The distribution of vaccines to states is a complex and coordinated effort involving federal, state, and local governments, as well as private sector partners. In the United States, the Centers for Disease Control and Prevention (CDC) and the Department of Health and Human Services (HHS) play a central role in allocating vaccine doses based on population size, vulnerability, and other factors. States then receive their allotted doses and are responsible for further distribution to local health departments, hospitals, pharmacies, and other designated vaccination sites. This process is guided by phased distribution plans, prioritizing high-risk groups such as healthcare workers, the elderly, and essential workers, before expanding to the general public. Logistics, including cold chain storage and transportation, are critical to ensuring vaccines remain effective, with companies like Pfizer and Moderna requiring ultra-cold storage for their mRNA vaccines. Transparency and equity are key principles, with efforts to address disparities in access and ensure fair distribution across diverse communities.
| Characteristics | Values |
|---|---|
| Allocation Method | Based on adult population (18+ years) as reported by the U.S. Census Bureau. |
| Distribution Frequency | Weekly allocations to states, territories, and select federal entities. |
| Vaccine Types Distributed | Pfizer-BioNTech, Moderna, Johnson & Johnson (Janssen), and Novavax. |
| Federal Pharmacy Partnership | Vaccines distributed to pharmacies (e.g., CVS, Walgreens) for direct administration. |
| State Flexibility | States determine allocation to local jurisdictions, healthcare providers, and priority groups. |
| Equity Considerations | Focus on underserved communities through programs like the Federal Retail Pharmacy Program. |
| Federal Entities Receiving Vaccines | Includes Veterans Health Administration, Department of Defense, and Bureau of Prisons. |
| Monitoring and Reporting | States report vaccine administration data to CDC via the Vaccine Administration Management System (VAMS). |
| Supply Chain Management | Coordinated by Operation Warp Speed (initially) and now by the CDC and state health departments. |
| Cold Chain Requirements | Ultra-cold storage for Pfizer, standard refrigeration for Moderna and J&J. |
| Latest Data Source | CDC COVID-19 Vaccination Program (as of October 2023). |
Explore related products






What You'll Learn
- Federal Allocation Formula: Population, risk factors, and equity determine each state's vaccine supply share
- State Distribution Plans: States prioritize groups (e.g., healthcare workers, elderly) based on local needs
- Logistics & Storage: Cold chain requirements and transportation ensure vaccine viability during delivery
- Provider Enrollment: Hospitals, pharmacies, and clinics register to receive and administer vaccines
- Monitoring & Adjustments: Data on distribution and uptake guide reallocation to high-demand areas
![]()
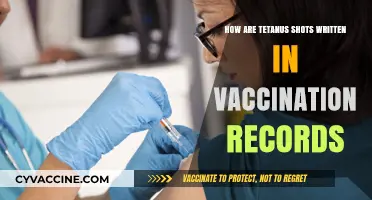
Federal Allocation Formula: Population, risk factors, and equity determine each state's vaccine supply share
The distribution of COVID-19 vaccines to U.S. states is guided by a Federal Allocation Formula that prioritizes fairness, population needs, and risk mitigation. At its core, this formula ensures that each state receives a vaccine supply share proportional to its population size. This approach acknowledges that larger states have more residents to vaccinate and thus require a greater volume of doses. The Centers for Disease Control and Prevention (CDC) and the Department of Health and Human Services (HHS) use census data to calculate allocations, ensuring a baseline of equity across states. Population-based distribution serves as the foundation for all vaccine allocations, providing a transparent and objective starting point.
Beyond population, the formula incorporates risk factors to address disparities and protect vulnerable populations. This includes prioritizing states with higher rates of COVID-19 cases, hospitalizations, and deaths. Additionally, the formula considers the presence of high-risk groups, such as healthcare workers, elderly populations, and individuals with underlying health conditions. By factoring in these risks, the federal government aims to direct vaccines to areas where they can have the greatest impact in reducing severe outcomes and alleviating strain on healthcare systems. This risk-based component ensures that states facing more significant public health challenges receive commensurate support.
Equity is another critical pillar of the federal allocation formula, designed to address systemic disparities in healthcare access and outcomes. The formula accounts for social vulnerability indices, which measure factors like poverty, lack of access to transportation, and crowded housing. States with higher social vulnerability scores receive additional vaccine doses to ensure marginalized communities are not left behind. This equity-focused approach aligns with broader public health goals of reducing health disparities and promoting justice in vaccine distribution. It also reflects lessons learned from early distribution challenges, where underserved communities faced barriers to accessing vaccines.
