If you're wondering whether you've received the polio vaccine, it’s important to consider your age, location, and vaccination history. Polio vaccination has been a standard part of childhood immunization schedules in many countries for decades, typically administered as part of the inactivated poliovirus vaccine (IPV) or oral poliovirus vaccine (OPV). Most individuals born after the mid-20th century in regions with robust healthcare systems likely received the vaccine as part of routine childhood immunizations. To confirm your vaccination status, check your medical records, immunization card, or consult with a healthcare provider. If you’re unsure or at risk of exposure, especially when traveling to areas where polio still exists, it’s advisable to discuss vaccination options with a healthcare professional.
Explore related products






What You'll Learn
- Vaccine Schedule: When and how many doses of the polio vaccine are required for full protection
- Vaccine Types: Difference between inactivated (IPV) and oral (OPV) polio vaccines
- Side Effects: Common and rare reactions to the polio vaccine
- Effectiveness: How well the polio vaccine prevents the disease
- Global Eradication: Progress and challenges in eliminating polio worldwide
![]()
Vaccine Schedule: When and how many doses of the polio vaccine are required for full protection
The polio vaccine schedule is a critical component of ensuring lifelong immunity against this debilitating disease. In the United States, the Centers for Disease Control and Prevention (CDC) recommends a series of four doses, typically administered at specific intervals during early childhood. The first dose is given at 2 months of age, followed by subsequent doses at 4 months, 6-18 months, and 4-6 years. This schedule is designed to establish a robust immune response, providing near-complete protection against all three types of poliovirus.
Analyzing the Dosing Regimen
Each dose of the inactivated poliovirus vaccine (IPV) contains a precise amount of viral antigens to stimulate the immune system without causing the disease. The initial doses in infancy prime the immune system, while later doses reinforce immunity, ensuring long-term protection. For example, the 4-month dose builds on the first, and the 6-18 month dose further solidifies this foundation. The final dose, given before school entry, acts as a booster, maximizing immunity during a critical developmental period. This staggered approach mirrors the body’s natural immune response, creating a durable defense against polio.
Practical Tips for Parents and Caregivers
Adhering to the polio vaccine schedule requires planning and awareness. Keep a record of your child’s immunizations, either through a personal health log or a digital tool like the CDC’s immunization tracker. Schedule appointments in advance, especially for the 4-6 year booster, which can coincide with other school-entry vaccinations. If a dose is missed, consult your healthcare provider to resume the schedule without restarting it. Remember, delays do not render previous doses ineffective, but timely completion ensures optimal protection.
Comparing Global Schedules
While the U.S. schedule is standardized, variations exist globally. In some countries, oral poliovirus vaccine (OPV) is used alongside or instead of IPV, often in regions with higher polio prevalence. For instance, the World Health Organization (WHO) recommends a primary series of three OPV doses starting at 6 weeks of age, followed by IPV boosters. Travelers or those moving between countries should verify their vaccination status and consult health authorities to ensure compliance with local requirements. This highlights the importance of understanding regional differences in vaccine protocols.
The Takeaway: Full Protection is Achievable
Completing the full polio vaccine schedule is non-negotiable for eradicating this disease. Each dose plays a unique role in building and maintaining immunity. For adults unsure of their vaccination status, a blood test can determine immunity levels, though catching up on missed doses is generally safe and effective. By following the recommended schedule, individuals not only protect themselves but also contribute to global polio eradication efforts. In a world where vaccine-preventable diseases persist, staying informed and proactive is a responsibility we all share.
Post-Covishield Care: Essential Steps for Recovery and Well-being
You may want to see also
Explore related products






![]()
Vaccine Types: Difference between inactivated (IPV) and oral (OPV) polio vaccines
Polio vaccines have eradicated the disease in most countries, but the choice between inactivated (IPV) and oral (OPV) versions remains critical. Understanding their differences ensures informed decisions for individuals and public health strategies. IPV, administered through injection, contains killed poliovirus, offering robust protection without the risk of vaccine-derived polio. OPV, delivered orally, uses weakened live virus, providing gut immunity but carrying a rare risk of reversion to a virulent form. Both vaccines target the same disease but differ fundamentally in composition, administration, and safety profiles.
