The topic of myocarditis cases potentially linked to COVID-19 vaccines has sparked significant public and scientific interest, particularly following reports of rare instances of heart inflammation in individuals, primarily young males, after receiving mRNA-based vaccines. While myocarditis is a recognized adverse event, its incidence remains extremely low compared to the vast number of vaccine doses administered globally. Health authorities, such as the CDC and WHO, emphasize that the benefits of vaccination in preventing severe COVID-19 outcomes far outweigh the minimal risks associated with myocarditis. Ongoing research and surveillance continue to monitor and assess these cases to ensure vaccine safety and inform public health strategies.
| Characteristics | Values |
|---|---|
| Vaccine Type | Primarily mRNA vaccines (Pfizer-BioNTech, Moderna) |
| Age Group Most Affected | Adolescents and young adults (12-29 years old), particularly males |
| Onset Time After Vaccination | Typically within 1-7 days after the second dose |
| Symptoms | Chest pain, shortness of breath, fatigue, palpitations |
| Severity | Mostly mild to moderate, rarely severe |
| Reported Cases (U.S.) | Approximately 1,000-2,000 cases (as of late 2023, CDC data) |
| Incidence Rate (U.S.) | ~10-47 cases per million doses (second dose, males 12-29) |
| Recovery Rate | High; most cases resolve with minimal intervention |
| Long-term Effects | Limited data, but most patients recover fully |
| Risk vs. Benefit | Myocarditis risk from COVID-19 infection is significantly higher than from vaccination |
| Monitoring | Active surveillance by health agencies (e.g., CDC, FDA) |
| Recommendations | Vaccination still strongly recommended due to overall benefits outweighing rare risks |
Explore related products






What You'll Learn
![]()
Myocarditis cases post-COVID-19 vaccination: global statistics
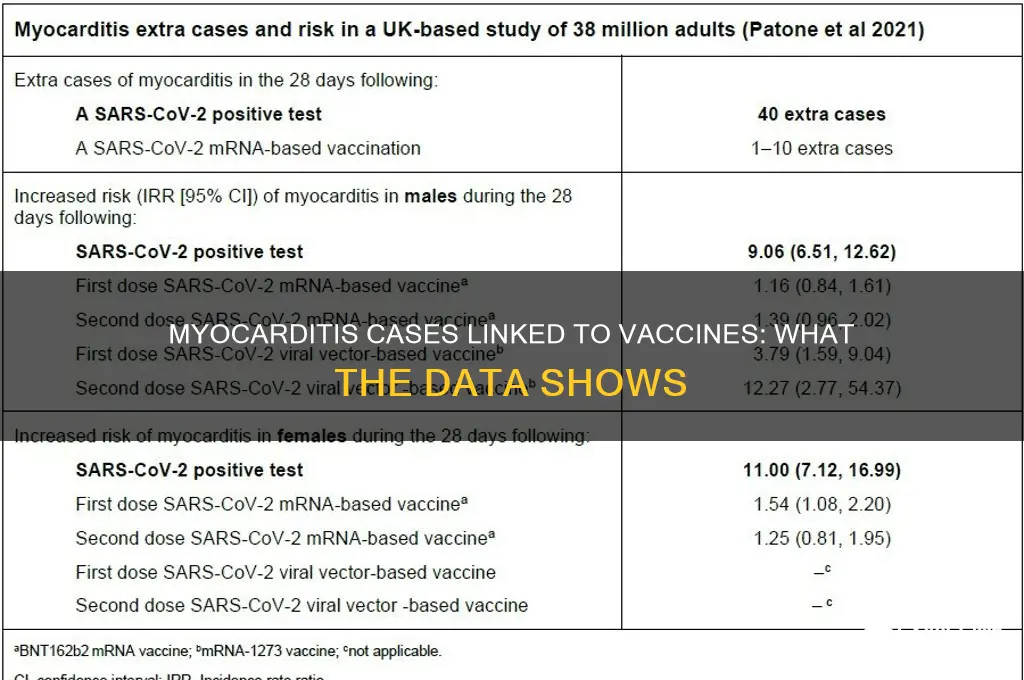
Myocarditis, an inflammation of the heart muscle, has been a rare but notable concern following COVID-19 vaccination, particularly with mRNA vaccines like Pfizer-BioNTech and Moderna. Global data indicates that the incidence is highest among adolescent males and young men after the second dose, with rates ranging from 1 to 10 cases per 100,000 vaccinated individuals in this demographic. For context, the risk is significantly lower in females and older age groups, with fewer than 1 case per 100,000 reported. These statistics highlight the importance of monitoring specific populations while emphasizing the overall rarity of this adverse event.
