The rollout of COVID-19 vaccines has been a critical aspect of public health efforts across the United States, with each state implementing its own strategies to distribute and administer doses. As of now, the progress varies significantly from one state to another, influenced by factors such as population density, healthcare infrastructure, and local policies. Some states have achieved high vaccination rates, successfully reaching a large portion of their eligible populations, while others face challenges such as vaccine hesitancy, supply chain issues, or disparities in access. Understanding how your state is performing in terms of vaccine distribution and uptake is essential for assessing local public health outcomes and identifying areas for improvement. By examining key metrics like vaccination rates, demographic disparities, and the pace of administration, individuals can gain insight into the effectiveness of their state’s efforts and advocate for equitable and efficient vaccine distribution.
Explore related products






What You'll Learn
- Vaccine Distribution Efficiency: Tracking how quickly and fairly vaccines are being distributed across the state
- Vaccination Rates by Age: Analyzing vaccination completion percentages among different age groups in the state
- Vaccine Hesitancy Trends: Identifying regions or demographics with higher resistance to COVID-19 vaccination
- Booster Shot Uptake: Measuring the percentage of eligible residents receiving COVID-19 booster doses
- Vaccine Equity Initiatives: Evaluating state programs to ensure equitable vaccine access for underserved communities
![]()
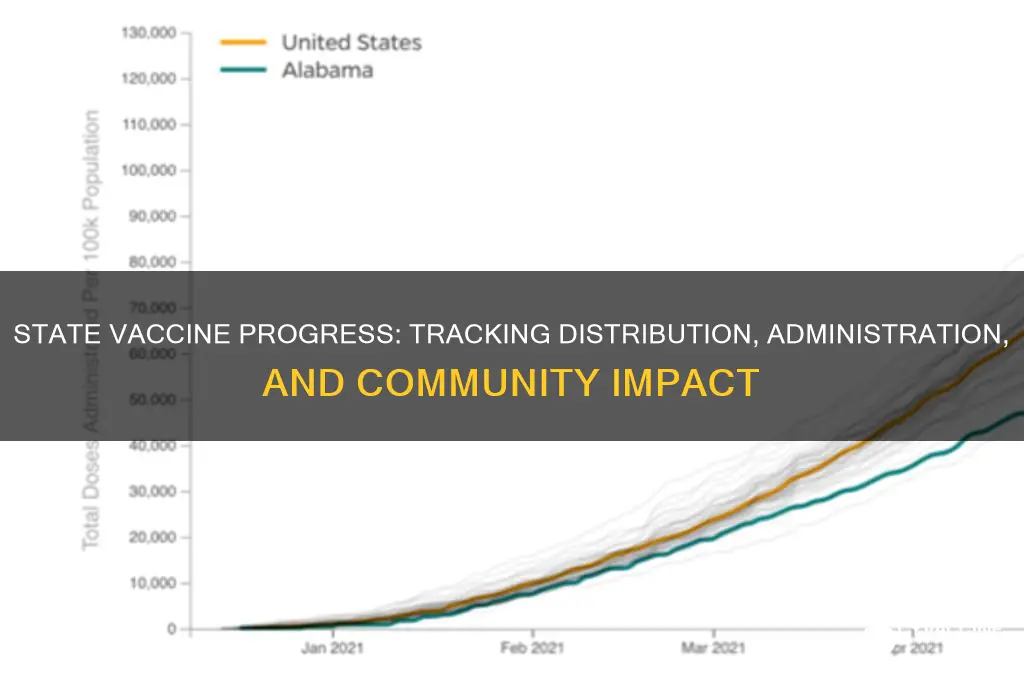
Vaccine Distribution Efficiency: Tracking how quickly and fairly vaccines are being distributed across the state
The speed at which vaccines are administered directly impacts public health outcomes. A state that vaccinates 70% of its eligible population within six months of vaccine availability can significantly reduce hospitalization rates and deaths compared to one that takes twice as long. Tracking distribution efficiency involves monitoring daily and weekly vaccination rates, identifying bottlenecks in supply chains, and ensuring that doses are not expiring unused. For instance, some states have implemented real-time dashboards that show how many doses have been administered out of the total received, broken down by county or demographic group. This transparency helps pinpoint areas lagging behind and allows for swift corrective action.
