements, staying informed and proactive is essential for parents and caregivers. By understanding the nuances of state-specific policies and exemptions, families can ensure their children meet school entry requirements while contributing to the broader goal of disease prevention.
Tractor Supply's Bordetella Vaccine Availability: What Pet Owners Need to Know
You may want to see also
Explore related products






![]()
Vaccine Types: List of common vaccines (e.g., MMR, DTaP, polio)
The United States recommends a comprehensive vaccination schedule for children, encompassing a range of vaccine types designed to protect against serious, preventable diseases. Among the most common are the MMR (Measles, Mumps, Rubella), DTaP (Diphtheria, Tetanus, Pertussis), and polio vaccines. Each serves a distinct purpose, targeting specific pathogens to build immunity during critical developmental stages. Understanding these vaccines—their components, administration schedules, and importance—is essential for parents and caregivers navigating childhood health.
MMR Vaccine: A Triple Shield Against Contagious Diseases
The MMR vaccine is a cornerstone of childhood immunization, administered in two doses: the first at 12–15 months and the second at 4–6 years. This combination vaccine prevents measles, a highly contagious virus causing fever and rash; mumps, known for painful swelling of the salivary glands; and rubella, which poses severe risks to pregnant women and their fetuses. Despite occasional misconceptions, extensive research confirms its safety and efficacy. Parents should ensure timely vaccination, especially before school entry, to protect children and contribute to herd immunity.
DTaP Vaccine: Protecting Against Respiratory and Neurological Threats
The DTaP vaccine safeguards against diphtheria, tetanus, and pertussis (whooping cough), with a series of five doses starting at 2 months and ending between 4–6 years. Diphtheria and pertussis target the respiratory system, while tetanus causes muscle stiffness and spasms via wound exposure. Booster doses (Tdap) are recommended at 11–12 years and during each pregnancy to maintain immunity. Parents should monitor for mild side effects like soreness or fever and consult a healthcare provider if concerns arise.
Polio Vaccine: Eradicating a Crippling Disease
Polio vaccination, administered as IPV (inactivated poliovirus), is given in four doses: at 2 months, 4 months, 6–18 months, and 4–6 years. This vaccine has nearly eradicated polio globally, a disease causing paralysis and, in severe cases, death. While rare in the U.S., global travel risks persist, making vaccination critical. Parents should adhere to the schedule, ensuring children receive all doses for full protection.
Practical Tips for Vaccine Administration
To ease the vaccination process, schedule appointments during calm times of day and bring a favorite toy or book for distraction. After vaccination, use cool compresses for injection site discomfort and administer acetaminophen if fever develops. Keep a record of vaccine dates and share it with all caregivers. Stay informed about school requirements and travel-related vaccine needs. By prioritizing these vaccines, parents play a vital role in safeguarding their child’s health and public well-being.
Exploring Vaccine Brands: Understanding the Diversity in Immunization Options
You may want to see also
Explore related products






![]()
Doses and Timing: Number of doses and age intervals for each vaccine
The CDC's recommended childhood immunization schedule outlines a precise roadmap for protecting children from 14 vaccine-preventable diseases. This schedule is not arbitrary; it's a carefully crafted plan based on when a child's immune system is most receptive to each vaccine and when they're most vulnerable to specific diseases.
For instance, the Hepatitis B vaccine is typically administered in three doses: the first at birth, the second at 1-2 months, and the third at 6-18 months. This staggered approach ensures the development of long-lasting immunity. Similarly, the Rotavirus vaccine, which protects against severe diarrhea, is given in a series of two or three doses, starting at 2 months and completing by 8 months. This timing coincides with the period when infants are most susceptible to this highly contagious virus.
Consider the Measles, Mumps, and Rubella (MMR) vaccine, a cornerstone of childhood immunization. It's administered in two doses: the first at 12-15 months and the second at 4-6 years. This two-dose regimen is crucial because a single dose provides only partial protection. The interval between doses allows the immune system to mature and mount a stronger response to the second dose, ensuring robust immunity against these highly contagious diseases. This principle of multiple doses spaced over time is a recurring theme in the immunization schedule, highlighting the importance of following the recommended timeline for optimal protection.
The DTaP vaccine, which shields against Diphtheria, Tetanus, and Pertussis, exemplifies the need for booster doses. The initial series consists of five doses, starting at 2 months and completing by 4-6 years. However, a booster dose (Tdap) is recommended at 11-12 years to reinforce immunity, particularly against Pertussis, which can be severe in adolescents and adults. This multi-dose approach underscores the dynamic nature of immunity and the need for periodic reinforcement.
While the immunization schedule provides a clear framework, flexibility is built into the system. Minor deviations from the recommended intervals generally don't necessitate restarting the series. However, significant delays may require adjustments to ensure timely completion. Healthcare providers play a pivotal role in guiding parents through the schedule, addressing concerns, and ensuring that children receive their vaccines on time. Adherence to the recommended doses and intervals is paramount for individual protection and community immunity, a concept where high vaccination rates prevent disease outbreaks and protect vulnerable individuals who cannot be vaccinated.
RSV Vaccine: Does It Stop Transmission or Just Prevent Illness?
You may want to see also
Explore related products