Analyzing the data reveals a clear pattern: the risk of myocarditis post-vaccination is dose-dependent, with the second dose posing a higher risk than the first. Studies from Israel, the United States, and Europe consistently show that cases typically occur within a week of vaccination, often presenting as chest pain, shortness of breath, or palpitations. Most cases are mild and resolve with minimal intervention, such as rest and anti-inflammatory medications. However, healthcare providers are advised to maintain vigilance, particularly when vaccinating males aged 12–29, who account for the majority of reported cases.
From a comparative perspective, the risk of myocarditis from COVID-19 infection itself is substantially higher than from vaccination. Research suggests that COVID-19 patients are 16 times more likely to develop myocarditis than those vaccinated. This underscores the vaccine’s role in preventing more severe outcomes, including heart complications. For example, a study in *The Lancet* found that the incidence of myocarditis in unvaccinated COVID-19 patients was 11 cases per 100,000, compared to 1 case per 100,000 vaccinated individuals. This disparity reinforces the net benefit of vaccination despite rare side effects.
Practical guidance for healthcare professionals and the public includes monitoring for symptoms post-vaccination, particularly after the second dose in younger males. If symptoms occur, prompt evaluation with tools like ECG, troponin levels, and cardiac MRI can confirm diagnosis. Transparency in communication about risks is crucial to maintaining public trust while ensuring informed decision-making. Parents and young adults should weigh the low risk of myocarditis against the proven efficacy of vaccines in preventing severe COVID-19, hospitalization, and long-term complications like multisystem inflammatory syndrome (MIS-C) in children.
In conclusion, while myocarditis cases post-COVID-19 vaccination are rare and typically mild, their concentration in specific demographics warrants targeted awareness and monitoring. The data reinforces the vaccine’s safety profile while highlighting the need for tailored public health messaging. By balancing risk communication with evidence-based benefits, healthcare systems can continue to promote vaccination as a critical tool in the global fight against COVID-19.
Strategic Market Analysis for Influenza Vaccine Development and Launch
You may want to see also
Explore related products





![]()
Vaccine types linked to myocarditis: mRNA vs. others
Myocarditis, an inflammation of the heart muscle, has been a rare but notable concern associated with certain vaccines, particularly mRNA vaccines like Pfizer-BioNTech and Moderna. Data from the Centers for Disease Control and Prevention (CDC) and other health agencies indicate that the risk is highest among adolescent males and young men, typically after the second dose. For instance, rates of myocarditis following mRNA vaccination are estimated at 10.7 to 40.9 cases per million doses in this demographic, compared to 1 to 2 cases per million for non-mRNA vaccines like Novavax or Janssen (Johnson & Johnson).
To minimize risk, health authorities recommend spacing mRNA vaccine doses by at least 8 weeks for individuals under 30, as longer intervals appear to reduce myocarditis incidence. Symptoms to monitor post-vaccination include chest pain, shortness of breath, or abnormal heart rhythms, which typically manifest within a week of vaccination. If these occur, immediate medical evaluation is advised, though most cases resolve with rest and anti-inflammatory treatment.
Comparatively, non-mRNA vaccines have a lower myocarditis risk profile. For example, the adenovirus-based Janssen vaccine has been linked to rare cases of thrombosis with thrombocytopenia syndrome (TTS) but fewer myocarditis reports. Novavax, a protein subunit vaccine, has shown even lower rates in clinical trials, though real-world data is still emerging. This suggests that vaccine platform differences—mRNA vs. non-mRNA—play a role in myocarditis risk, with mRNA vaccines exhibiting a slightly higher but still rare occurrence.
Practically, individuals concerned about myocarditis should weigh the benefits of vaccination against COVID-19, which include reduced risk of severe illness, hospitalization, and long-term cardiac complications from the virus itself. For those at higher risk of myocarditis, consulting a healthcare provider to discuss alternative vaccine options or dose timing can be a prudent step. Ultimately, the risk of myocarditis from vaccination remains exceedingly low compared to the cardiac risks posed by COVID-19 infection.
