The influenza vaccine's effectiveness in any given market is typically measured through a combination of epidemiological surveillance, vaccine uptake rates, and clinical studies. Health authorities monitor influenza activity, including the prevalence of specific strains, hospitalization rates, and mortality data, to assess how well the vaccine is protecting the population. Vaccine uptake rates, which indicate the percentage of the target population that has received the vaccine, are also crucial in evaluating its impact. Additionally, post-vaccination studies, such as test-negative design studies, compare the likelihood of vaccinated individuals contracting influenza versus those who are unvaccinated, providing direct evidence of vaccine efficacy. These metrics collectively help stakeholders understand the vaccine's performance, identify areas for improvement, and guide future vaccination strategies.
Explore related products


$11.93 $21.99




What You'll Learn
- Vaccine Efficacy Metrics: Measures how well the vaccine prevents influenza illness in real-world settings
- Market Demand Analysis: Assesses consumer demand and uptake rates for the influenza vaccine annually
- Cost-Effectiveness Evaluation: Analyzes the economic impact and value of the vaccine in healthcare systems
- Distribution Channel Performance: Tracks vaccine delivery efficiency through pharmacies, clinics, and other channels
- Adverse Event Monitoring: Evaluates safety by measuring reported side effects post-vaccination in the market
![]()
Vaccine Efficacy Metrics: Measures how well the vaccine prevents influenza illness in real-world settings
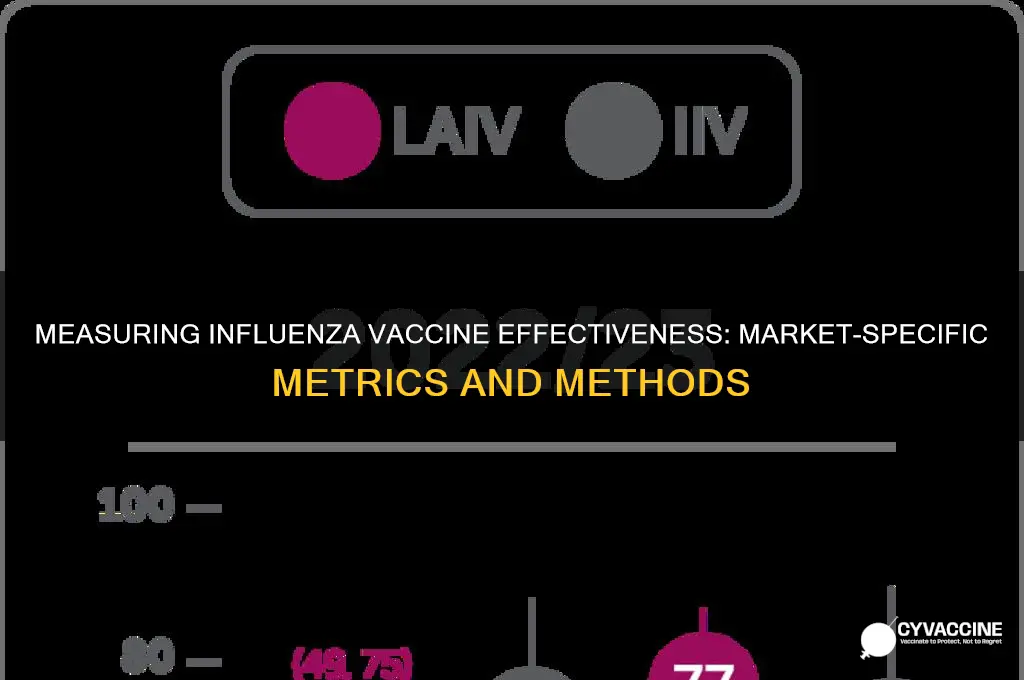
Vaccine efficacy metrics are critical for understanding how well influenza vaccines perform in real-world settings, beyond controlled clinical trials. These metrics assess the vaccine’s ability to prevent influenza illness, reduce severity, and limit transmission within populations. One of the primary measures is vaccine effectiveness (VE), which compares the risk of influenza infection or illness among vaccinated individuals to those who are unvaccinated. VE is typically calculated using observational studies, such as test-negative designs, where individuals seeking medical care for acute respiratory illness are tested for influenza, and the odds of vaccination are compared between those who test positive and those who test negative. This approach provides a direct estimate of how well the vaccine prevents medically attended influenza in real-world conditions.
Another important metric is relative efficacy, which measures the reduction in disease incidence among vaccinated individuals compared to a control group. This is often expressed as a percentage and is derived from randomized controlled trials or large-scale observational studies. For example, if a vaccine has a relative efficacy of 60%, it means vaccinated individuals are 60% less likely to develop influenza compared to those who are unvaccinated. However, relative efficacy must be interpreted alongside factors like virus strain mismatch, population immunity, and vaccine uptake rates, as these can significantly influence real-world performance.