![]()
Vaccine Safety: FDA approval process and monitoring for childhood vaccines
The United States recommends 16 vaccine doses against 6 diseases for children by age 2, yet the FDA’s approval process ensures each vaccine meets rigorous safety and efficacy standards before it reaches pediatric offices. This multi-stage evaluation begins with preclinical testing, where vaccines are studied in labs and animals to assess their immune response and potential risks. Clinical trials follow, progressing through three phases involving thousands of volunteers to confirm safety, determine dosage, and prove effectiveness. For instance, the Pfizer-BioNTech COVID-19 vaccine for children aged 5–11 underwent trials with over 3,000 participants, demonstrating a lower dose (10 micrograms vs. 30 micrograms for adults) was both safe and effective. Only after this data is reviewed by the FDA’s Vaccines and Related Biological Products Advisory Committee does a vaccine receive approval or emergency use authorization.
Approval is just the beginning. Post-market surveillance systems like the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) continuously monitor vaccines for rare or long-term side effects. VAERS relies on healthcare providers and parents to report adverse events, while VSD analyzes healthcare data from over 12 million people to detect patterns. For example, these systems identified a rare link between the rotavirus vaccine RotaShield and intussusception in 1999, leading to its withdrawal. Today’s rotavirus vaccines, RotaTeq and Rotarix, have been administered to millions of children with no significant safety concerns. This ongoing monitoring ensures that even the rarest risks are identified and addressed promptly.
Parents often wonder how vaccines are tailored for children, and the answer lies in age-specific formulations and dosing. The hepatitis B vaccine, for instance, is administered in three doses starting at birth, with pediatric doses containing 5 micrograms of antigen compared to 10 micrograms for adults. Similarly, the MMR (measles, mumps, rubella) vaccine is given in two doses, the first at 12–15 months and the second at 4–6 years, to align with a child’s developing immune system. These adjustments are based on extensive research to maximize protection while minimizing side effects, such as mild fever or soreness at the injection site.
Critically, the FDA’s process is not static; it adapts to emerging science and public health needs. During the COVID-19 pandemic, the FDA expedited vaccine approvals without compromising safety standards, allowing the Moderna and Pfizer vaccines to be authorized for adolescents and later children as young as 6 months. This flexibility, combined with robust monitoring, ensures vaccines remain a cornerstone of pediatric health. For parents, understanding this process can build confidence in the vaccines their children receive, knowing each dose has been meticulously tested, approved, and monitored for safety.
Vaccination Divide: Shared Concerns, Goals, and Misconceptions Explored
You may want to see also
Frequently asked questions
The Centers for Disease Control and Prevention (CDC) recommends approximately 14 different vaccines for children from birth to age 18, protecting against 16 vaccine-preventable diseases.
Most states require certain vaccines for school entry, but the specific requirements vary by state. Common vaccines include MMR (measles, mumps, rubella), DTaP (diphtheria, tetanus, pertussis), and polio.
Yes, all states allow medical exemptions, and most allow religious exemptions. Some states also permit philosophical exemptions, but the availability of these exemptions varies.
The CDC’s recommended childhood vaccine schedule is reviewed and updated annually by the Advisory Committee on Immunization Practices (ACIP) based on the latest scientific evidence.