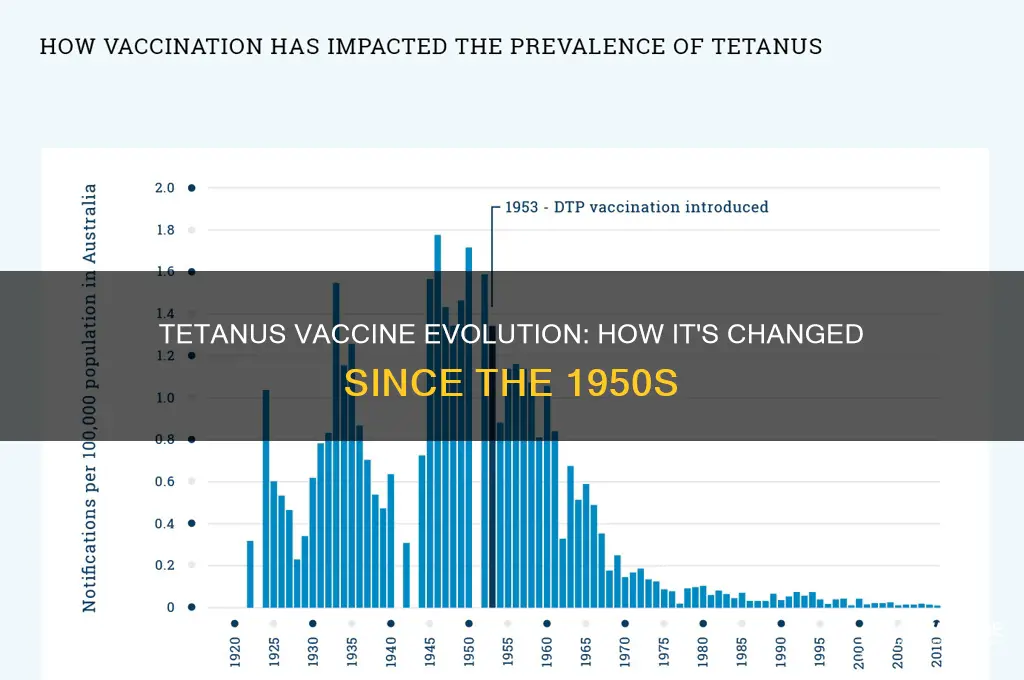
The tetanus vaccine has undergone significant advancements since its initial development in the 1920s, with notable changes occurring after 1950. In the mid-20th century, the tetanus toxoid vaccine, which was first introduced in the 1920s, became more widely available and was often combined with diphtheria toxoid to create the tetanus-diphtheria (Td) vaccine. Since then, the vaccine has been further refined, with the introduction of the tetanus-diphtheria-pertussis (DTP) vaccine in the 1940s and its subsequent replacement by the acellular pertussis-containing vaccine (DTaP) in the 1990s. Additionally, the development of the tetanus, diphtheria, and acellular pertussis (Tdap) vaccine in the early 2000s provided a reduced dose of pertussis components, making it suitable for adolescents and adults. These advancements have improved the safety, efficacy, and accessibility of tetanus vaccination, reducing the global burden of tetanus-related morbidity and mortality. Furthermore, ongoing research continues to explore new vaccine formulations, delivery methods, and immunization strategies to enhance protection against tetanus and other vaccine-preventable diseases.