Absolute risk reduction (ARR) is another valuable metric, representing the difference in the risk of influenza illness between vaccinated and unvaccinated groups. ARR provides a more tangible measure of the vaccine’s impact by quantifying the number of cases prevented per vaccinated individual. For instance, if the ARR is 5%, it means 5 fewer cases of influenza occur for every 100 vaccinated individuals. This metric is particularly useful for public health decision-making, as it directly reflects the vaccine’s real-world benefit.
In addition to preventing illness, vaccine efficacy metrics also assess the vaccine’s ability to reduce disease severity and hospitalization. Studies often evaluate outcomes such as the rate of influenza-related hospitalizations, intensive care admissions, or deaths among vaccinated versus unvaccinated populations. A vaccine that significantly lowers these severe outcomes, even if it does not entirely prevent infection, is still considered highly effective in protecting public health. These metrics are especially important for high-risk groups, such as the elderly, young children, and individuals with underlying health conditions.
Finally, population-level impact is a broader metric that evaluates how vaccination programs reduce the overall burden of influenza in a community. This includes measures like reductions in outpatient visits, hospitalizations, and mortality rates at the population level. Population-level impact is influenced not only by vaccine efficacy but also by vaccination coverage rates and the circulating influenza strains. Monitoring these metrics helps public health officials assess the success of vaccination campaigns and adjust strategies to maximize protection against influenza in real-world settings.
Vaccination's Role in Strengthening Immunity and Preventing Diseases
You may want to see also
Explore related products





![]()
Market Demand Analysis: Assesses consumer demand and uptake rates for the influenza vaccine annually
Market demand analysis for the influenza vaccine is a critical component in understanding consumer behavior and vaccine uptake rates. This analysis involves examining various factors that influence consumer decisions, such as awareness, accessibility, and perceived benefits of the vaccine. By evaluating these elements, stakeholders can gauge the annual demand and identify trends that impact vaccination rates. Primary data sources include vaccination records from healthcare providers, pharmacies, and public health departments, which provide insights into the number of doses administered each year. Secondary data, such as surveys and consumer behavior studies, further enriches the analysis by capturing public sentiment and barriers to vaccination.
Consumer demand for the influenza vaccine is often measured through uptake rates, which reflect the percentage of the target population that receives the vaccine annually. These rates are typically segmented by demographic groups, such as age, geographic location, and socioeconomic status, to identify disparities in access and acceptance. For instance, elderly populations and healthcare workers often exhibit higher uptake rates due to increased vulnerability and occupational requirements, respectively. Market demand analysis also considers the role of public health campaigns and media influence in driving vaccination rates. Effective campaigns can significantly boost demand by addressing misconceptions and highlighting the vaccine’s effectiveness in preventing severe illness.
Another key aspect of market demand analysis is the evaluation of seasonal variations and external factors that impact vaccine uptake. Influenza vaccine demand is inherently tied to the flu season, with peak demand occurring in the months leading up to and during the outbreak. However, factors such as vaccine availability, cost, and public trust in healthcare systems can either enhance or hinder uptake. For example, supply chain disruptions or vaccine hesitancy fueled by misinformation can lead to lower demand, even during high-risk seasons. Analyzing these dynamics helps in forecasting demand and ensuring adequate vaccine supply to meet consumer needs.
Market demand analysis also involves benchmarking against previous years’ data to identify growth or decline in vaccination rates. This longitudinal approach allows stakeholders to assess the effectiveness of interventions, such as expanded access programs or financial incentives, in increasing uptake. Additionally, comparing regional or national demand trends provides insights into best practices and areas for improvement. For instance, regions with higher uptake rates may have more robust distribution networks or stronger community engagement strategies that can be replicated elsewhere.
Finally, understanding market demand requires integrating qualitative and quantitative data to paint a comprehensive picture of consumer behavior. Qualitative insights, such as focus group discussions or interviews, help uncover underlying motivations and concerns that quantitative data alone cannot capture. By combining these methodologies, market demand analysis can inform targeted strategies to increase influenza vaccine uptake, such as tailoring messaging to specific demographics or addressing logistical barriers to access. Ultimately, this analysis is essential for optimizing public health outcomes and ensuring that vaccination efforts align with consumer needs and preferences.
Pneumonia Vaccine: All Types Covered?
