The spacing of vaccines, often referred to as the vaccination schedule, is a critical aspect of public health that ensures optimal immune response and protection against diseases. Determining how far apart to space vaccines involves careful consideration of factors such as the type of vaccine, the individual's age, immune status, and the specific disease being targeted. For instance, some vaccines, like those for measles, mumps, and rubella (MMR), are typically administered in multiple doses spaced weeks or months apart to allow the immune system to build a robust defense. In contrast, booster shots for vaccines like tetanus or influenza may be given years apart to maintain immunity. Proper spacing not only maximizes the effectiveness of each dose but also minimizes the risk of adverse reactions, making it a cornerstone of vaccination strategies worldwide.
Explore related products






What You'll Learn
- Age-Based Spacing: Different age groups may require varied vaccine spacing for optimal immune response
- Vaccine Type: Spacing varies between live, inactivated, mRNA, and viral vector vaccines
- Immune Status: Immunocompromised individuals may need adjusted spacing for safety and efficacy
- Disease Risk: High-risk areas may require closer spacing for faster protection
- Dose Intervals: Optimal time between doses ensures maximum immunity and minimal side effects
![]()
Age-Based Spacing: Different age groups may require varied vaccine spacing for optimal immune response
The immune system's response to vaccines is a delicate dance, and age plays a pivotal role in determining the optimal spacing between doses. For instance, infants and young children often receive multiple vaccine doses in close succession, such as the 2-month, 4-month, and 6-month schedules for vaccines like DTaP, Hib, and pneumococcal conjugate vaccine (PCV). This rapid spacing is designed to build immunity quickly during a period of heightened vulnerability to infectious diseases. However, this approach is not one-size-fits-all. As individuals age, their immune systems mature and respond differently, necessitating adjustments in vaccine spacing.
Consider the adolescent and adult populations. For vaccines like HPV (Human Papillomavirus), the Centers for Disease Control and Prevention (CDC) recommends a two-dose schedule for those initiating the series before their 15th birthday, with doses spaced 6–12 months apart. In contrast, individuals starting the series at ages 15 or older require a three-dose schedule, with the second dose administered 1–2 months after the first and the third dose 6 months after the first. This age-based differentiation highlights the immune system's evolving capacity to mount a robust response. The longer intervals for older adolescents and adults allow for a more sustained immune memory, which is crucial for long-term protection.
Practical implementation of age-based spacing requires careful planning and communication. For example, healthcare providers must ensure that parents and caregivers understand the importance of adhering to the recommended schedules for young children. Missed doses or incorrect spacing can compromise immunity, necessitating catch-up schedules that may involve additional doses or extended intervals. For older adults, particularly those receiving booster shots like the Tdap (Tetanus, Diphtheria, and Pertussis) or shingles vaccine, providers should emphasize the need for timely administration to maximize efficacy. A 2020 study in *Vaccine* found that Tdap efficacy waned significantly when the booster was delayed beyond the recommended 10-year interval, underscoring the critical role of age-appropriate spacing.
One compelling example of age-based spacing is the COVID-19 vaccine rollout. Initial studies showed that a 3–4 week interval between mRNA vaccine doses (Pfizer-BioNTech or Moderna) was effective for younger adults. However, research later suggested that extending this interval to 6–8 weeks could enhance immune response, particularly in older adults. This finding led some countries to adjust their dosing schedules, balancing the need for rapid protection with the benefits of optimized spacing. Such adaptations illustrate the dynamic nature of vaccine protocols and the importance of tailoring them to age-specific immune profiles.
In conclusion, age-based spacing is not merely a logistical consideration but a scientifically grounded strategy to enhance vaccine efficacy. From infancy to old age, the immune system’s unique characteristics at each life stage dictate the optimal timing between doses. Healthcare providers and policymakers must remain vigilant in updating guidelines based on emerging evidence, ensuring that vaccines are administered in a manner that maximizes protection across all age groups. By doing so, we can harness the full potential of immunization to safeguard public health.
