The distribution of vaccines to states is a complex, multi-faceted process that involves coordination between federal, state, and local health authorities, as well as pharmaceutical manufacturers and logistics providers. At the federal level, the Centers for Disease Control and Prevention (CDC) and the Department of Health and Human Services (HHS) play a critical role in allocating vaccine doses to states based on factors such as population size, disease prevalence, and healthcare infrastructure. Once allocated, states are responsible for developing and implementing their own distribution plans, which often prioritize high-risk groups such as healthcare workers, elderly individuals, and those with underlying health conditions. The logistics of vaccine distribution are further complicated by the need for specialized storage and handling, particularly for vaccines that require ultra-cold temperatures, such as the Pfizer-BioNTech COVID-19 vaccine. To ensure efficient and equitable distribution, states often partner with local health departments, hospitals, pharmacies, and community organizations to establish vaccination sites and reach underserved populations. Throughout the process, real-time data tracking and monitoring are essential to identify and address distribution bottlenecks, ensure accountability, and maintain public trust in the vaccination effort.
| Characteristics | Values |
|---|---|
| Allocation Basis | Population of adults (18+) in each state/jurisdiction. |
| Data Source for Population | U.S. Census Bureau’s 2019 American Community Survey (latest available). |
| Distribution Process | Federal government allocates vaccines to states based on population data. |
| State Role | States determine distribution plans within their jurisdictions. |
| Federal Partners | CDC, HHS, and Operation Warp Speed (previously) oversee distribution. |
| Vaccine Types Distributed | Pfizer-BioNTech, Moderna, Johnson & Johnson (as of latest data). |
| Equity Considerations | Priority for underserved and high-risk populations. |
| Monitoring System | CDC’s Vaccine Administration Management System (VAMS) tracks distribution. |
| Current Phase (as of 2023) | Open to all individuals aged 6 months and older. |
| Booster Distribution | Allocated based on demand and eligibility criteria. |
| Private Sector Involvement | Pharmacies (e.g., CVS, Walgreens) receive direct federal allocations. |
| Transparency | Weekly allocation data published by CDC and state health departments. |
| Adjustments | Allocations adjusted based on uptake, wastage, and local needs. |
| Global Distribution | U.S. donates surplus vaccines through COVAX and bilateral agreements. |
Explore related products




$48.91 $66


What You'll Learn
- Federal Allocation Formulas: Based on population, disease risk, and healthcare infrastructure needs
- State Distribution Plans: States prioritize counties, cities, and vulnerable populations
- Cold Chain Logistics: Maintaining vaccine temperature during transport and storage
- Provider Enrollment: Hospitals, clinics, and pharmacies register to receive doses
- Equity Monitoring: Ensuring fair access across demographics and geographic areas
![]()
Federal Allocation Formulas: Based on population, disease risk, and healthcare infrastructure needs
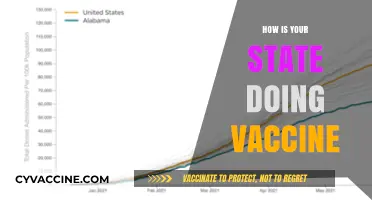
The distribution of vaccines to states is a complex process that hinges on federal allocation formulas designed to ensure equitable and effective coverage. These formulas are not arbitrary; they are meticulously crafted to account for three critical factors: population size, disease risk, and healthcare infrastructure needs. By balancing these elements, the federal government aims to maximize the impact of limited vaccine supplies while addressing regional disparities.
Consider the population-based component first. States with larger populations naturally require more vaccine doses to achieve herd immunity. For instance, California, with its nearly 40 million residents, would receive a significantly larger allocation than Wyoming, which has fewer than 600,000. However, raw population numbers aren’t the sole determinant. Age distribution plays a role too. States with higher percentages of elderly residents, such as Florida, may receive additional doses to prioritize vulnerable age groups, often starting with those over 65 or 75, depending on the vaccine’s efficacy data.
Disease risk is another pivotal factor. States experiencing outbreaks or with higher baseline rates of the targeted disease are prioritized. During the COVID-19 pandemic, for example, states with surging cases or lower vaccination rates were often allocated extra doses. Similarly, regions with historically high influenza rates might receive larger flu vaccine allocations. This risk-based approach ensures that resources are directed where they’re most needed, often using real-time data to adjust distributions dynamically.