| Characteristics | Values |
|---|---|
| Vaccine Composition | Modern tetanus vaccines use purified tetanus toxoid, unlike earlier formulations which may have contained less refined antigens. |
| Adjuvants | Aluminum salts are commonly used as adjuvants in modern tetanus vaccines to enhance immune response. |
| Preservatives | Some vaccines may contain preservatives like thiomersal, though preservative-free versions are also available. |
| Combination Vaccines | Tetanus vaccines are often combined with diphtheria (Td) and pertussis (DTaP/Tdap) in modern formulations. |
| Dosage and Schedule | Updated dosing schedules and booster recommendations based on improved understanding of immunity. |
| Safety Profile | Enhanced safety with reduced side effects compared to earlier versions. |
| Efficacy | Higher efficacy due to improved formulation and administration practices. |
| Storage Requirements | Modern vaccines often have more stable storage conditions, including some that are less temperature-sensitive. |
| Manufacturing Process | Advanced manufacturing techniques ensure higher purity and consistency. |
| Global Availability | Widespread availability and inclusion in national immunization programs globally. |
| Regulatory Approval | Modern vaccines undergo rigorous testing and approval by regulatory bodies like the FDA and WHO. |
| Public Perception | Increased public trust due to transparency and evidence-based communication about vaccine safety. |
Explore related products






What You'll Learn
- Vaccine Composition Evolution: Changes in tetanus toxoid formulation and adjuvants since 1950
- Manufacturing Advances: Improved production methods and quality control for tetanus vaccines
- Combination Vaccines: Integration of tetanus with diphtheria, pertussis, and other antigens
- Efficacy and Duration: Studies on vaccine effectiveness and immunity longevity over decades
- Safety Improvements: Reduced side effects and enhanced safety profiles since the 1950s
![]()
Vaccine Composition Evolution: Changes in tetanus toxoid formulation and adjuvants since 1950
The tetanus toxoid vaccine has undergone significant transformations since its early formulations in the 1950s, driven by advancements in immunology, manufacturing techniques, and safety standards. Initially, the vaccine consisted of crude tetanus toxoid preparations derived from tetanus toxin inactivated with formaldehyde. These early formulations were effective but often associated with local reactions due to impurities and the absence of modern adjuvants. Over time, purification methods improved, reducing side effects and enhancing immunogenicity. For instance, the shift from whole-cell to acellular toxoid preparations marked a pivotal change, allowing for more precise control over the antigen’s structure and potency.
One of the most notable changes in tetanus toxoid formulation has been the standardization of dosage and concentration. Early vaccines often contained variable amounts of toxoid, leading to inconsistent immune responses. Today, the typical adult dose is 0.5 mL of adsorbed tetanus toxoid, containing 5–10 LF (flocculating units) of toxoid. This standardization ensures predictable immunity while minimizing adverse reactions. Pediatric formulations, such as the DTaP vaccine (diphtheria, tetanus, and acellular pertussis), are tailored to younger age groups, with reduced antigen concentrations to suit their developing immune systems. For example, infants receive 0.5 mL doses at 2, 4, 6, and 15–18 months, followed by a booster at 4–6 years, ensuring sustained protection during critical developmental stages.
Adjuvants have played a crucial role in the evolution of tetanus vaccines, enhancing their efficacy and longevity. Early formulations relied on simple aluminum salts (alum) as adjuvants, which improved immune responses by promoting antigen presentation. However, modern vaccines have explored more sophisticated adjuvants, such as aluminum phosphate or hydroxide, which offer better stability and reduced reactogenicity. These advancements have been particularly beneficial for combination vaccines like Tdap (tetanus, diphtheria, and acellular pertussis), where adjuvants must balance the immunogenicity of multiple antigens. For instance, the use of aluminum adjuvants in Tdap ensures robust tetanus immunity while minimizing interference with pertussis antigens.
Practical considerations for administering tetanus vaccines have also evolved. Booster doses, once recommended every 5–10 years, are now tailored to individual risk factors, such as occupational exposure or wound management. For example, individuals with clean, minor wounds who have completed a primary series may not require a booster unless more than 10 years have passed since their last dose. In contrast, those with contaminated wounds and incomplete vaccination histories should receive a booster immediately, along with tetanus immune globulin if necessary. These guidelines reflect a more nuanced understanding of tetanus immunology and risk assessment, ensuring optimal protection without over-vaccination.
In summary, the evolution of tetanus toxoid formulation and adjuvants since 1950 highlights the interplay between scientific progress and public health needs. From crude preparations to standardized, adjuvant-enhanced vaccines, these changes have improved safety, efficacy, and accessibility. For healthcare providers and individuals alike, understanding these advancements is essential for informed decision-making, whether administering vaccines or seeking protection against tetanus. By staying abreast of these developments, we can ensure that tetanus remains a preventable disease in the modern era.