Managing Vaccine Reactions: Steps to Take and When to Seek Help
You may want to see also
Explore related products






![]()
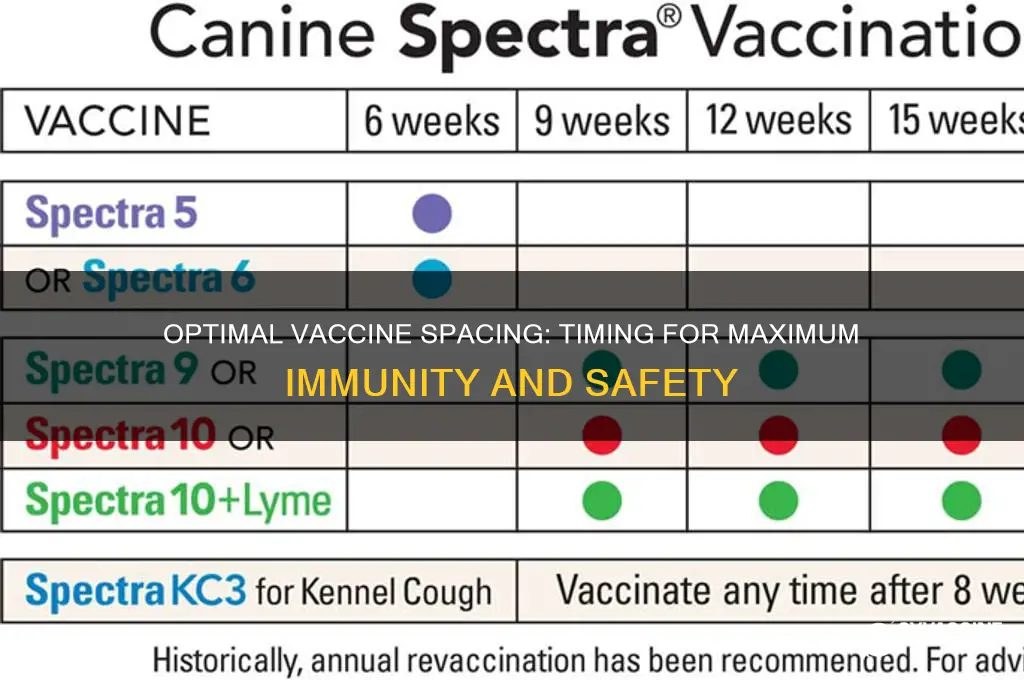
Vaccine Type: Spacing varies between live, inactivated, mRNA, and viral vector vaccines
The spacing between vaccine doses is not a one-size-fits-all approach. Different vaccine types—live, inactivated, mRNA, and viral vector—require distinct intervals to ensure optimal immune response and safety. For instance, live vaccines, such as the MMR (measles, mumps, rubella), typically need a minimum of 4 weeks between doses to prevent interference between the replicating viruses. This spacing allows the immune system to fully engage with the first dose before encountering the next, ensuring robust immunity.
In contrast, inactivated vaccines, like the seasonal flu shot, often permit shorter intervals, sometimes as little as 2 weeks, especially in high-risk populations or during outbreaks. This flexibility stems from their inability to replicate, reducing the risk of immunological competition. However, even with inactivated vaccines, age plays a role—infants and young children may require longer intervals to account for their developing immune systems. For example, the hepatitis A vaccine for children under 2 years old is typically spaced 6–18 months apart, while adults may receive doses 6–12 months apart.
MRNA vaccines, such as Pfizer-BioNTech and Moderna’s COVID-19 vaccines, have introduced new spacing considerations. Initial studies recommended 3–4 weeks between doses for maximum efficacy, but real-world data led to extended intervals of 6–8 weeks in some countries to balance supply constraints with immune response. Longer spacing has shown to enhance antibody production in certain age groups, particularly in younger adults. However, for immunocompromised individuals, shorter intervals are often maintained to ensure a quicker and more reliable immune response.
Viral vector vaccines, like AstraZeneca’s COVID-19 vaccine, present another unique case. The first and second doses are typically spaced 8–12 weeks apart to optimize the immune response. This longer interval allows the body to build a stronger memory response to the spike protein. However, in urgent situations, such as during a surge in cases, intervals as short as 4 weeks have been used, albeit with potentially reduced efficacy. Practical tips for recipients include scheduling reminders and ensuring access to the same vaccine type for both doses, as mixing viral vector vaccines is not universally recommended.
Understanding these spacing variations is crucial for healthcare providers and recipients alike. While guidelines provide a framework, individual factors like age, health status, and local disease prevalence may necessitate adjustments. Always consult a healthcare professional for personalized advice, as proper spacing maximizes protection while minimizing risks.