HPV Vaccine for Girls at 13: Protecting Against Cervical Cancer
You may want to see also
Explore related products






![]()
Age groups most affected by vaccine-related myocarditis
Vaccine-related myocarditis, though rare, has shown a distinct pattern in terms of age group susceptibility. Data from multiple health agencies, including the CDC and EMA, consistently highlight that adolescents and young adults, particularly males aged 12 to 29, are at the highest risk. This demographic experiences myocarditis most frequently after receiving mRNA COVID-19 vaccines, specifically following the second dose. The incidence rate peaks in the 12–15 and 16–24 age brackets, with males in these groups reporting cases at a rate of approximately 10 to 69 per million doses, compared to significantly lower rates in older adults and females.
Analyzing the data reveals a clear dose-dependent trend. The risk of myocarditis increases after the second dose of mRNA vaccines, with symptoms typically appearing within 1–4 days post-vaccination. This temporal association underscores the importance of monitoring young recipients during this critical window. While the condition is usually mild and resolves with conservative management, the concentration of cases in this age group has prompted health authorities to issue tailored guidance. For instance, some countries now recommend extending the interval between doses for adolescents to potentially mitigate risk, though this remains a subject of ongoing research.
From a comparative standpoint, the risk-benefit analysis remains firmly in favor of vaccination across all age groups. Myocarditis associated with COVID-19 infection is significantly more common and severe than vaccine-related cases, particularly in younger populations. However, the age-specific risk of vaccine-induced myocarditis necessitates targeted communication strategies. Parents and young adults should be informed about potential symptoms—such as chest pain, shortness of breath, or palpitations—and advised to seek medical attention promptly if these occur. This proactive approach ensures early intervention and minimizes complications.
Practical tips for healthcare providers and caregivers include emphasizing the importance of hydration and rest after vaccination, especially for adolescents. Encouraging recipients to avoid strenuous physical activity for a few days post-vaccination may also reduce the likelihood of triggering symptoms. While these measures are not definitive preventive strategies, they align with current recommendations to optimize safety. Ultimately, understanding the age-specific risk profile of vaccine-related myocarditis empowers both providers and recipients to make informed decisions, balancing protection against COVID-19 with vigilance for rare adverse events.
Exploring mRNA Vaccines: A Historical Perspective on Their Development
You may want to see also
Explore related products






![]()
Recovery rates from myocarditis after vaccination
Myocarditis following COVID-19 vaccination, though rare, has been a focal point of discussion, particularly among younger males. Data from the Centers for Disease Control and Prevention (CDC) and the European Medicines Agency (EMA) indicate that the incidence is highest in adolescent males and young men after the second dose of mRNA vaccines, with rates ranging from 10.7 to 40.9 cases per million doses. Despite the alarming headlines, the recovery rates from vaccine-induced myocarditis are reassuringly high, with most cases resolving within a short period.
Understanding the Recovery Timeline
The majority of myocarditis cases post-vaccination are mild and self-limiting. Studies show that symptoms, such as chest pain and fatigue, typically appear within 7 days of vaccination, peaking around day 3. Hospitalization is often brief, with most patients discharged within 2–3 days. A 2022 study published in *JAMA Cardiology* found that 95% of affected individuals fully recovered within 6 months, with no long-term cardiac complications. For adolescents aged 12–17, who are at higher risk, recovery is even faster, with 85% returning to normal activities within 3 weeks.
Factors Influencing Recovery
Several factors contribute to the swift recovery from vaccine-related myocarditis. Early diagnosis and prompt treatment, including anti-inflammatory medications like NSAIDs and rest, play a critical role. Age is another determinant; younger patients tend to recover more quickly than older adults. Additionally, the absence of pre-existing cardiac conditions significantly improves outcomes. A study in *Circulation* highlighted that patients who received supportive care and avoided strenuous activity for 3–6 months post-recovery had no recurrence of symptoms.
Practical Tips for Affected Individuals
If diagnosed with myocarditis after vaccination, follow these steps:
- Rest Immediately: Avoid physical exertion for at least 3–6 months, as recommended by the American Heart Association.