Healthcare infrastructure needs are equally critical, particularly in rural or underserved areas. States with fewer hospitals, clinics, or healthcare providers may struggle to administer vaccines efficiently. To address this, federal formulas allocate additional doses or logistical support, such as mobile vaccination units or funding for storage facilities capable of handling ultra-cold vaccines like Pfizer’s mRNA shot, which requires temperatures of -94°F. This ensures that even remote communities can access vaccines without wastage or delays.
Practical implementation of these formulas requires collaboration between federal agencies, state health departments, and local providers. States must submit detailed plans outlining how they’ll distribute doses, prioritize populations, and report administration data. For example, a state might allocate 40% of its doses to urban centers, 30% to rural areas, and 30% to high-risk populations like healthcare workers or immunocompromised individuals. Transparency and accountability are key, with weekly updates and adjustments based on uptake rates and emerging needs.
In conclusion, federal allocation formulas are a strategic tool for vaccine distribution, balancing population size, disease risk, and infrastructure needs to ensure fairness and efficiency. By understanding these formulas, states can better prepare for vaccine rollouts, advocate for their specific needs, and ultimately protect their residents more effectively. This structured approach, while complex, is essential for navigating the challenges of large-scale immunization campaigns.
The Kid Who Defied Parents: A Vaccination Story
You may want to see also
Explore related products






![]()
State Distribution Plans: States prioritize counties, cities, and vulnerable populations
In the intricate process of vaccine distribution, states play a pivotal role in ensuring equitable access, particularly by prioritizing counties, cities, and vulnerable populations. Each state develops its own distribution plan, often guided by federal recommendations but tailored to local needs. For instance, states like California and New York have implemented phased approaches, starting with healthcare workers and long-term care residents, then expanding to essential workers, seniors, and individuals with underlying health conditions. These plans are not one-size-fits-all; they account for regional disparities in population density, healthcare infrastructure, and disease prevalence. For example, rural counties in states like Montana or Wyoming may receive allocations based on their ability to store and administer vaccines, such as the Moderna vaccine, which requires storage at -20°C, compared to the Pfizer vaccine’s -70°C requirement.
Analyzing these plans reveals a common thread: vulnerability-based prioritization. States often use data on COVID-19 cases, hospitalizations, and mortality rates to identify high-risk areas. For instance, counties with higher poverty rates, limited access to healthcare, or large elderly populations are frequently prioritized. In Florida, counties like Miami-Dade and Broward, with dense urban populations and significant elderly communities, received early allocations. Similarly, in Texas, Harris County, home to Houston, was prioritized due to its large population and healthcare worker density. This data-driven approach ensures that vaccines reach those most at risk, even within the same state. However, it also highlights the need for flexibility, as states must adapt to changing infection rates and vaccine supply.
A critical aspect of state distribution plans is the collaboration with local governments and community organizations. Cities and counties often serve as the last mile in vaccine delivery, requiring coordination with health departments, hospitals, pharmacies, and mobile clinics. For example, Chicago partnered with community-based organizations to set up vaccination sites in underserved neighborhoods, ensuring accessibility for vulnerable populations. In contrast, smaller cities like Austin, Texas, utilized local pharmacies and drive-thru clinics to efficiently distribute doses. Practical tips for local implementation include pre-registration systems to manage demand, multilingual outreach to address language barriers, and transportation assistance for those without access to vaccination sites. These strategies not only streamline distribution but also build trust in communities with historically low vaccination rates.
Comparing state plans also underscores the importance of balancing speed with equity. Some states, like West Virginia, were praised for their rapid rollout by leveraging existing infrastructure from their opioid crisis response. Others, like Mississippi, faced challenges due to lower healthcare capacity and hesitancy. A key takeaway is that successful distribution requires a dual focus: reaching high-risk populations while maintaining a steady pace to cover the broader population. For instance, allocating 70% of doses to priority groups in the initial phases, as recommended by the CDC, ensures protection for the most vulnerable without delaying progress. States must also prepare for unique challenges, such as handling multi-dose vials (e.g., Pfizer’s 6-dose vials) or managing second-dose appointments, which demand precise planning and communication.
Ultimately, state distribution plans are a testament to the complexity of public health logistics. By prioritizing counties, cities, and vulnerable populations, states can address disparities and save lives. However, this requires continuous monitoring, adaptability, and community engagement. For example, as new variants emerge or vaccine supply fluctuates, states must be ready to reallocate resources or adjust eligibility criteria. Practical steps include regularly updating distribution maps, providing real-time data on vaccine availability, and offering clear guidelines for age categories (e.g., 65+ or 16+ with comorbidities). In this way, state plans not only distribute vaccines but also lay the groundwork for a more resilient healthcare system.