The federal government periodically adjusts the allocation formula to reflect evolving pandemic conditions and vaccine supply. For instance, as new variants emerge or vaccination rates plateau in certain areas, the formula may be fine-tuned to prioritize states experiencing outbreaks or lagging in immunization coverage. These adjustments ensure that the distribution remains responsive to real-time data and public health needs. States are informed of their allocations through regular updates from the CDC and HHS, allowing them to plan their vaccination campaigns effectively.
In summary, the Federal Allocation Formula for vaccine distribution is a multifaceted system that balances population size, risk factors, and equity considerations. By prioritizing these elements, the federal government aims to ensure that vaccines are distributed fairly and effectively across all states. This formula not only addresses immediate public health needs but also works to rectify long-standing inequities in healthcare access. As the pandemic continues to evolve, this adaptive and data-driven approach remains essential for achieving widespread immunity and protecting the nation’s health.
Evaluating the Success of Childhood Vaccination Programs: A Comprehensive Review
You may want to see also
Explore related products






![]()
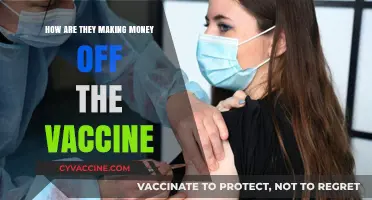
State Distribution Plans: States prioritize groups (e.g., healthcare workers, elderly) based on local needs
The distribution of COVID-19 vaccines to states is a complex process that involves careful planning and prioritization based on local needs. Each state has developed its own distribution plan, taking into account factors such as population demographics, healthcare infrastructure, and disease prevalence. At the core of these plans is the prioritization of specific groups, such as healthcare workers, the elderly, and individuals with underlying medical conditions, who are at higher risk of severe illness or death from COVID-19. States receive vaccine allocations from the federal government based on their population size, and it is up to each state to determine how to distribute these doses in a fair and efficient manner.
States prioritize groups based on a combination of federal guidelines and local data. The Centers for Disease Control and Prevention (CDC) has provided a framework for vaccine distribution, which recommends prioritizing healthcare personnel, long-term care facility residents, frontline essential workers, and individuals aged 75 and older in the initial phases of distribution. However, states have the flexibility to adapt these guidelines to meet their specific needs. For example, some states may choose to prioritize teachers or grocery store workers earlier in the distribution process if they determine that these groups are at particularly high risk in their communities. By tailoring their distribution plans to local conditions, states can ensure that the limited vaccine supply is used to maximum effect.
!)
One key aspect of state distribution plans is the use of phased approaches to prioritize different groups over time. Most states have implemented a multi-phase system, with each phase focusing on specific populations or occupational groups. For instance, Phase 1a typically includes healthcare workers and long-term care facility residents, while Phase 1b may expand to include frontline essential workers, individuals aged 75 and older, and those with high-risk medical conditions. As more vaccine doses become available, states can move into subsequent phases, gradually expanding eligibility to larger segments of the population. This phased approach allows states to balance the urgent need to protect the most vulnerable with the goal of achieving widespread immunity over time.
To implement their distribution plans, states rely on a variety of strategies and partnerships. Many states have established regional or local vaccination sites, such as hospitals, pharmacies, and community health centers, to administer doses to prioritized groups. Some states have also implemented mass vaccination events or mobile clinics to reach underserved or rural populations. Additionally, states work closely with local health departments, healthcare providers, and community organizations to identify and reach priority groups, provide education and outreach, and address vaccine hesitancy. By leveraging these partnerships, states can ensure that their distribution plans are implemented effectively and equitably.
Monitoring and evaluating the distribution process is crucial to ensuring that states are meeting their goals and adapting to changing conditions. States track vaccine administration data, including the number of doses administered, the characteristics of vaccinated individuals, and any adverse events reported. This data is used to identify areas where distribution efforts may be falling short, such as disparities in access among certain racial or ethnic groups, and to make adjustments to the distribution plan as needed. States also provide regular updates to the public on the status of vaccine distribution, including information on eligibility criteria, vaccination sites, and appointment scheduling. By maintaining transparency and accountability, states can build trust and confidence in the vaccination process, which is essential for achieving widespread immunity and ending the pandemic.