Understanding Tetanus Vaccine: Key Ingredients and Their Role in Protection
You may want to see also
Explore related products






![]()
Immune Status: Immunocompromised individuals may need adjusted spacing for safety and efficacy
Immunocompromised individuals face unique challenges when it comes to vaccination, as their weakened immune systems may not respond optimally to standard dosing schedules. For instance, a study on organ transplant recipients found that spacing COVID-19 vaccine doses 4–6 weeks apart, rather than the typical 3–4 weeks, improved antibody production without increasing adverse effects. This adjusted interval allows more time for immune cells to recognize and respond to the vaccine antigen, potentially enhancing protection in this vulnerable population.
Consider the case of a 52-year-old kidney transplant recipient on tacrolimus and mycophenolate mofetil. Standard vaccine spacing might leave them underprotected due to immunosuppression. By extending the interval between doses, clinicians can mitigate the risk of breakthrough infections while minimizing drug interactions that could further compromise efficacy. For vaccines requiring multiple doses, such as hepatitis B or HPV, immunocompromised patients may benefit from additional doses or alternative formulations, like higher antigen concentrations, to achieve adequate immunity.
Adjusting vaccine spacing is not a one-size-fits-all solution. Factors like the type of immunosuppression (e.g., HIV, chemotherapy, autoimmune disease treatment) and the specific vaccine (live attenuated vs. inactivated) must be considered. For example, live vaccines like MMR or varicella are generally contraindicated in severely immunocompromised individuals due to the risk of vaccine-strain infection. In contrast, mRNA vaccines, which do not contain live virus, can be safely administered but may require modified schedules to optimize response.
Practical tips for healthcare providers include consulting guidelines from organizations like the CDC or WHO, which often provide tailored recommendations for immunocompromised populations. For patients, maintaining open communication with their care team is crucial. Tracking antibody levels post-vaccination can help determine if additional doses or adjusted spacing are needed. Finally, combining vaccination with other protective measures, such as masking and social distancing, remains essential for this high-risk group until robust immunity is confirmed.
In conclusion, immunocompromised individuals require a nuanced approach to vaccine spacing to balance safety and efficacy. By personalizing schedules based on immune status, medical history, and vaccine type, healthcare providers can maximize protection for this vulnerable population. As research evolves, staying informed about updated guidelines will ensure the best possible outcomes for patients with weakened immune systems.
MMR Vaccine and mRNA: Debunking Myths About Its Composition
You may want to see also
Explore related products






![]()
Disease Risk: High-risk areas may require closer spacing for faster protection
In regions where disease outbreaks are imminent or ongoing, the standard vaccine schedule may not provide timely protection. For instance, during a measles outbreak, health authorities often recommend reducing the interval between the first and second doses of the MMR vaccine from the usual 28 days to as little as 4 weeks, ensuring faster immunity buildup. This accelerated schedule is particularly crucial for children aged 6–11 months, who are at higher risk of severe complications and may receive an early dose not counted toward the standard series.
The decision to shorten vaccine spacing hinges on balancing the risk of disease exposure against potential side effects. In high-risk areas, the benefits of rapid protection typically outweigh concerns like mild fever or soreness. For example, in cholera-endemic zones, the oral cholera vaccine (OCV) is sometimes administered with a 7-day interval between doses instead of the standard 14 days, as studies show this provides adequate immunity within a critical timeframe. However, such adjustments require careful monitoring by healthcare providers to ensure safety.
Practical implementation of closer vaccine spacing demands clear communication and logistical planning. Clinics in outbreak zones must prioritize rapid inventory turnover and educate communities about the urgency of adhering to the modified schedule. For instance, during a yellow fever outbreak, vaccination campaigns might administer fractional doses (e.g., 0.1 mL instead of 0.5 mL) to stretch supplies while maintaining efficacy, with doses spaced 10–14 days apart for accelerated coverage. Mobile clinics and door-to-door efforts often play a pivotal role in such scenarios.