Bill Gates' Family Vaccination Choices: Fact-Checking the Rumors
You may want to see also
Explore related products






![]()
Manufacturing Advances: Improved production methods and quality control for tetanus vaccines
The tetanus vaccine has undergone significant transformations since its early formulations in the 1950s, with manufacturing advances playing a pivotal role in enhancing its safety, efficacy, and accessibility. One of the most notable improvements lies in the shift from crude, whole-cell preparations to highly purified toxoid-based vaccines. Early tetanus vaccines often contained impurities and residual chemicals from the production process, leading to higher rates of adverse reactions. Modern manufacturing techniques, such as recombinant DNA technology and chromatography, now ensure the isolation of only the essential tetanus toxoid component, minimizing contaminants and improving tolerability. This refinement has been particularly beneficial for pediatric populations, where a 0.5 mL dose of the purified vaccine is administered as part of the DTaP (Diphtheria, Tetanus, and Pertussis) series, starting at 2 months of age, with booster doses recommended every 10 years thereafter.
A critical aspect of these manufacturing advances is the implementation of stringent quality control measures. In the 1950s, batch testing was rudimentary, often relying on animal models to assess potency and safety. Today, manufacturers employ advanced analytical tools, such as mass spectrometry and enzyme-linked immunosorbent assays (ELISAs), to precisely quantify toxoid concentration and detect potential contaminants. These methods ensure that each vial meets international standards, such as those set by the World Health Organization (WHO), which mandates a minimum toxoid content of 5 LF (flocculating units) per dose. Additionally, automated production lines and sterile filtration systems have reduced the risk of microbial contamination, a common issue in earlier manufacturing processes.
The adoption of adjuvants and stabilizers has further revolutionized tetanus vaccine production. Aluminum salts, commonly used as adjuvants, enhance the immune response by promoting antigen presentation, allowing for lower toxoid doses without compromising efficacy. For instance, the Tdap vaccine (Tetanus, Diphtheria, and acellular Pertussis) contains 5-20 LF of tetanus toxoid, combined with aluminum phosphate or sulfate, to ensure a robust immune response in adolescents and adults. Stabilizers like lactose or sucrose are also added to maintain vaccine potency during storage, particularly in multi-dose vials, which are essential for mass immunization campaigns in resource-limited settings.
Another transformative development is the integration of continuous manufacturing processes, which have replaced traditional batch production methods. Continuous biomanufacturing allows for real-time monitoring and adjustment of production parameters, reducing variability and increasing yield. This approach has not only streamlined vaccine production but also lowered costs, making tetanus vaccines more affordable globally. For example, the price of a single dose of tetanus toxoid-containing vaccines has decreased from approximately $10 in the 1950s (adjusted for inflation) to less than $1 in many low-income countries today, thanks to these efficiencies.
Despite these advancements, challenges remain, particularly in ensuring consistent access to high-quality vaccines worldwide. Manufacturers must adhere to Good Manufacturing Practices (GMP) guidelines, which include rigorous documentation, personnel training, and facility maintenance. Practical tips for healthcare providers include storing vaccines between 2°C and 8°C, avoiding freeze-thaw cycles, and using single-dose vials whenever possible to prevent contamination. As manufacturing technologies continue to evolve, the tetanus vaccine stands as a testament to how innovation can drive improvements in public health, saving millions of lives annually from this once-devastating disease.
USPS COVID-19 Vaccine Mandate: What Employees Need to Know
You may want to see also
Explore related products






![]()
Combination Vaccines: Integration of tetanus with diphtheria, pertussis, and other antigens
The tetanus vaccine has evolved significantly since its early formulations in the 1950s, with one of the most notable advancements being the development of combination vaccines. These innovations integrate tetanus toxoid with antigens for diphtheria, pertussis, and other diseases, streamlining immunization schedules and improving public health outcomes. This approach not only simplifies vaccine administration but also enhances compliance by reducing the number of required injections.
Analytical Perspective:
Combination vaccines, such as DTaP (diphtheria, tetanus, and acellular pertussis) for children and Tdap for adolescents and adults, exemplify the integration of multiple antigens into a single formulation. For instance, the DTaP vaccine is administered in a series of 5 doses starting at 2 months of age, with boosters recommended at 4–6 years. This schedule ensures sustained immunity against all three diseases, addressing the resurgence of pertussis while maintaining protection against tetanus and diphtheria. The acellular pertussis component, introduced in the 1990s, replaced the whole-cell version, reducing side effects while maintaining efficacy.
