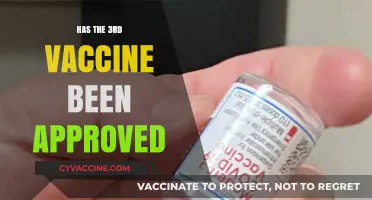
The question of whether anyone has died from COVID-19 vaccines has been a topic of significant public concern and misinformation. While rare, serious adverse events, including deaths, have been reported following vaccination, extensive research and data from health authorities such as the CDC, WHO, and EMA consistently show that these cases are extremely uncommon and often unrelated to the vaccine itself. Studies indicate that the benefits of vaccination in preventing severe illness, hospitalization, and death from COVID-19 far outweigh the minimal risks. Additionally, investigations into reported deaths have frequently identified underlying health conditions or other factors as the primary cause. It is crucial to rely on credible, evidence-based sources to understand the safety profile of vaccines and avoid spreading unfounded claims.
| Characteristics | Values |
|---|---|
| Reported Deaths Post-Vaccination | Rare cases of deaths have been reported following COVID-19 vaccination, but causality is not always established. |
| Causal Link Established | In some cases, a direct causal link between the vaccine and death has been confirmed (e.g., rare instances of thrombosis with thrombocytopenia syndrome (TTS) after adenovirus vector vaccines). |
| Frequency of Fatal Outcomes | Extremely rare; estimated at approximately 1-2 deaths per million doses administered, depending on the vaccine type and population. |
| Vaccine Types Involved | Adenovirus vector vaccines (e.g., AstraZeneca, Johnson & Johnson) have been associated with rare fatal cases of TTS. mRNA vaccines (e.g., Pfizer, Moderna) have rare reports of myocarditis-related deaths. |
| Demographics at Higher Risk | Younger individuals (especially males under 50) are at slightly higher risk for rare adverse events like TTS or myocarditis. |
| Global Monitoring Systems | Systems like VAERS (U.S.), EudraVigilance (EU), and WHO's VigiBase monitor and investigate reported deaths post-vaccination. |
| Comparative Risk | Risk of death from COVID-19 infection is significantly higher than the risk of death from vaccination, especially in vulnerable populations. |
| Public Health Stance | Health organizations (WHO, CDC, EMA) emphasize that the benefits of vaccination far outweigh the rare risks of severe adverse events, including death. |
| Latest Data (as of 2023) | Ongoing surveillance indicates that fatal outcomes remain exceptionally rare, with no significant increase in reported cases since initial vaccine rollouts. |
Explore related products

$11.93 $21.99





What You'll Learn
![]()
Reported Deaths Post-Vaccination
Vaccine safety monitoring systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the United States and the Yellow Card scheme in the UK, have recorded rare instances of deaths following vaccination. These reports are crucial for identifying potential patterns or risks, but they do not inherently prove causation. For example, as of October 2023, VAERS received over 15,000 reports of death among individuals who received COVID-19 vaccines, out of more than 600 million doses administered in the U.S. alone. However, the majority of these cases involved elderly individuals or those with pre-existing conditions, making it essential to differentiate between correlation and causation.
Analyzing these reports requires a nuanced approach. Health authorities often conduct thorough investigations, including autopsies and medical record reviews, to determine whether a death was directly linked to the vaccine. For instance, the rare cases of thrombosis with thrombocytopenia syndrome (TTS) following the Johnson & Johnson COVID-19 vaccine led to specific warnings for individuals under 50. Similarly, anaphylaxis, a severe allergic reaction, has been documented in approximately 2 to 5 cases per million doses of mRNA vaccines, with prompt medical intervention being critical to prevent fatalities. These examples highlight the importance of understanding individual risk factors and following post-vaccination guidelines.
From a comparative perspective, the risk of death from vaccine-preventable diseases far outweighs the risk of death from the vaccines themselves. For example, COVID-19 has caused over 6 million deaths globally, whereas vaccine-related fatalities remain extremely rare. Influenza vaccines, administered annually to millions, have an even lower fatality rate, with VAERS reporting fewer than 100 deaths per year, many of which are unrelated to the vaccine. This comparison underscores the life-saving benefits of vaccination and the rigorous safety standards in place to minimize risks.
Practical tips for individuals post-vaccination include monitoring for severe symptoms such as difficulty breathing, swelling of the face or throat, or persistent dizziness, which warrant immediate medical attention. Staying hydrated and resting for 24–48 hours after vaccination can also help manage common side effects like fever or fatigue. For those with a history of severe allergies, consulting a healthcare provider before vaccination is advisable. Finally, reporting any adverse events to national monitoring systems contributes to ongoing safety evaluations, ensuring vaccines remain as safe as possible for everyone.
Yellow Fever Vaccine Requirement for Panama Entry: What You Need to Know
You may want to see also
Explore related products