While closer spacing can expedite protection, it is not a one-size-fits-all solution. Factors like vaccine type, age group, and local infrastructure influence feasibility. For example, inactivated vaccines (e.g., hepatitis A) may tolerate shorter intervals better than live-attenuated vaccines (e.g., varicella), which require more time for immune response. In remote areas with limited refrigeration, prioritizing single-dose vaccines or those stable at higher temperatures becomes essential. Tailoring strategies to local conditions ensures both speed and sustainability in high-risk settings.
Essential Vaccines for Your Baby's 2-Month Checkup: What to Expect
You may want to see also
Explore related products






![]()
Dose Intervals: Optimal time between doses ensures maximum immunity and minimal side effects
The timing between vaccine doses is a critical factor in the immune response, acting as a delicate balance between priming the immune system and allowing it to consolidate its memory. For instance, the Pfizer-BioNTech COVID-19 vaccine initially recommended a 3-week interval between doses, while AstraZeneca’s vaccine showed enhanced efficacy with a 12-week gap. These intervals are not arbitrary; they are rooted in immunological principles, such as the time required for B cells to mature into memory cells and for T cells to differentiate. Shorter intervals may risk immune interference, where the second dose fails to significantly boost the response, while longer intervals can lead to waning immunity if the pathogen is encountered prematurely.
Consider the practical implications for different age groups. Children and adolescents, with their robust immune systems, often tolerate shorter intervals, such as 3–4 weeks for the HPV vaccine. In contrast, older adults may benefit from extended intervals, like the 8-week gap recommended for shingles vaccines, to minimize side effects and ensure a stronger immune response. For pregnant individuals, spacing doses to avoid overlapping with critical fetal development stages is a consideration, though specific guidelines vary by vaccine and trimester. Always consult healthcare providers for personalized advice, as factors like underlying health conditions or local disease prevalence may influence optimal timing.
A persuasive argument for adhering to recommended dose intervals lies in the data. Studies on the Moderna COVID-19 vaccine demonstrated that extending the interval from 4 to 8 weeks increased antibody titers by up to 30%, with no significant increase in adverse reactions. Similarly, the meningococcal vaccine series for adolescents shows improved long-term immunity when doses are spaced 6 months apart rather than rushed. Deviating from these intervals—whether by shortening or prolonging them—can compromise both efficacy and safety, underscoring the importance of following evidence-based schedules.
To navigate dose intervals effectively, follow these actionable steps: First, verify the specific recommendations for your vaccine, as these vary widely (e.g., 21 days for Pfizer, 28 days for Moderna, 4–8 weeks for influenza). Second, mark your calendar and set reminders to avoid missing the optimal window. Third, if a dose is delayed, consult your healthcare provider; in many cases, the series can be resumed without restarting, though exceptions exist (e.g., rabies vaccines require strict adherence). Finally, monitor for side effects, as these can differ based on the interval—longer gaps may reduce systemic reactions like fatigue or fever. By respecting these intervals, you maximize the vaccine’s protective potential while minimizing discomfort.
Smallpox Vaccination: The US History and End Date
You may want to see also
Frequently asked questions
The recommended interval between COVID-19 vaccine doses varies depending on the specific vaccine and local guidelines. For example, the Pfizer-BioNTech and Moderna mRNA vaccines typically have a 3-4 week interval between doses, while the AstraZeneca vaccine may have a longer interval of 4-12 weeks. Always follow the advice of your healthcare provider or local health authority.
In general, it's safe to receive other vaccines, such as the flu shot, at the same time as your COVID-19 vaccine. However, if you prefer to space them out, the CDC recommends waiting at least 14 days before or after receiving the COVID-19 vaccine. Consult with your healthcare provider to determine the best schedule for your individual needs.
Live attenuated vaccines, such as the MMR (measles, mumps, and rubella) vaccine, should generally be spaced at least 4 weeks apart from other live attenuated vaccines. If you need to receive a non-live vaccine, like the flu shot or COVID-19 vaccine, it can be given at any time before or after a live attenuated vaccine.
Yes, it's essential to follow the recommended vaccine schedule for children to ensure optimal protection. The CDC and American Academy of Pediatrics provide guidelines for childhood vaccinations, which typically involve a series of shots spaced out over several months to years. For example, the DTaP (diphtheria, tetanus, and pertussis) vaccine is usually given at 2, 4, and 6 months of age, with booster shots at 15-18 months and 4-6 years. Always consult with your child's pediatrician to ensure they receive vaccines according to the recommended schedule.