From an analytical perspective, IPV’s inactivated nature makes it safer for immunocompromised individuals, as it cannot cause polio. It is typically given in a series of 3-4 doses, starting at 2 months of age, with boosters recommended for travelers to polio-endemic regions. OPV, on the other hand, is cheaper and easier to administer, making it ideal for mass vaccination campaigns in low-resource settings. However, its live virus component can, in rare cases (1 in 2.7 million), cause vaccine-associated paralytic polio (VAPP). This risk, though minuscule, has led many high-income countries to switch exclusively to IPV.
Persuasively, the choice between IPV and OPV often hinges on context. In regions with strong healthcare infrastructure, IPV’s safety and efficacy make it the preferred choice. For global eradication efforts, OPV’s ability to induce mucosal immunity and interrupt wild poliovirus transmission remains invaluable. Combining both vaccines in a sequenced schedule (e.g., OPV for initial doses and IPV for boosters) maximizes benefits while minimizing risks, a strategy adopted by some countries to balance individual and herd immunity.
Comparatively, IPV’s injection route ensures consistent dosing but requires trained healthcare workers, while OPV’s oral delivery simplifies administration, especially in remote areas. Dosage-wise, IPV is given in 0.5 mL intramuscular injections, whereas OPV is administered as 2 drops (0.1 mL) for infants and children. Cost-effectiveness favors OPV, but IPV’s safety record justifies its higher expense in settings where VAPP risk is unacceptable. Practical tips include verifying vaccination records to determine which vaccine was received and consulting healthcare providers for travel-specific recommendations.
In conclusion, the inactivated (IPV) and oral (OPV) polio vaccines serve complementary roles in the fight against polio. IPV’s safety and reliability suit individual protection, particularly in developed nations, while OPV’s ease of use and mucosal immunity make it a cornerstone of global eradication efforts. Understanding these differences empowers individuals and policymakers to make evidence-based choices, ensuring polio remains a disease of the past.
Need to Register for the Vaccine? Here’s the Number to Call
You may want to see also
Explore related products






![]()
Side Effects: Common and rare reactions to the polio vaccine
The polio vaccine, a cornerstone of modern medicine, has virtually eradicated a once-feared disease. Yet, like any medical intervention, it carries the potential for side effects. Understanding these reactions—both common and rare—is crucial for informed decision-making and peace of mind.
Common side effects are generally mild and short-lived. Soreness, redness, or swelling at the injection site is typical, especially with the inactivated polio vaccine (IPV), the version used in most countries today. These localized reactions usually resolve within a few days and can be managed with cold compresses and over-the-counter pain relievers like acetaminophen. Fatigue, headache, and low-grade fever may also occur, mimicking a mild flu-like state. These systemic symptoms are more common in children and typically subside within 24-48 hours.
Rare but serious side effects are exceptionally uncommon with IPV. Severe allergic reactions, characterized by difficulty breathing, swelling of the face or throat, and rapid heartbeat, require immediate medical attention. Anaphylaxis, though rare, is a medical emergency. Another rare complication is shoulder injury related to vaccine administration (SIRVA), which can cause persistent pain and limited range of motion. This is more likely to occur with improper injection technique, emphasizing the importance of trained healthcare professionals administering the vaccine.
The oral polio vaccine (OPV), still used in some regions, carries a minuscule risk of vaccine-associated paralytic polio (VAPP). This occurs when the weakened virus in the vaccine reverts to a virulent form and causes paralysis. The risk of VAPP is approximately 1 in 2.7 million doses, highlighting the vaccine's remarkable safety profile. However, this risk has led to the global shift towards IPV, which cannot cause polio.
Understanding the balance between risk and benefit is paramount. The polio vaccine's efficacy in preventing a devastating disease far outweighs the potential for side effects. The vast majority of individuals experience no adverse reactions, and even common side effects are mild and transient. By being aware of possible reactions, individuals can make informed choices and seek prompt medical attention if necessary, ensuring the continued success of polio eradication efforts.