You may want to see also
Explore related products






![]()
Cost-Effectiveness Evaluation: Analyzes the economic impact and value of the vaccine in healthcare systems
The cost-effectiveness evaluation of the influenza vaccine is a critical component in assessing its economic impact and value within healthcare systems. This analysis involves comparing the costs associated with vaccine production, distribution, and administration against the health outcomes and financial savings it generates. By quantifying both direct medical costs (e.g., hospitalizations, outpatient visits) and indirect costs (e.g., productivity losses due to illness), policymakers can determine whether the vaccine provides a net economic benefit. For instance, studies often use metrics such as the incremental cost-effectiveness ratio (ICER), which measures the cost per quality-adjusted life year (QALY) gained, to assess the vaccine's value relative to other healthcare interventions.
In many markets, the influenza vaccine is measured through cost-effectiveness models that simulate the disease's transmission dynamics and the vaccine's impact on reducing morbidity and mortality. These models incorporate local epidemiological data, vaccine efficacy rates, and healthcare utilization patterns to estimate the potential cost savings. For example, preventing influenza cases reduces the burden on hospitals and clinics, freeing up resources for other critical care needs. Additionally, by minimizing absenteeism and productivity losses, the vaccine contributes to economic stability at both individual and societal levels. Such models are essential for justifying public health investments in vaccination programs.
Another key aspect of cost-effectiveness evaluation is the consideration of herd immunity, where high vaccination rates protect unvaccinated individuals by reducing disease spread. This indirect benefit is particularly valuable in vulnerable populations, such as the elderly or immunocompromised, who may not respond well to the vaccine. Economic analyses often account for these broader societal benefits, which can significantly enhance the vaccine's cost-effectiveness profile. For instance, a study might show that every dollar spent on influenza vaccination yields several dollars in savings by preventing outbreaks and reducing healthcare demand.
Cost-effectiveness evaluations also vary by market due to differences in healthcare infrastructure, disease burden, and vaccine pricing. In developed countries with higher healthcare costs, the economic benefits of vaccination may be more pronounced due to the high expenses associated with treating severe influenza cases. Conversely, in low-resource settings, the cost-effectiveness of the vaccine may depend on its affordability and accessibility. Policymakers must therefore tailor their evaluations to local contexts, considering factors such as vaccine coverage rates, population demographics, and existing healthcare policies.
Finally, the long-term economic impact of influenza vaccination extends beyond immediate healthcare savings. By reducing the prevalence of influenza, the vaccine can lower the risk of complications such as pneumonia or exacerbation of chronic conditions, which are costly to treat. Moreover, consistent vaccination programs can lead to decreased antibiotic use, mitigating the risk of antimicrobial resistance—a growing global health concern. These broader health and economic benefits underscore the importance of robust cost-effectiveness evaluations in guiding vaccine policy and ensuring sustainable healthcare systems.
Vaccine vs. Drug Testing: Key Differences and Safety Protocols
You may want to see also
Explore related products





![]()
Distribution Channel Performance: Tracks vaccine delivery efficiency through pharmacies, clinics, and other channels
The performance of distribution channels is a critical aspect of measuring the success and reach of the influenza vaccine in any market. Distribution Channel Performance focuses on tracking the efficiency and effectiveness of vaccine delivery through various channels, including pharmacies, clinics, hospitals, and public health centers. By analyzing these channels, stakeholders can identify bottlenecks, optimize logistics, and ensure timely access to vaccines for the population. Key metrics such as delivery timelines, stock availability, and wastage rates are monitored to gauge how well each channel performs in distributing the vaccine.
Pharmacies play a significant role in the distribution network, often serving as the most accessible point for individuals seeking vaccination. Performance tracking in pharmacies involves measuring the number of doses administered, the speed of distribution, and customer satisfaction levels. Data on vaccine uptake from pharmacies is cross-referenced with population density and demographic data to ensure equitable distribution. Additionally, monitoring stock levels and expiration dates helps prevent wastage and ensures a steady supply. Pharmacies that consistently meet or exceed distribution targets are identified as high-performing channels and may receive additional support or resources.
Clinics and hospitals are another vital distribution channel, particularly for high-risk groups such as the elderly, pregnant women, and individuals with chronic conditions. Performance in clinics and hospitals is measured by assessing the rate of vaccine administration, the efficiency of appointment scheduling, and the ability to handle large volumes of patients. Metrics such as the percentage of eligible patients vaccinated and the time taken from vaccine receipt to administration are crucial indicators of performance. Hospitals and clinics are also evaluated on their ability to manage cold chain requirements and minimize vaccine spoilage, as these facilities often handle larger quantities of doses.
