Understanding whether you have been vaccinated against polio is crucial for your health and public safety, as polio is a highly contagious viral disease that can lead to paralysis or even death. Vaccination against polio is typically administered during childhood as part of routine immunization schedules, with the inactivated polio vaccine (IPV) or oral polio vaccine (OPV) being the most common options. To determine your vaccination status, you can review your immunization records, consult with your healthcare provider, or check for documentation such as a vaccination card or medical history. If you are unsure or unable to locate your records, a blood test can assess your immunity levels, and your healthcare provider can recommend appropriate steps, including catch-up vaccinations if necessary. Ensuring you are protected against polio not only safeguards your health but also contributes to global efforts to eradicate this preventable disease.
Explore related products






What You'll Learn
- Vaccine Types: Oral (OPV) vs. Inactivated (IPV) polio vaccines and their differences
- Vaccination Schedule: Recommended doses and timing for polio immunization in children
- Immunity Duration: How long polio vaccines provide protection against the virus
- Side Effects: Common and rare reactions to polio vaccination in individuals
- Verification Methods: Checking vaccination records or antibody tests to confirm polio immunity
![]()
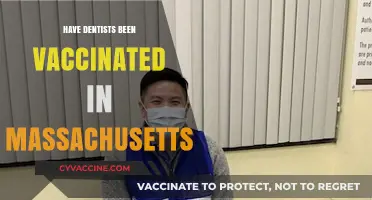
Vaccine Types: Oral (OPV) vs. Inactivated (IPV) polio vaccines and their differences
Polio vaccination relies on two primary tools: the Oral Polio Vaccine (OPV) and the Inactivated Polio Vaccine (IPV). Understanding their differences is crucial for informed decision-making, especially in regions where polio remains a threat or for travelers to endemic areas.
Mechanism & Administration: OPV, a live attenuated vaccine, contains weakened poliovirus strains that replicate in the gut, triggering immunity. Administered orally (drops or syrup), it’s ideal for mass campaigns due to ease of delivery, particularly in low-resource settings. IPV, in contrast, uses inactivated (killed) virus injected intramuscularly or subcutaneously, requiring trained healthcare personnel. While less logistically demanding than OPV for large-scale use, IPV’s injectable format ensures precise dosing.
Immunity Profile: OPV confers both humoral (bloodstream) and mucosal (intestinal) immunity, reducing viral shedding and transmission—a key advantage in outbreak control. IPV primarily induces humoral immunity, effectively preventing paralytic disease but offering limited protection against viral spread. Combining both vaccines (sequential OPV-IPV or IPV-OPV schedules) maximizes individual and community protection, a strategy increasingly adopted in polio eradication efforts.
Safety & Risks: OPV’s live virus carries a rare risk (1 in 2.7 million doses) of vaccine-associated paralytic polio (VAPP), where the weakened virus reverts to a virulent form. This risk, though minuscule, has led many high-income countries to transition exclusively to IPV. IPV, being inactivated, cannot cause polio but may require booster doses to maintain long-term immunity. For infants, the WHO recommends OPV at birth in high-risk areas, followed by IPV doses at 6, 10, and 14 weeks, balancing safety and efficacy.
Global Use & Accessibility: OPV remains the backbone of global eradication campaigns due to its low cost ($0.15–$0.20 per dose) and suitability for mass immunization. IPV, costing $10–$20 per dose, is prioritized in polio-free countries to eliminate VAPP risk. Travelers to endemic regions should verify their vaccination status; most adults require a single IPV booster if previously immunized, while children follow age-specific schedules (e.g., 2–3 doses before international travel).
Practical Considerations: If unsure of your vaccination history, consult immunization records or request a blood titer test for polio antibodies. In the absence of records, adults can safely receive an IPV dose without prior testing. For parents, adhere to the WHO’s 2020 recommendation: use OPV in outbreak zones and IPV in routine schedules where polio is eliminated. Always store OPV at 2–8°C to maintain potency, a critical factor in remote vaccination drives.