Instructive Approach:
When administering combination vaccines, healthcare providers must adhere to specific dosage guidelines. For adults, the Tdap vaccine (e.g., Adacel or Boostrix) is recommended as a one-time booster, followed by Td (tetanus and diphtheria) boosters every 10 years. Pregnant individuals should receive Tdap during each pregnancy, ideally between 27 and 36 weeks, to confer passive immunity to the newborn. It’s crucial to verify prior vaccination history to avoid over-immunization, particularly with tetanus toxoid, which can cause adverse reactions if administered too frequently.
Comparative Insight:
Compared to standalone tetanus vaccines, combination vaccines offer practical advantages, particularly in resource-limited settings. For example, the pentavalent vaccine (DTaP-HepB-Hib) combines protection against diphtheria, tetanus, pertussis, hepatitis B, and *Haemophilus influenzae* type b, reducing the logistical burden of multiple injections. This approach has been instrumental in global immunization campaigns, improving coverage rates for all included antigens. However, combination vaccines may have slightly higher rates of local reactions, such as pain or swelling at the injection site, which should be communicated to recipients.
Persuasive Argument:
The integration of tetanus with other antigens in combination vaccines is a testament to the adaptability and progress of immunization science. By consolidating multiple vaccines into a single dose, this strategy not only saves time and resources but also addresses vaccine hesitancy by minimizing the number of clinic visits. For parents, this means fewer stressful appointments for their children, while public health systems benefit from streamlined inventory management and improved adherence to vaccination schedules. As vaccine technology continues to advance, further innovations in combination formulations are likely to emerge, reinforcing their role as a cornerstone of modern preventive medicine.
Do Vaccines Cause Peanut Allergies? Separating Fact from Fiction
You may want to see also
Explore related products






![]()
Efficacy and Duration: Studies on vaccine effectiveness and immunity longevity over decades
The tetanus vaccine has undergone significant advancements since its introduction in the 1920s, with modern formulations boasting higher efficacy and longer-lasting immunity. Early vaccines, including those used in the 1950s, were often whole-cell preparations that, while effective, sometimes caused adverse reactions like pain and swelling at the injection site. Today’s vaccines, such as the tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) formulation, use purified components to minimize side effects while maintaining robust protection. This evolution underscores the importance of studying how vaccine effectiveness and immunity longevity have changed over decades.
Analyzing long-term studies reveals that the tetanus vaccine provides near-complete protection against the disease, with efficacy rates consistently above 95% across age groups. For instance, a 2019 review in *Vaccine* found that individuals who received a primary series of tetanus vaccinations retained protective antibody levels for at least 30 years. However, immunity wanes over time, necessitating booster doses. Adults are advised to receive a Tdap booster every 10 years, while individuals with deep or dirty wounds should get a booster if their last dose was more than 5 years prior. These recommendations are based on studies showing that antibody titers decline significantly after a decade, leaving individuals vulnerable to infection without reinforcement.
Comparatively, the duration of immunity from the 1950s vaccines was shorter due to less refined formulations and lower antigen concentrations. Modern vaccines, with standardized dosages of 5 Lf (limit of flocculation) of tetanus toxoid, ensure consistent immune responses. For example, a study published in *Clinical Infectious Diseases* demonstrated that individuals vaccinated with contemporary formulations maintained protective antibody levels for over 20 years, compared to 10–15 years with older vaccines. This improvement highlights the role of technological advancements in enhancing vaccine longevity.
Practical tips for maintaining tetanus immunity include keeping a vaccination record to track booster schedules and consulting healthcare providers after injuries, especially if the wound is contaminated. For travelers to regions with limited medical resources, ensuring up-to-date tetanus vaccination is critical, as tetanus remains endemic in many low-income countries. Parents should also ensure children complete the recommended DTaP series (diphtheria, tetanus, and acellular pertussis) at 2, 4, 6, and 15–18 months, followed by a booster at 4–6 years, to establish a strong foundation of immunity.
In conclusion, studies on vaccine effectiveness and immunity longevity demonstrate that modern tetanus vaccines offer superior and prolonged protection compared to their 1950s counterparts. While the core principle of inducing antitoxin antibodies remains unchanged, refinements in formulation and dosing have extended immunity duration and reduced side effects. Adhering to current vaccination guidelines ensures sustained protection against this potentially fatal disease, making it a cornerstone of public health strategies worldwide.