Beyond traditional channels, alternative distribution methods such as mobile clinics, workplace vaccination programs, and community health fairs are increasingly being utilized to expand vaccine reach. Tracking performance in these channels involves measuring participation rates, geographic coverage, and the ability to target underserved populations. For example, mobile clinics are assessed based on their ability to reach remote or rural areas, while workplace programs are evaluated on employee participation rates. These alternative channels are particularly important for addressing gaps in vaccine access and ensuring comprehensive coverage across diverse populations.
To enhance overall distribution channel performance, data from all channels is aggregated and analyzed to identify trends, challenges, and opportunities for improvement. Advanced analytics tools are employed to predict demand, optimize inventory management, and allocate resources efficiently. Collaboration between public health authorities, distributors, and healthcare providers is essential to streamline processes and address inefficiencies. Regular performance reviews and feedback loops ensure that distribution strategies remain adaptive and responsive to changing market conditions, ultimately improving the effectiveness of influenza vaccine delivery.
Polio Vaccination in the 80s: What Happened?
You may want to see also
Explore related products





![]()
Adverse Event Monitoring: Evaluates safety by measuring reported side effects post-vaccination in the market
Adverse Event Monitoring (AEM) is a critical component of post-market surveillance for influenza vaccines, ensuring ongoing safety evaluation by systematically tracking and analyzing reported side effects. This process involves the collection of data from various sources, including healthcare providers, patients, and vaccine manufacturers, to identify potential safety signals. In most markets, AEM is conducted through national pharmacovigilance systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the United States or the Yellow Card Scheme in the United Kingdom. These systems rely on voluntary reporting, where healthcare professionals and individuals submit details of adverse events following vaccination. The data collected typically includes the type of vaccine administered, the timing of the adverse event, its severity, and any pre-existing medical conditions of the individual.
To ensure robust monitoring, regulatory agencies often collaborate with vaccine manufacturers to establish active surveillance programs. These programs may involve proactive follow-up with vaccinated individuals through surveys, electronic health records, or registries. For instance, the Centers for Disease Control and Prevention (CDC) in the U.S. utilizes the Vaccine Safety Datalink (VSD) to monitor adverse events in real-time by analyzing healthcare data from large populations. Such active surveillance complements passive reporting systems by providing more comprehensive and timely data, enabling quicker identification of rare or unexpected side effects.
The evaluation of reported adverse events involves a structured risk assessment process. Regulatory bodies, such as the Food and Drug Administration (FDA) or the European Medicines Agency (EMA), analyze the data to determine causality, frequency, and clinical significance of the events. Signal detection methods, including disproportionality analysis and statistical algorithms, are employed to identify patterns or clusters of adverse events that may warrant further investigation. If a potential safety signal is detected, additional studies, such as epidemiological investigations or clinical trials, may be conducted to confirm the association and assess the risk-benefit profile of the vaccine.
Transparency and communication are key aspects of AEM. Regulatory agencies regularly publish safety updates, summaries of adverse event reports, and risk management plans to inform healthcare providers, policymakers, and the public. This ensures that any emerging safety concerns are promptly addressed and that vaccination programs remain evidence-based. For example, during the 2009 H1N1 influenza pandemic, AEM played a pivotal role in quickly identifying and communicating the rare association between a specific vaccine and cases of narcolepsy, leading to adjustments in vaccination recommendations.
Continuous improvement of AEM systems is essential to enhance their effectiveness. This includes integrating advanced technologies, such as artificial intelligence and machine learning, to improve data analysis and signal detection. Additionally, efforts to increase reporting rates and improve data quality, such as training healthcare professionals and raising public awareness, are crucial. By maintaining a vigilant and adaptive AEM framework, markets can ensure the safety of influenza vaccines, build public trust, and support informed decision-making in immunization programs.
How Vaccines Activate Our B and T Cells
You may want to see also
Frequently asked questions
The effectiveness of the influenza vaccine is typically measured through observational studies, such as test-negative design studies, which compare the vaccination rates among individuals with laboratory-confirmed influenza to those without. These studies assess how well the vaccine prevents medically attended influenza illnesses in real-world settings.
Key metrics include vaccine effectiveness (VE), which measures the reduction in disease incidence among vaccinated individuals compared to unvaccinated individuals, and vaccine coverage rates, which indicate the proportion of the population that has received the vaccine. Additionally, seroprotection rates (antibody levels post-vaccination) are often assessed in clinical trials.
The market impact of the influenza vaccine is measured by evaluating its ability to reduce influenza-related hospitalizations, outpatient visits, and deaths. Public health surveillance systems, such as those maintained by the CDC or WHO, track these outcomes to assess the vaccine’s contribution to disease prevention and healthcare cost savings.