Fairness in vaccine distribution is as critical as speed, ensuring that marginalized communities are not left behind. Data should be disaggregated by age, race, ethnicity, and socioeconomic status to reveal disparities. For example, if a state reports that 60% of its population over 65 is vaccinated, but only 30% of that group in rural areas has received a dose, it signals a systemic issue. Solutions might include mobile vaccination clinics, partnerships with local community organizations, and multilingual outreach campaigns. Prioritizing equity not only saves lives but also builds trust in public health systems, which is essential for long-term disease prevention.
Practical steps for improving distribution efficiency include optimizing appointment systems and reducing waste. States can adopt digital platforms that allow residents to schedule vaccinations easily, with reminders for second doses. Walk-in clinics and extended hours can accommodate those who cannot take time off work. Additionally, providers should be trained in drawing extra doses from vials when possible—for example, some COVID-19 vaccine vials contain enough for six doses instead of five with proper technique. These small adjustments can collectively increase the number of people vaccinated without requiring additional supply.
Comparing distribution strategies across states offers valuable lessons. For instance, one state might excel in urban areas but struggle in rural regions, while another has successfully bridged this gap through innovative transportation solutions. Analyzing these differences highlights best practices that can be adapted elsewhere. A comparative approach also fosters healthy competition among states, driving improvements in efficiency and equity. By studying both successes and failures, policymakers can refine their strategies to maximize impact.
Ultimately, tracking vaccine distribution efficiency requires a combination of data-driven analysis, community engagement, and adaptability. It’s not enough to know how many doses have been administered; understanding *where* and *to whom* they’ve been given is crucial. States must remain vigilant in addressing disparities and flexible in responding to challenges like supply fluctuations or hesitancy. With careful planning and execution, efficient and equitable vaccine distribution becomes not just a goal but a reality.
Post-Vaccine Arm Pain: Understanding Causes and Relief Tips
You may want to see also
Explore related products






![]()
Vaccination Rates by Age: Analyzing vaccination completion percentages among different age groups in the state
The latest data reveals a striking disparity in vaccination completion rates across age groups within the state, with seniors aged 65 and older leading at 89% fully vaccinated, while young adults aged 18-24 trail behind at 58%. This gap underscores not only varying levels of access and awareness but also differing perceptions of risk among demographics. For instance, older adults, who face higher risks from COVID-19, have prioritized vaccination, whereas younger groups may perceive themselves as less vulnerable, despite being key vectors for community transmission.
To bridge this gap, public health initiatives must tailor strategies to specific age groups. For young adults, leveraging social media campaigns and partnering with universities or workplaces could increase visibility and convenience. Pop-up clinics at campuses or offering incentives like discounts at local businesses post-vaccination might boost participation. Meanwhile, for middle-aged adults (35-54), who hover around 72% completion, addressing vaccine hesitancy through trusted community leaders or debunking misinformation could be effective.
A closer look at the data also highlights the success of school-based vaccination drives for adolescents aged 12-17, who have reached 75% completion. This suggests that integrating vaccination into existing routines—such as back-to-school health checks or sports physicals—works well for this age group. Parents play a critical role here, so providing clear, accessible information about vaccine safety and long-term benefits could further improve rates.
Finally, analyzing these age-based trends offers a roadmap for targeted interventions. For example, while seniors have high completion rates, ensuring they receive booster doses remains crucial. Conversely, focusing on young adults and middle-aged groups could significantly reduce overall transmission rates. By understanding these nuances, the state can allocate resources more effectively, ensuring no age group is left behind in achieving herd immunity.
Launching a Successful Vaccination Program: Essential Steps and Strategies
You may want to see also
Explore related products






![]()
Vaccine Hesitancy Trends: Identifying regions or demographics with higher resistance to COVID-19 vaccination
COVID-19 vaccination rates vary widely across regions and demographics, with certain areas and groups exhibiting higher resistance to immunization. Rural communities, for instance, often report lower vaccination rates compared to urban centers. This disparity can be attributed to limited access to healthcare facilities, lower health literacy, and a stronger reliance on local, sometimes misinformation-driven, networks. In states like Mississippi and Alabama, rural counties have consistently lagged behind in vaccination efforts, with rates up to 20% lower than their urban counterparts. Addressing this gap requires targeted strategies, such as mobile vaccination clinics and community-led education campaigns, to build trust and improve accessibility.