As vaccine distribution continues to ramp up, states face ongoing challenges in prioritizing groups and allocating doses effectively. The emergence of new COVID-19 variants, fluctuations in vaccine supply, and evolving scientific guidance all require states to remain flexible and responsive in their planning. Furthermore, addressing disparities in vaccine access and uptake among marginalized communities remains a critical priority. States must continue to engage with community leaders, address language and cultural barriers, and implement targeted outreach and education efforts to ensure that all populations have equitable access to the vaccine. By prioritizing the needs of their local communities and adapting to changing circumstances, states play a vital role in the successful distribution of COVID-19 vaccines and the ultimate goal of protecting public health.
RSV Vaccine: What's in a Name?
You may want to see also
Explore related products

$97.71 $103





![]()
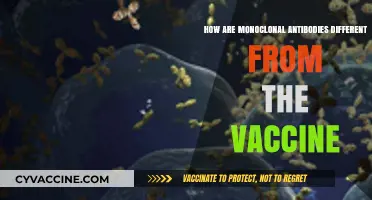
Logistics & Storage: Cold chain requirements and transportation ensure vaccine viability during delivery
The distribution of vaccines to states is a complex process that heavily relies on robust logistics and storage systems, particularly the maintenance of the cold chain, to ensure vaccine viability during delivery. Vaccines are temperature-sensitive biological products that require specific storage and handling conditions to remain effective. The cold chain is a temperature-controlled supply chain that ensures vaccines are kept at the recommended temperatures from the point of manufacture to the point of administration. For most vaccines, including many COVID-19 vaccines, this means storage between 2°C and 8°C (36°F and 46°F), with some requiring ultra-cold temperatures as low as -70°C (-94°F).
To maintain the integrity of the cold chain, specialized equipment and procedures are employed. Refrigerators, freezers, and ultra-cold freezers are used to store vaccines at the appropriate temperatures. These units are equipped with temperature monitoring devices that continuously track and record internal temperatures, ensuring any deviations are promptly addressed. Additionally, insulated containers and cold boxes are used during transportation to maintain the required temperature range, especially for last-mile delivery to remote or rural areas. These containers are often packed with dry ice or gel packs to provide additional cooling and stability.
Transportation of vaccines is another critical aspect of the logistics process. Vaccines are shipped via air, ground, or a combination of both, depending on the distance and urgency. For ultra-cold chain vaccines, specialized carriers with temperature-controlled units are utilized to ensure the vaccines remain within the required temperature range throughout transit. The transportation process is meticulously planned to minimize exposure to temperature fluctuations, which can compromise vaccine efficacy. This includes optimizing routes, reducing transit times, and ensuring seamless handoffs between different modes of transportation.
At the state and local levels, receiving and storing vaccines require careful coordination and infrastructure. States have designated vaccine storage facilities equipped with the necessary refrigeration units and backup power systems to prevent temperature excursions during power outages. These facilities are strategically located to facilitate distribution to local health departments, hospitals, clinics, and vaccination sites. Personnel involved in vaccine handling are trained in cold chain management, including proper packing, unpacking, and storage procedures, to minimize the risk of temperature breaches.
Monitoring and oversight are integral to ensuring the cold chain is maintained throughout the distribution process. Federal and state health agencies use temperature monitoring systems and data loggers to track vaccine conditions in real time. Any deviations from the required temperature range trigger immediate corrective actions, such as relocating vaccines to functional storage units or discarding compromised doses. Regular audits and inspections of storage facilities and transportation processes are conducted to ensure compliance with cold chain guidelines and identify areas for improvement.
Finally, collaboration between federal, state, and local authorities, as well as private sector partners, is essential for successful vaccine distribution. The federal government allocates vaccines to states based on population and other criteria, while states are responsible for further distributing doses to local jurisdictions. Public-private partnerships play a crucial role in providing the necessary logistics infrastructure, including transportation networks and storage facilities. By working together, these entities ensure that vaccines are delivered efficiently, safely, and in a manner that preserves their viability, ultimately enabling widespread vaccination efforts.