Understanding Rotavirus Vaccine Age Limits: Why 15 Months is Maximum
You may want to see also
![]()
Safety Improvements: Reduced side effects and enhanced safety profiles since the 1950s
The tetanus vaccine has undergone significant transformations since the 1950s, with safety improvements being a cornerstone of its evolution. Early formulations, such as the tetanus toxoid (TT) introduced in the 1920s and widely used mid-century, were effective in preventing tetanus but often caused notable side effects. These included pain, redness, and swelling at the injection site, as well as systemic reactions like fever and fatigue. For instance, the original TT vaccine had a higher incidence of adverse reactions, particularly in individuals receiving booster doses, due to the presence of higher antigen concentrations and less purified formulations.
Analyzing the shift from the 1950s to the present, one of the most critical advancements has been the refinement of vaccine manufacturing processes. Modern tetanus vaccines, such as the tetanus, diphtheria, and acellular pertussis (Tdap) combination vaccine, use highly purified tetanus toxoid. This purification reduces the presence of extraneous proteins and impurities that previously contributed to side effects. For example, the Tdap vaccine, recommended for adolescents and adults, contains a reduced dose of tetanus toxoid compared to earlier formulations, minimizing local and systemic reactions while maintaining robust immunity. This precision in dosing and purification exemplifies how safety profiles have been enhanced over time.
Instructively, the transition to combination vaccines like DTaP (diphtheria, tetanus, and acellular pertussis) for children and Tdap for older age groups has further improved safety. The acellular pertussis component in these vaccines, introduced in the 1990s, replaced the whole-cell pertussis vaccine, which was associated with higher rates of fever, irritability, and rare neurological events. By integrating tetanus vaccination into these safer combination products, public health officials have streamlined immunization schedules while reducing the risk of adverse effects. Parents and caregivers should note that the CDC recommends DTaP doses at 2, 4, 6, and 15-18 months, followed by a Tdap booster at 11-12 years, ensuring continuous protection with minimal side effects.
Persuasively, the data underscores the success of these safety improvements. Studies comparing the original TT vaccine to modern Tdap formulations show a dramatic reduction in severe adverse events, such as anaphylaxis, which is now estimated to occur in fewer than 1 in a million doses. Additionally, the incidence of moderate reactions, like extensive limb swelling, has decreased from 1-2% in the 1950s to less than 0.1% today. These statistics highlight the importance of ongoing vaccine research and development, demonstrating that safety enhancements are not just theoretical but have tangible, real-world benefits for recipients.
Comparatively, the evolution of the tetanus vaccine mirrors broader trends in vaccinology, where safety and efficacy are continually balanced through innovation. Unlike the 1950s, when vaccines were often crude by today’s standards, modern formulations prioritize both immunogenicity and tolerability. For instance, the use of adjuvants like aluminum salts in tetanus vaccines has been optimized to enhance immune response without increasing side effects. This contrasts with earlier formulations, where higher antigen doses were sometimes used to compensate for lower purity, leading to more frequent reactions. The takeaway is clear: safety improvements in the tetanus vaccine are a testament to the power of scientific progress in protecting public health.
Understanding the Full Form of SIC R Vaccination: A Comprehensive Guide
You may want to see also
Frequently asked questions
Yes, the tetanus vaccine has evolved since 1950. Early vaccines used whole-cell pertussis components combined with tetanus and diphtheria toxoids (DTP), but modern formulations typically use acellular pertussis components (DTaP or Tdap) for improved safety and reduced side effects.
No, the tetanus vaccine today is not the same as in 1950. While the core tetanus toxoid remains effective, the vaccine is now often combined with acellular pertussis and diphtheria components, and manufacturing processes have been refined for purity and consistency.
Yes, the tetanus vaccine's effectiveness has improved due to advancements in production techniques, better purification methods, and the inclusion of adjuvants to enhance immune response. Modern vaccines provide robust and long-lasting protection.
Yes, side effects are generally milder today. Early vaccines, especially those with whole-cell pertussis, caused more frequent and severe reactions. Modern acellular vaccines (DTaP/Tdap) have significantly reduced side effects while maintaining efficacy.
Yes, the vaccination schedule has been updated. In 1950, tetanus vaccination was often given as a standalone shot or in combination with diphtheria. Today, it is typically administered as part of a series (DTaP for children, Tdap for adolescents/adults) with booster recommendations every 10 years or after injuries.