By grasping these distinctions, individuals and health systems can tailor polio prevention strategies effectively, accelerating progress toward global eradication.
Do Puppies Feel Bad After Vaccines? Understanding Post-Shot Reactions
You may want to see also
Explore related products






![]()
Vaccination Schedule: Recommended doses and timing for polio immunization in children
Polio immunization in children follows a precise schedule to ensure robust protection against this debilitating disease. The World Health Organization (WHO) and national health authorities recommend a series of doses administered at specific intervals to maximize immunity. Typically, the vaccination begins in infancy, with the first dose given at 6 weeks of age, followed by subsequent doses at 10 weeks and 14 weeks. This primary series is crucial for building a strong immune foundation. A fourth dose, often referred to as a booster, is administered between 12 and 23 months of age to reinforce immunity. In some regions, an additional booster may be given during the school years, usually between 4 and 6 years old, to ensure long-term protection.
The timing of these doses is not arbitrary; it aligns with the child’s developing immune system and the risk of exposure to the poliovirus. For instance, the early doses are scheduled to protect infants during their most vulnerable months, while the later boosters maintain immunity as they grow. It’s essential to adhere to this schedule, as delays can leave children susceptible to infection. Parents and caregivers should consult their healthcare provider to confirm the exact timing based on local guidelines, as variations may exist depending on regional polio prevalence and vaccine availability.
One practical tip for parents is to keep a detailed record of their child’s vaccinations, including dates and types of vaccines received. This documentation is invaluable for tracking adherence to the schedule and ensuring no doses are missed. Many countries offer immunization cards or digital records for this purpose. If a dose is missed, healthcare providers can advise on catch-up schedules to minimize gaps in protection. Consistency is key, as the full series of doses is required to achieve optimal immunity against polio.
Comparatively, the polio vaccination schedule is simpler than some other childhood immunization regimens, such as those for measles or hepatitis B, which may involve more doses or combination vaccines. However, its importance cannot be overstated. Polio remains a threat in parts of the world, and even in regions where it has been eradicated, maintaining high vaccination rates is critical to prevent re-emergence. The schedule’s design reflects a balance between maximizing immunity and minimizing the number of clinic visits for young children, making it both effective and practical for families.
In conclusion, the recommended polio immunization schedule for children is a carefully structured plan designed to provide lifelong protection against a once-devastating disease. By following the prescribed doses and timing—starting at 6 weeks, continuing through infancy, and concluding with boosters in early childhood—parents can ensure their children are shielded from polio. Adherence to this schedule not only safeguards individual health but also contributes to global efforts to eradicate the disease. Practical steps, such as maintaining vaccination records and consulting healthcare providers, further support this critical public health initiative.
No Side Effects After Vaccination: Should You Be Concerned?
You may want to see also
Explore related products






![]()
Immunity Duration: How long polio vaccines provide protection against the virus
The duration of immunity provided by polio vaccines is a critical factor in their effectiveness, offering long-term protection against a once-devastating disease. Both the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV) have been instrumental in reducing global polio cases by over 99% since 1988. While IPV, typically administered through injection, is now the primary vaccine used in most countries, OPV, given orally, remains essential in regions where polio is still endemic. Understanding how long these vaccines confer immunity is vital for maintaining herd immunity and eradicating the virus entirely.
Analyzing the data, IPV provides robust and long-lasting immunity, often conferring protection for decades after the initial series of doses. The standard schedule involves three to four doses, starting at 2 months of age, with a booster shot recommended between 4 and 6 years. Studies show that after completing this series, individuals retain protective antibody levels for at least 18–20 years, with some evidence suggesting lifelong immunity. However, the exact duration can vary based on factors like age at vaccination, overall health, and exposure to the virus. For instance, older adults vaccinated in childhood may still have sufficient immunity, but a booster dose is advised for those at higher risk, such as healthcare workers or travelers to polio-endemic areas.