Coronavirus Vaccine: Microchip Myth Debunked
You may want to see also
Explore related products






![]()
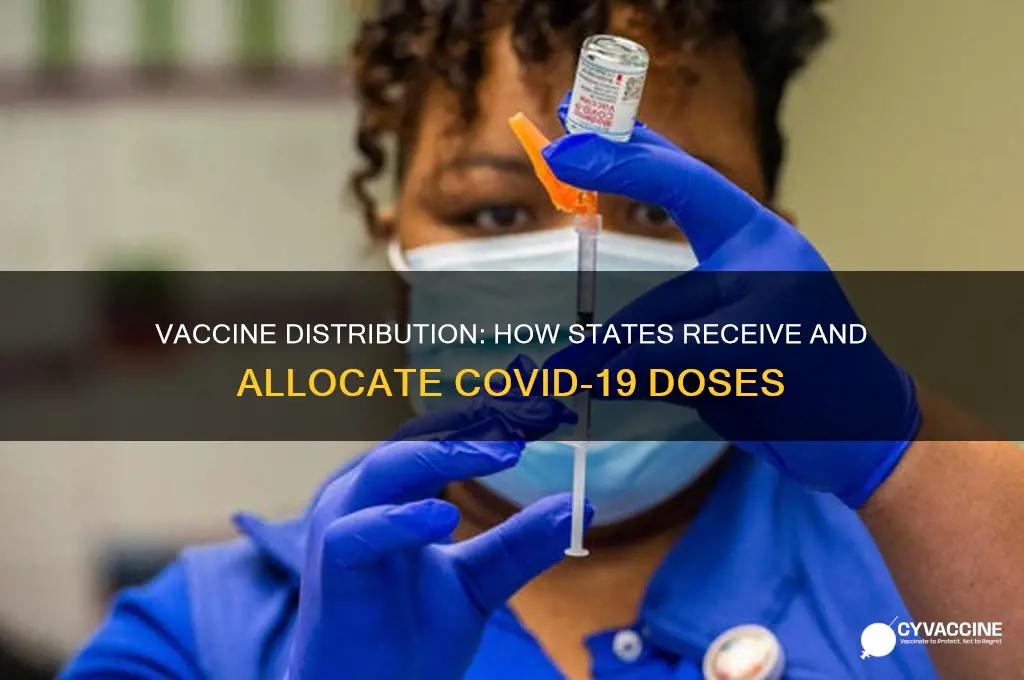
Provider Enrollment: Hospitals, pharmacies, and clinics register to receive and administer vaccines
Provider enrollment is a critical step in the vaccine distribution process, ensuring that hospitals, pharmacies, and clinics are equipped and authorized to receive and administer vaccines. This process begins with healthcare providers registering through state health departments or designated immunization programs. Each state has established specific criteria and procedures for enrollment, often requiring providers to meet certain standards, such as having adequate storage facilities for vaccines, trained staff, and a plan for managing vaccine administration and reporting. Providers must complete an application that includes details about their facility, staffing, and capacity to handle vaccine distribution. This ensures that only qualified and prepared entities are included in the distribution network.
Once registered, providers are typically assigned to a tier or priority group based on their role in the healthcare system and their ability to reach target populations. For example, large hospitals and health systems may be prioritized for early vaccine allocation due to their capacity to handle high volumes and their role in treating COVID-19 patients. Similarly, pharmacies, especially those in underserved or rural areas, play a vital role in expanding access to vaccines. Clinics, including community health centers and federally qualified health centers (FQHCs), are also key participants, as they often serve vulnerable populations and have established relationships with their communities. This tiered approach ensures that vaccines are distributed efficiently and equitably across different provider types.
The enrollment process also involves providers agreeing to specific terms and conditions, such as adhering to federal and state guidelines for vaccine storage, handling, and administration. Providers must commit to reporting vaccine administration data promptly and accurately, which is crucial for monitoring distribution and coverage rates. Many states require providers to use designated immunization information systems (IIS) or platforms to track vaccine inventory and administration. This data is then shared with state and federal authorities to ensure transparency and accountability in the distribution process. Compliance with these requirements is essential for providers to remain eligible to receive vaccine allocations.