Nurse Faints Post-Vaccine: Unraveling the Incident and Aftermath
You may want to see also
Explore related products


$14.97 $29.95




![]()
Cold Chain Logistics: Maintaining vaccine temperature during transport and storage
Vaccines are highly sensitive biological products that require precise temperature control to remain effective. The cold chain—a temperature-controlled supply chain—is critical to ensuring vaccines reach their destination in optimal condition. From the moment a vaccine is manufactured until it is administered, it must be stored and transported within a specific temperature range, typically between 2°C and 8°C (36°F and 46°F). Even brief exposure to temperatures outside this range can compromise efficacy, rendering doses unusable and wasting valuable resources.
Consider the Pfizer-BioNTech COVID-19 vaccine, which requires ultra-cold storage at -70°C ±10°C (-94°F ±15°F) before distribution. This presents unique logistical challenges, as specialized freezers and dry ice are needed to maintain such low temperatures. For instance, when distributing this vaccine to rural or remote areas, logistics teams must plan routes meticulously to minimize transit time and ensure continuous temperature monitoring. In contrast, vaccines like the Moderna COVID-19 vaccine can be stored at standard freezer temperatures (-20°C/-4°F) for up to six months, offering more flexibility in distribution. Understanding these differences is crucial for designing effective cold chain systems tailored to each vaccine’s requirements.
Maintaining the cold chain involves more than just refrigeration. It requires a coordinated effort across multiple stakeholders, including manufacturers, distributors, healthcare providers, and government agencies. Key components include insulated packaging, temperature monitoring devices, and backup power systems to prevent temperature excursions during power outages. For example, data loggers and real-time monitoring systems can track temperature fluctuations, providing alerts if conditions deviate from the required range. Additionally, "last-mile" delivery—the final stage of transport to remote or hard-to-reach areas—often relies on portable cold storage units and trained personnel to ensure vaccines remain viable.
Despite advancements, cold chain logistics face significant challenges. In low-resource settings, inadequate infrastructure, unreliable electricity, and limited access to specialized equipment can disrupt the supply chain. For instance, during the COVID-19 pandemic, many African countries struggled to distribute vaccines due to insufficient cold chain capacity. To address this, innovative solutions like solar-powered refrigerators and drone deliveries have been piloted in some regions. These technologies not only improve access but also reduce the environmental impact of traditional cold chain methods.
In conclusion, cold chain logistics are the backbone of vaccine distribution, ensuring that life-saving doses retain their potency from production to administration. By understanding the unique temperature requirements of different vaccines and implementing robust monitoring and storage systems, stakeholders can minimize waste and maximize impact. As global vaccination efforts continue to evolve, investing in resilient cold chain infrastructure will be essential to overcoming distribution challenges and achieving equitable vaccine access worldwide.
Caleb White's Vaccine Status: Unraveling the Truth Behind the Speculations
You may want to see also
Explore related products






![]()
Provider Enrollment: Hospitals, clinics, and pharmacies register to receive doses
Provider enrollment is the critical first step in ensuring that vaccines reach those who need them most. Hospitals, clinics, and pharmacies must register with state or federal health departments to qualify for vaccine distribution. This process involves submitting detailed information about their facility, including storage capabilities, staff qualifications, and patient demographics. For instance, providers must confirm they have ultra-cold freezers if they plan to administer mRNA vaccines like Pfizer-Comirnaty, which require storage at -94°F to -68°F. Without proper enrollment, even the largest hospitals cannot receive doses, making this step a linchpin in the distribution chain.
The enrollment process is not one-size-fits-all. Each state has its own criteria and application system, often managed through platforms like the Centers for Disease Control and Prevention’s (CDC) Vaccine Ordering Management System (VOMS). Providers must also agree to adhere to strict guidelines, such as prioritizing high-risk populations—elderly individuals, healthcare workers, and those with comorbidities—during initial phases. For example, a rural clinic might receive smaller, more frequent shipments to avoid wastage, while a large urban hospital could handle bulk deliveries. Understanding these nuances is essential for providers to navigate the system effectively.