- Monitor Symptoms: Keep track of chest pain, shortness of breath, or palpitations, and report any worsening to a healthcare provider.
- Follow-Up Care: Schedule cardiac evaluations, including ECGs and troponin tests, to ensure full recovery.
- Vaccination Guidance: Consult a cardiologist before receiving subsequent doses or other vaccines.
Comparing Recovery to Other Causes of Myocarditis
Vaccine-induced myocarditis has a more favorable prognosis compared to cases caused by viral infections, such as SARS-CoV-2 itself. COVID-19-related myocarditis often presents with more severe symptoms and a longer recovery period, with up to 20% of patients experiencing persistent cardiac dysfunction. In contrast, vaccine-related cases rarely lead to long-term damage, underscoring the importance of vaccination in preventing more serious cardiac complications from the virus.
In summary, while vaccine-related myocarditis is a rare but notable side effect, the recovery rates are exceptionally high, particularly among younger populations. With proper management and adherence to medical advice, most individuals can expect a full and swift return to health.
Wisconsin Vaccine Eligibility: Who Qualifies for COVID-19 Shots Now?
You may want to see also
Explore related products






![]()
Myocarditis risk comparison: vaccines vs. COVID-19 infection
Myocarditis, an inflammation of the heart muscle, has been a rare but concerning topic in discussions about COVID-19 vaccines and infections. Data from the Centers for Disease Control and Prevention (CDC) and other health agencies show that mRNA vaccines, particularly Pfizer-BioNTech and Moderna, have been associated with a small increased risk of myocarditis, primarily in adolescent males and young adults after the second dose. However, the incidence remains extremely low, with approximately 1 to 2 cases per 100,000 vaccinated individuals in this demographic. This risk is not uniform across age groups, with older adults showing significantly lower rates.
To put this in perspective, COVID-19 infection itself poses a far greater risk of myocarditis. Studies indicate that SARS-CoV-2 infection increases the likelihood of myocarditis by a factor of 15 to 16 times compared to vaccination. For instance, a study published in *Circulation* found that the incidence of myocarditis in COVID-19 patients was approximately 11 cases per 100,000 infections, dwarfing the vaccine-related risk. This disparity highlights the protective value of vaccination, even when considering rare side effects.
From a practical standpoint, healthcare providers should counsel patients, especially younger males, about the potential risk of myocarditis post-vaccination while emphasizing the vastly higher risk associated with COVID-19 infection. Symptoms to monitor include chest pain, shortness of breath, or abnormal heart rhythms within a week of vaccination. If these occur, immediate medical evaluation is essential. For those hesitant due to myocarditis concerns, the data clearly show that the benefits of vaccination in preventing severe COVID-19 outcomes far outweigh the risks.
A comparative analysis reveals that while vaccine-related myocarditis is rare and typically mild, COVID-19-induced myocarditis is more frequent and often severe, requiring hospitalization in many cases. For example, a 2022 study in *JAMA Cardiology* found that 40% of COVID-19 patients with myocarditis required intensive care, compared to less than 5% of vaccine-related cases. This underscores the importance of vaccination as a preventive measure, particularly in populations at higher risk of severe COVID-19 complications.
In conclusion, while myocarditis is a valid concern, the data unequivocally demonstrate that the risk from COVID-19 infection is substantially higher than that from vaccination. Healthcare professionals and individuals must weigh these risks carefully, prioritizing evidence-based decision-making to protect public health. Vaccination remains a critical tool in reducing the overall burden of myocarditis and other severe outcomes associated with COVID-19.
Pneumococcal Vaccine: Who Among Children Should Get It?
You may want to see also
Frequently asked questions
As of recent data, the incidence of myocarditis following COVID-19 vaccination is rare, with estimates ranging from 1 to 12 cases per 100,000 vaccinated individuals, primarily occurring in young males after the second dose of mRNA vaccines.
The mRNA vaccines, Pfizer-BioNTech and Moderna, have been most commonly linked to myocarditis cases, particularly in adolescents and young adults after the second dose.
Studies show that the risk of myocarditis from COVID-19 infection is significantly higher than the risk from vaccination, with infection posing a greater overall threat to health, including more severe myocarditis cases.