Training and education are integral components of provider enrollment. Before receiving vaccines, healthcare providers and their staff must complete mandatory training on vaccine handling, administration techniques, and managing potential adverse reactions. This training is often provided through state health departments, the Centers for Disease Control and Prevention (CDC), or other authorized entities. Additionally, providers are given resources and guidelines to educate their patients about the vaccines, including information on efficacy, safety, and the importance of completing the vaccination series. This ensures that providers are not only capable of administering vaccines but also of addressing patient concerns and promoting vaccine confidence.
Finally, provider enrollment is an ongoing process that adapts to the evolving needs of the vaccination campaign. As new vaccines become available or as distribution priorities shift, providers may need to update their enrollment information or reapply to continue receiving allocations. States also conduct periodic reviews to assess provider performance, ensuring that they are meeting distribution goals and maintaining compliance with guidelines. This dynamic approach allows the distribution network to remain flexible and responsive to changes in vaccine supply, demand, and public health priorities. By carefully managing provider enrollment, states can ensure a robust and efficient system for delivering vaccines to their populations.
Grocery Workers: Who Gets Vaccinated?
You may want to see also
Explore related products






![]()
Monitoring & Adjustments: Data on distribution and uptake guide reallocation to high-demand areas
The distribution of vaccines to states is a dynamic process that relies heavily on real-time data monitoring and strategic adjustments to ensure equitable and efficient allocation. Central to this process is the continuous tracking of vaccine distribution and uptake, which provides critical insights into where vaccines are being administered and how quickly they are being used. Federal agencies, such as the Centers for Disease Control and Prevention (CDC) and the Department of Health and Human Services (HHS), collaborate with state and local health departments to collect and analyze this data. By monitoring metrics like the number of doses shipped, administered, and remaining in inventory, officials can identify trends and disparities in vaccine distribution across regions.
Data on vaccine uptake is particularly crucial for guiding reallocation efforts to high-demand areas. Uptake rates, which measure the percentage of delivered doses that have been administered, highlight regions where demand outpaces supply or where logistical challenges are hindering distribution. For instance, if a state reports high demand but low uptake, it may indicate issues such as insufficient staffing, storage limitations, or hesitancy among the population. Conversely, areas with high uptake and persistent demand are prioritized for additional shipments to meet the needs of their populations. This data-driven approach ensures that vaccines are not left unused in one area while another faces shortages.
To facilitate these adjustments, federal authorities use predictive analytics and demand forecasting models to anticipate future needs. These models consider factors such as population size, infection rates, and demographic vulnerabilities to project where vaccines will be most needed in the coming weeks. For example, if a surge in cases is predicted in a specific region, additional doses can be preemptively allocated to that area to mitigate the outbreak. Similarly, areas with high vaccination rates and declining demand may see their allocations reduced, with doses redirected to regions with greater need.
Transparency and communication are essential components of this monitoring and adjustment process. State and local health departments receive regular updates on their allocations and are encouraged to provide feedback on their specific needs and challenges. This two-way communication ensures that federal decisions are informed by on-the-ground realities. Additionally, public dashboards and reports are often made available to track distribution and uptake at the state and county levels, fostering accountability and public trust in the process.
Finally, the ability to quickly reallocate vaccines based on real-time data is a key strength of the distribution system. For example, if a state experiences a sudden spike in demand due to a localized outbreak or increased public interest, federal authorities can swiftly redirect doses from areas with surplus inventory. This flexibility is supported by robust logistics networks, including partnerships with private distributors and the strategic placement of vaccine stockpiles in regional hubs. By continuously monitoring distribution and uptake data, the system can adapt to changing circumstances, ensuring that vaccines reach those who need them most.
Vaccination Requirements for Attending Live Concerts
You may want to see also
Frequently asked questions
COVID-19 vaccines are allocated to states based on population size, with adjustments made for specific needs such as healthcare worker prioritization, equity considerations, and local demand. The federal government, through the CDC, determines the allocation formula and works with state health departments to distribute doses accordingly.
Each state’s health department, in collaboration with local health authorities, decides the distribution plan. States follow federal guidelines but have flexibility to prioritize specific groups (e.g., healthcare workers, seniors) and allocate vaccines to providers like hospitals, pharmacies, and community clinics based on local needs.
Vaccines are transported through a federal partnership with private distributors like McKesson Corporation. Specialized cold chain logistics ensure proper storage, especially for mRNA vaccines requiring ultra-cold temperatures. States and providers receive shipments directly, with monitoring systems in place to maintain vaccine integrity during transit and storage.