One common challenge in provider enrollment is the administrative burden. Facilities must designate a vaccine coordinator, track inventory meticulously, and report administration data within 72 hours of each dose. Pharmacies, in particular, often face additional hurdles, such as ensuring pharmacists are trained to administer vaccines to specific age groups—like adolescents aged 12–15, who require a different dosage than adults. Despite these challenges, enrollment offers providers access to resources like the Vaccine Adverse Event Reporting System (VAERS) and educational materials to support their efforts.
A persuasive argument for streamlined enrollment lies in its impact on equity. Providers in underserved areas, such as community health centers or independent pharmacies, often struggle with the complexity of registration. Simplifying this process—through standardized forms, multilingual support, or technical assistance—could ensure these critical access points are not left behind. For instance, during the COVID-19 vaccine rollout, states like California prioritized enrolling providers in ZIP codes with high social vulnerability indices, reducing disparities in access.
In conclusion, provider enrollment is more than a bureaucratic hurdle; it’s a strategic tool for efficient and equitable vaccine distribution. By understanding the requirements, leveraging available resources, and advocating for simplification, hospitals, clinics, and pharmacies can play their part in safeguarding public health. Whether managing a 0.3 mL pediatric dose or a 0.5 mL adult dose, every enrolled provider contributes to a network that protects communities, one registration at a time.
Identifying Vaccination Status in Deceased Individuals: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Equity Monitoring: Ensuring fair access across demographics and geographic areas
Vaccine distribution is not just about delivering doses; it’s about ensuring those doses reach the right people in the right places at the right time. Equity monitoring plays a critical role in this process by identifying and addressing disparities in access across demographics and geographic areas. Without robust monitoring, vulnerable populations—such as rural communities, racial minorities, or the elderly—risk being left behind, undermining the overall effectiveness of vaccination campaigns.
Consider the logistical challenges of distributing a vaccine like Pfizer-BioNTech, which requires ultra-cold storage at -70°C. Urban areas with advanced infrastructure may receive and administer doses efficiently, while rural regions lack the necessary equipment or trained personnel. Equity monitoring involves tracking these disparities and allocating resources—such as mobile vaccination units or additional funding—to bridge the gap. For instance, during the COVID-19 vaccine rollout, some states prioritized zip codes with higher social vulnerability indices, ensuring doses reached underserved communities first.
Demographic data is another cornerstone of equity monitoring. Age, race, ethnicity, and socioeconomic status significantly influence vaccine access and hesitancy. For example, a 2021 CDC report revealed that Black and Hispanic individuals were less likely to receive vaccines due to barriers like transportation and mistrust of healthcare systems. To address this, equity monitoring frameworks must include targeted outreach—such as multilingual campaigns, community partnerships, and accessible vaccination sites in low-income neighborhoods. A practical tip: use local leaders and trusted figures to disseminate information, as they can effectively combat misinformation and encourage uptake.
Geographic equity extends beyond urban-rural divides to include hard-to-reach areas like islands, border towns, and tribal lands. In Alaska, for instance, the state partnered with tribal health organizations to distribute vaccines to remote Native communities, ensuring doses were administered according to cultural preferences and logistical needs. This approach highlights the importance of tailoring distribution strategies to local contexts, rather than applying a one-size-fits-all model. Equity monitoring in such cases involves not just tracking doses delivered but also measuring vaccination rates and identifying barriers to access.
Finally, equity monitoring requires transparency and accountability. States must publish disaggregated data on vaccine distribution and uptake, broken down by demographics and geographic areas. This data allows policymakers, advocates, and the public to identify inequities in real time and demand corrective action. For example, if a county’s vaccination rate for 65+ residents lags behind the state average, officials can deploy pop-up clinics or increase dose allocations to that area. By embedding equity monitoring into the distribution process, states can ensure that vaccines serve as a tool for health justice, not just disease prevention.
RSV Vaccine for Seniors: Is It a Necessary Protection?
You may want to see also
Frequently asked questions
The federal government initially allocated COVID-19 vaccines to states based on population size, with each state receiving a proportional share of available doses. Over time, allocations evolved to consider factors like vaccination rates, demand, and equity to ensure fair distribution.
State governments are responsible for developing and implementing distribution plans, prioritizing populations (e.g., healthcare workers, elderly), and coordinating with local health departments, hospitals, pharmacies, and other providers to ensure vaccines reach eligible individuals efficiently.
Vaccines are transported using specialized cold chain logistics to maintain required temperatures. Ultra-cold vaccines (like Pfizer’s) require dry ice or freezers, while others (like Moderna’s) can be stored in standard refrigerators. States and providers must adhere to strict storage and handling guidelines to ensure vaccine effectiveness.