In contrast, OPV, while highly effective in inducing mucosal immunity and stopping viral transmission, has a slightly different immunity profile. The live attenuated virus in OPV stimulates a stronger gut-level immune response, which is crucial in regions with poor sanitation. However, the duration of immunity from OPV can wane more quickly compared to IPV, particularly in areas with low circulation of the virus. This has led to the strategic use of OPV in outbreak response, often supplemented with IPV to ensure broader and more durable protection. It’s also worth noting that rare cases of vaccine-derived poliovirus (VDPV) can occur with OPV, emphasizing the need for careful monitoring and vaccination strategies.
Practical tips for individuals unsure about their polio vaccination status include checking childhood immunization records or consulting healthcare providers. If records are unavailable, a blood test can measure poliovirus antibody levels, though this is not routinely recommended. For those planning travel to high-risk areas, a single IPV booster dose is generally sufficient to reinforce immunity, regardless of how long it’s been since the last vaccination. Pregnant women, immunocompromised individuals, and those with specific medical conditions should consult their doctor before receiving any polio vaccine, as recommendations may vary.
In conclusion, the polio vaccines’ immunity duration is a testament to their design and effectiveness, with IPV offering decades-long protection and OPV playing a vital role in interrupting transmission. While the vaccines’ longevity is well-established, staying informed about personal vaccination status and adhering to booster recommendations ensures continued protection against this preventable disease. As global efforts near polio eradication, maintaining awareness and vaccination compliance remains key to sustaining this public health victory.
Hepatitis A Vaccine and Fetal DNA: Unraveling the Facts and Myths
You may want to see also
Explore related products






![]()
Side Effects: Common and rare reactions to polio vaccination in individuals
Polio vaccination, a cornerstone of global health, is generally safe and highly effective. However, like any medical intervention, it can cause side effects, ranging from mild and common to rare and severe. Understanding these reactions is crucial for informed decision-making and managing expectations. The two primary types of polio vaccines—the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV)—have distinct side effect profiles, reflecting their different mechanisms of action.
Common Reactions: What to Expect After Vaccination
For IPV, administered as an injection, the most frequent side effects are localized and mild. These include soreness, redness, or swelling at the injection site, typically lasting 1–2 days. Some individuals, particularly children, may experience low-grade fever, fatigue, or irritability. These symptoms are transient and can be managed with over-the-counter pain relievers like acetaminophen, following age-appropriate dosing guidelines (e.g., 10–15 mg/kg every 4–6 hours for children). OPV, given orally, is even less likely to cause noticeable side effects, though rare cases of mild abdominal discomfort or loose stools have been reported. Both vaccines are well-tolerated across age groups, from infants to adults, with reactions more common in younger recipients due to their developing immune systems.
Rare but Serious: Understanding Severe Adverse Events
While extremely uncommon, severe reactions to polio vaccines warrant attention. IPV, being an inactivated vaccine, cannot cause polio, but in rare instances (approximately 1 in a million doses), it may lead to allergic reactions such as anaphylaxis. Symptoms include difficulty breathing, swelling of the face or throat, and rapid heartbeat, requiring immediate medical intervention. OPV, though highly effective, carries a theoretical risk of vaccine-associated paralytic polio (VAPP) at a rate of about 1 case per 2–4 million doses. This risk is higher in immunocompromised individuals or those with specific genetic conditions. Such cases highlight the importance of avoiding OPV in populations with weakened immunity, opting instead for IPV.
Comparing IPV and OPV: Weighing Risks and Benefits
The choice between IPV and OPV often depends on regional polio prevalence and individual health status. IPV’s side effect profile is milder and more predictable, making it the preferred option in polio-free countries. OPV, despite its rare risks, remains invaluable in outbreak settings due to its ability to induce intestinal immunity and reduce viral transmission. For example, in endemic regions, OPV’s benefits in halting polio spread outweigh its minimal VAPP risk. Conversely, IPV is the safer choice for travelers to polio-affected areas, offering robust protection without the risk of vaccine-derived poliovirus circulation.