Demographically, younger adults aged 18–29 and individuals without college degrees show higher vaccine hesitancy. Surveys indicate that skepticism among these groups often stems from concerns about long-term side effects and a perceived lower risk of severe illness. For example, in states like Wyoming and Idaho, where college attainment rates are below the national average, vaccination rates among younger adults are significantly lower. Public health initiatives should focus on tailored messaging that addresses specific concerns, such as emphasizing the vaccine’s safety profile and its role in preventing long COVID, which disproportionately affects younger populations.
Racial and ethnic minorities, particularly Black and Hispanic communities, initially faced higher hesitancy due to historical medical mistrust and systemic barriers. However, recent data from states like Georgia and Texas show that targeted outreach efforts, including partnerships with community leaders and culturally sensitive messaging, have helped close this gap. For instance, vaccination rates among Hispanic adults in Texas increased by 15% after bilingual campaigns and pop-up clinics were introduced in predominantly Latino neighborhoods. These successes highlight the importance of culturally competent strategies in overcoming hesitancy.
Political affiliation also plays a significant role in vaccine resistance. Counties with strong conservative leanings, such as those in rural Pennsylvania and Ohio, often report lower vaccination rates. Misinformation spread through partisan media and social networks has fueled skepticism in these areas. To counter this, public health officials should collaborate with local trusted figures, such as religious leaders or sports personalities, to disseminate accurate information. Additionally, framing vaccination as a community protection measure rather than a political issue can help bridge ideological divides.
Finally, socioeconomic factors, such as income and employment status, contribute to hesitancy. Low-income individuals, particularly those in gig or service industries, may face logistical barriers like unpaid time off for vaccination or side effects. States like California and New York have implemented policies offering paid leave for vaccine appointments and recovery, which has shown promise in increasing uptake among these groups. Practical solutions, such as evening and weekend vaccination hours, can further reduce barriers for working populations. By addressing these specific challenges, states can make significant strides in reducing vaccine hesitancy across diverse populations.
Vaccines in the 1970s: A Look at Their Existence and Impact
You may want to see also
Explore related products






![]()
Booster Shot Uptake: Measuring the percentage of eligible residents receiving COVID-19 booster doses
As of the latest data, the percentage of eligible residents receiving COVID-19 booster doses varies significantly across states, with some regions boasting uptake rates above 50% among adults, while others lag behind at less than 30%. This disparity highlights the need for targeted strategies to improve booster shot uptake, particularly in areas with lower vaccination rates. For instance, states like Vermont and Connecticut have consistently led in booster administration, with over 60% of their eligible populations receiving an additional dose, compared to states like Mississippi and Alabama, where the rate hovers around 25%. Understanding these variations is crucial for identifying successful outreach methods and replicating them in underperforming regions.
To measure booster shot uptake effectively, public health officials should focus on age-specific data, as eligibility and hesitancy often differ across demographic groups. Adults aged 65 and older typically show higher booster uptake, with rates exceeding 70% in some states, due to their increased vulnerability to severe COVID-19 outcomes. Conversely, younger adults aged 18–49 have lower uptake, often below 40%, despite being eligible for boosters. Breaking down data by age allows for tailored messaging—emphasizing long-term protection for younger adults or partnering with senior centers to reach older populations. Additionally, tracking booster rates among immunocompromised individuals, who may require a third primary dose and a booster, is essential for ensuring comprehensive protection.
Increasing booster shot uptake requires a multi-faceted approach that addresses access, awareness, and hesitancy. Practical steps include expanding mobile vaccination clinics to underserved areas, offering flexible scheduling at workplaces and schools, and providing clear, culturally sensitive information about booster benefits. For example, pop-up clinics at grocery stores or community events have proven effective in reaching hesitant populations. Pairing these efforts with incentives, such as gift cards or discounts, can further motivate individuals to get boosted. Public health campaigns should also debunk myths about booster necessity, emphasizing that waning immunity increases the risk of breakthrough infections and severe illness.