Polio Vaccine: Aluminum and Its Presence
You may want to see also
Explore related products






![]()
Effectiveness: How well the polio vaccine prevents the disease
The polio vaccine stands as one of the most effective tools in modern medicine, nearly eradicating a disease that once paralyzed or killed thousands annually. Its success hinges on its ability to stimulate the immune system to produce antibodies against the poliovirus, preventing infection and halting transmission. Two types of vaccines exist: the inactivated poliovirus vaccine (IPV), administered through injection, and the oral poliovirus vaccine (OPV), given as drops. Both have proven highly effective, with IPV offering 90-100% protection after a complete series of doses, typically three shots given at 2 months, 4 months, and 6-18 months of age, followed by a booster at 4-6 years. OPV, while slightly less effective in individuals, excels at interrupting viral spread in communities, making it a cornerstone of global eradication efforts.
Consider the real-world impact: since the introduction of the polio vaccine in the 1950s, global cases have plummeted by over 99%. Countries that maintain high vaccination rates have eliminated the disease entirely. For instance, the Americas were declared polio-free in 1994, thanks to rigorous vaccination campaigns. However, effectiveness isn’t just about individual immunity; it’s also about herd immunity, which protects those who cannot be vaccinated due to medical reasons. A single missed dose or low community coverage can leave gaps, allowing the virus to resurge, as seen in rare outbreaks in under-vaccinated regions.
To ensure maximum protection, adherence to the recommended schedule is critical. For adults unsure of their vaccination status, a blood test can check for polio antibodies, though most born after the mid-20th century likely received the vaccine as children. If immunity is absent or uncertain, a catch-up series of IPV doses can be administered. Travelers to polio-endemic areas should receive a one-time booster, even if previously vaccinated, to reduce the risk of contracting or spreading the virus. Practical tips include keeping a vaccination record, consulting healthcare providers for personalized advice, and staying informed about global polio eradication efforts.
Comparing the polio vaccine to others highlights its exceptional efficacy. While vaccines like the flu shot require annual updates due to viral mutations, the polio vaccine provides lifelong immunity after a complete series. Its success underscores the importance of consistent public health strategies, including accessible healthcare, education, and global cooperation. The polio vaccine’s effectiveness isn’t just a medical triumph—it’s a testament to what humanity can achieve when science and solidarity align. By understanding its role and ensuring widespread coverage, we can sustain a world where polio remains a relic of the past.
Unraveling the Myth: Who Spread False Autism-Vaccine Claims?
You may want to see also
Explore related products






![]()
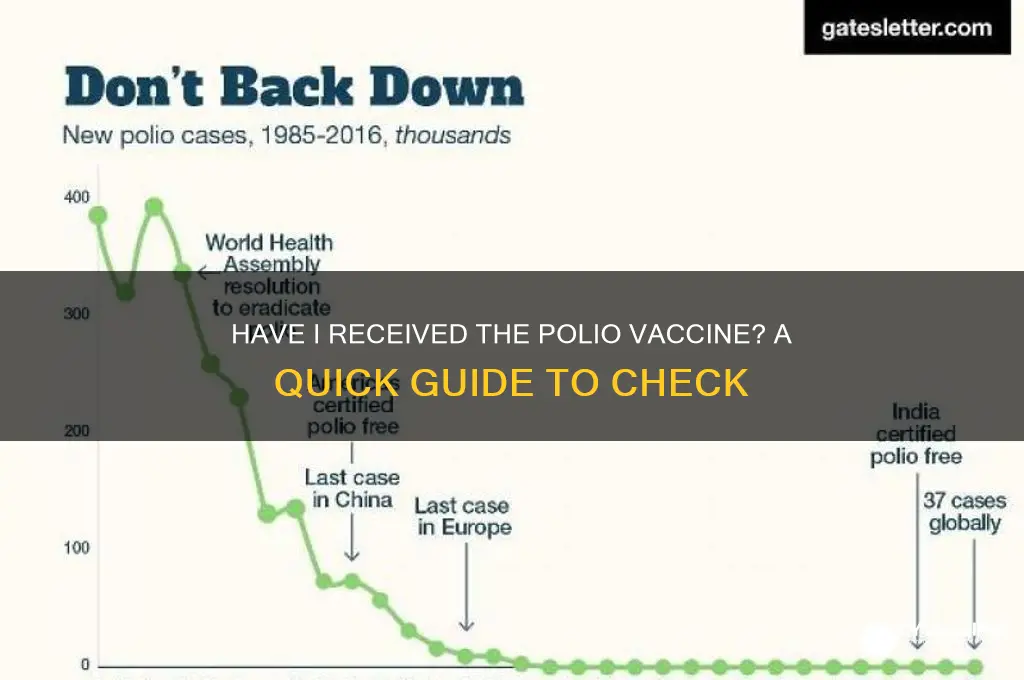
Global Eradication: Progress and challenges in eliminating polio worldwide
Polio, once a global scourge paralyzing hundreds of thousands annually, stands on the brink of eradication thanks to decades of concerted international efforts. The Global Polio Eradication Initiative (GPEI), launched in 1988, has reduced polio cases by 99.9%, from an estimated 350,000 cases in 125 countries to a mere handful in just two endemic nations today: Afghanistan and Pakistan. This monumental progress is a testament to the power of vaccination campaigns, community engagement, and political commitment. The oral polio vaccine (OPV), administered in multiple doses starting at 6 weeks of age, has been the cornerstone of this success, providing both individual and herd immunity. However, the final mile to eradication remains fraught with challenges that threaten to undo decades of work.