Practical Tips for Managing Side Effects
To minimize discomfort after polio vaccination, apply a cool, damp cloth to the injection site for IPV recipients. Encourage hydration and light activity to alleviate systemic symptoms like fever or fatigue. For OPV, ensure proper administration—typically two drops for children under 5—and avoid contaminating the vaccine with food or drink. Immunocompromised individuals should strictly avoid OPV and receive IPV under medical supervision. Always report severe or persistent symptoms to a healthcare provider, as timely intervention can prevent complications. By recognizing and addressing side effects, individuals can confidently participate in polio eradication efforts while safeguarding their health.
Should UAE Mandate COVID-19 Vaccination? Pros, Cons, and Public Health
You may want to see also
Explore related products






![]()
Verification Methods: Checking vaccination records or antibody tests to confirm polio immunity
Determining whether you’ve been vaccinated against polio requires a systematic approach, as immunity can be confirmed through two primary methods: reviewing vaccination records or undergoing antibody testing. Vaccination records, often stored by healthcare providers or public health departments, detail the type and dates of immunizations received. For polio, the inactivated poliovirus vaccine (IPV) is typically administered in a series of doses—usually at 2, 4, and 6–18 months of age, followed by a booster at 4–6 years. If you’re unsure about your vaccination status, start by contacting your pediatrician, family doctor, or local health department. Many countries also maintain immunization registries, which can be accessed with proper identification.
While vaccination records are the most straightforward method, they aren’t always available, especially for older adults or those who’ve relocated frequently. In such cases, antibody testing emerges as a reliable alternative. A polio antibody test, often performed via blood draw, measures the presence of protective antibodies against the poliovirus. This test is particularly useful for individuals born before the 1980s, when oral polio vaccine (OPV) was more commonly used, or for those traveling to regions where polio remains endemic. Results typically indicate whether you have sufficient immunity, though interpretation should always be done by a healthcare professional.
Comparing the two methods reveals distinct advantages and limitations. Vaccination records offer a clear timeline of immunization but rely on accurate documentation. Antibody testing, on the other hand, provides direct evidence of immunity but may not distinguish between vaccine-induced and natural exposure. For instance, if you received OPV as a child, your antibody levels might reflect both vaccination and potential low-level exposure to the virus. Cost and accessibility also differ—records are often free but require legwork, while antibody tests may incur fees and require a lab visit.
For practical implementation, begin by gathering any available medical records, including childhood immunization cards or school health forms. If records are incomplete, consult with a healthcare provider to discuss antibody testing. Keep in mind that false negatives can occur if the test is performed too soon after vaccination, so timing is crucial. Additionally, travelers to high-risk areas should ensure their immunity status is confirmed at least 4–6 weeks before departure, allowing time for potential booster doses if needed.
In conclusion, verifying polio immunity is a critical step for personal and public health, especially in an era of global travel and vaccine hesitancy. By leveraging vaccination records or antibody testing, individuals can take proactive measures to ensure protection against this once-devastating disease. Whether through meticulous documentation or laboratory analysis, the goal remains the same: to confirm immunity and safeguard against polio’s resurgence.
Understanding the Essential 8-in-1 Puppy Vaccine for Optimal Health
You may want to see also
Frequently asked questions
Check your vaccination records, contact your healthcare provider, or review your childhood immunization documents. Some countries also maintain national immunization registries.
The inactivated polio vaccine (IPV) and oral polio vaccine (OPV) are used. The number of doses varies by country, but typically, 3–4 doses are given in childhood, followed by boosters in some regions.
Consult your healthcare provider. They may recommend a blood test to check for immunity or advise getting a dose of IPV, especially if you’re at risk of exposure.
Yes, the polio vaccine (IPV) is safe for adults. It’s recommended for those who haven’t been vaccinated or are unsure of their immunity, especially before traveling to polio-endemic areas.
The polio vaccine is highly effective, but no vaccine provides 100% protection. However, vaccinated individuals are at significantly lower risk of contracting polio.