Comparing state-level strategies reveals that successful booster campaigns often involve collaboration between local governments, healthcare providers, and community organizations. States with high uptake rates frequently leverage trusted messengers, such as local doctors or religious leaders, to encourage vaccination. For instance, Minnesota’s partnership with tribal nations and rural health clinics has helped bridge gaps in booster access. In contrast, states relying solely on statewide mandates or broad messaging have seen slower progress. By studying these examples, regions with lower uptake can adapt proven tactics to their unique contexts, ensuring a more equitable distribution of booster doses.
Ultimately, measuring and improving booster shot uptake is not just about tracking numbers—it’s about saving lives and preventing healthcare systems from being overwhelmed. A 10% increase in booster uptake could significantly reduce hospitalizations and deaths, particularly during surges driven by new variants. States must prioritize data transparency, sharing real-time metrics on booster rates by county or zip code to identify hotspots of low uptake. Combining this data with actionable strategies, such as targeted outreach and improved access, can create a roadmap for boosting protection across all eligible populations. The goal is clear: ensure that every eligible resident has the opportunity and motivation to receive their booster dose.
Is Pre-Exposure Rabies Vaccine Covered by Insurance? What You Need to Know
You may want to see also
Explore related products






![]()
Vaccine Equity Initiatives: Evaluating state programs to ensure equitable vaccine access for underserved communities
Underserved communities face systemic barriers to vaccine access, from transportation challenges to mistrust rooted in historical injustices. To address this, states like California and New York have launched targeted equity initiatives. California’s *Vaccinate All 58* campaign allocated 40% of its initial vaccine doses to the lowest-income ZIP codes, identified using the Healthy Places Index. New York’s *Vax for All* program deployed mobile clinics to public housing complexes and partnered with community organizations to provide on-site vaccinations for seniors and essential workers. These efforts highlight a critical strategy: geographic and demographic targeting must underpin equity initiatives to dismantle access barriers.
Evaluating these programs requires clear metrics and community-driven feedback. For instance, Illinois’ *Equity-Focused Vaccine Administration Plan* tracks vaccination rates by race, ethnicity, and income level, comparing them to the state’s demographic baseline. A key metric is the equity ratio: the proportion of doses administered to underserved populations relative to their share of the population. Programs should also measure trust-building outcomes, such as increased vaccination rates in communities with historically low uptake. Without robust data collection and transparent reporting, even well-intentioned initiatives risk perpetuating disparities.
Practical implementation demands flexibility and cultural competency. In Texas, the *Saving Our Seniors* initiative trained volunteers to assist with registration and provided transportation vouchers for elderly residents in rural areas. Similarly, Minnesota’s *MN Equity Vaccine Collaborative* employed multilingual staff and offered evening/weekend clinic hours to accommodate working families. These examples underscore the importance of meeting communities where they are—literally and figuratively. Initiatives must adapt to local needs, whether by offering walk-in appointments, providing childcare during vaccinations, or addressing language barriers with translated materials.
Sustainability is the ultimate test of vaccine equity initiatives. Short-term solutions, like pop-up clinics, are vital but insufficient without long-term infrastructure. States like Massachusetts have integrated equity into their public health framework by establishing permanent community health worker programs. These workers build trust, educate residents, and connect them to healthcare resources beyond vaccines. To ensure lasting impact, states must embed equity into policy, allocate dedicated funding, and foster partnerships with grassroots organizations. Without sustained commitment, equity initiatives risk becoming fleeting responses to a persistent problem.
Ensuring Vaccine Compliance: How to Verify Up-to-Date Immunizations
You may want to see also
Frequently asked questions
Vaccine distribution varies by state, but most states provide regular updates on their official health department websites or through public dashboards. Check your state’s health department website for the latest data on doses administered, eligibility, and distribution plans.
The percentage of fully vaccinated individuals differs by state and is updated frequently. Visit the CDC’s COVID Data Tracker or your state’s health department website for the most current vaccination rates.
States vary in vaccine rollout based on population, infrastructure, and policy. National comparisons can be found on platforms like the CDC’s COVID Data Tracker or independent research organizations like Kaiser Family Foundation.
Common challenges include supply shortages, hesitancy, and reaching underserved populations. Specific issues for your state can be found in local news reports or updates from your state’s health department.