One of the most significant hurdles is vaccine hesitancy, fueled by misinformation, cultural barriers, and geopolitical instability. In regions like the Afghanistan-Pakistan border, where polio remains endemic, access to children for vaccination is often blocked by conflict, mistrust, or logistical difficulties. For instance, rumors linking the vaccine to infertility or Western conspiracies have led some communities to reject immunization efforts outright. Addressing these concerns requires culturally sensitive communication strategies, involving local leaders and health workers to build trust. Additionally, the shift from trivalent OPV to bivalent OPV in 2016, while necessary to prevent vaccine-derived polio cases, introduced new complexities in vaccine supply chains and public understanding.
Another critical challenge is the risk of polio re-emerging in previously polio-free regions due to gaps in immunization coverage. In 2021, Malawi and Mozambique reported cases of wild poliovirus, and several countries have seen outbreaks of circulating vaccine-derived poliovirus (cVDPV). These incidents highlight the importance of maintaining high vaccination rates globally, even in areas where polio has been eradicated. The inactivated polio vaccine (IPV), often used in combination with OPV in some countries, provides additional protection but is more expensive and requires injection, making it less accessible in resource-limited settings. Strengthening routine immunization systems and conducting targeted vaccination campaigns are essential to prevent backsliding.
Despite these challenges, innovative strategies offer hope for the final push toward eradication. For example, the use of satellite imagery and geospatial mapping has improved the precision of vaccination campaigns, ensuring that even remote populations are reached. Mobile health teams, often composed of local volunteers, have been instrumental in delivering vaccines in conflict zones. Moreover, the integration of polio eradication efforts with broader health initiatives, such as maternal and child health programs, has maximized impact and sustainability. The lessons learned from polio eradication—such as the importance of community engagement, data-driven decision-making, and global collaboration—provide a blueprint for tackling other infectious diseases.
In conclusion, the global eradication of polio is within reach, but it demands unwavering commitment, innovation, and resources. As individuals, knowing whether you’ve received the polio vaccine is not just a personal health concern but a contribution to a global effort. If you’re unsure, consult your vaccination records or healthcare provider, especially if you’re traveling to or from polio-endemic regions. For children, ensure they complete the full series of polio vaccinations, typically 3-4 doses of OPV or a combination of IPV and OPV, depending on the country’s schedule. By staying informed and vaccinated, we can all play a part in consigning polio to history.
Monsanto, Merck, and Glyphosate: The Vaccine Connection?
You may want to see also
Frequently asked questions
Check your immunization records or contact your healthcare provider. They can review your medical history and determine if you've been vaccinated against polio.
The polio vaccine typically requires multiple doses for full protection. The exact number of doses depends on the type of vaccine (inactivated poliovirus vaccine or oral poliovirus vaccine) and your age at the time of vaccination.
While the polio vaccine is highly effective, no vaccine provides 100% protection. However, vaccination significantly reduces your risk of contracting polio. In countries with high vaccination rates, polio has been nearly eradicated.
In most cases, adults who completed the full polio vaccine series as children do not need a booster. However, if you're traveling to an area with ongoing polio transmission or work in a high-risk profession (e.g., healthcare), your healthcare provider may recommend a booster dose.