![]()
Vaccine Side Effects Analysis
Vaccine safety is a critical concern, and while rare, severe side effects, including fatalities, have been reported. However, it’s essential to contextualize these events within the vast scale of global vaccination campaigns. For instance, as of 2023, over 13 billion COVID-19 vaccine doses have been administered worldwide. Adverse events leading to death are exceedingly rare, with rates estimated at approximately 1-2 cases per million doses. These incidents are meticulously investigated by health authorities to determine causality, as many occur due to underlying health conditions rather than the vaccine itself. Understanding this data is crucial for distinguishing between correlation and causation in vaccine-related fatalities.
Analyzing specific vaccines reveals varying side effect profiles. For example, the mRNA COVID-19 vaccines (Pfizer-BioNTech and Moderna) have been associated with rare cases of myocarditis, particularly in young males aged 12-29 after the second dose. Symptoms typically appear within a week of vaccination and include chest pain, shortness of breath, and fatigue. While most cases resolve with rest and treatment, severe outcomes, including death, have been documented in fewer than 1 in 500,000 vaccinated individuals. In contrast, the adenovirus vector vaccines (AstraZeneca and Johnson & Johnson) have been linked to rare blood clotting disorders, such as thrombosis with thrombocytopenia syndrome (TTS), with a fatality rate of approximately 20% among those affected, though incidence remains below 1 in 100,000 doses.
To minimize risks, healthcare providers follow specific protocols. For mRNA vaccines, the CDC recommends spacing doses by 8 weeks for individuals under 30 to reduce myocarditis risk. For those with a history of severe allergies, a 30-minute observation period post-vaccination is standard. Pregnant individuals and those with compromised immune systems are advised to consult their healthcare provider before vaccination, as side effects may vary. Practical tips include staying hydrated, monitoring for unusual symptoms, and reporting adverse reactions to national surveillance systems like VAERS (Vaccine Adverse Event Reporting System) in the U.S.
Comparatively, vaccine side effects pale in severity and frequency when weighed against the risks of the diseases they prevent. For instance, COVID-19 has a mortality rate of approximately 1% globally, with higher rates among the elderly and immunocompromised. Influenza vaccines, administered annually to millions, have a fatality rate associated with severe side effects of less than 1 in a million doses, while influenza itself causes tens of thousands of deaths yearly in the U.S. alone. This underscores the principle that the benefits of vaccination overwhelmingly outweigh the risks, even accounting for rare adverse events.
In conclusion, while no medical intervention is entirely risk-free, the incidence of fatal vaccine side effects is minuscule compared to the scale of administration and the dangers of preventable diseases. Public health strategies must continue to emphasize transparency, surveillance, and education to build trust and ensure informed decision-making. By focusing on evidence-based analysis and practical risk mitigation, societies can maximize the life-saving potential of vaccines while minimizing harm.
Frontline Workers and COVID-19 Vaccination Rates: A Comprehensive Analysis
You may want to see also
Explore related products






![]()
Global Adverse Event Data
Vaccine safety monitoring relies heavily on global adverse event data, a critical tool for identifying rare but serious side effects, including deaths. Systems like the Vaccine Adverse Event Reporting System (VAERS) in the U.S., the Yellow Card scheme in the UK, and the EudraVigilance in the EU collect reports of health issues following vaccination. These databases are passive, meaning they rely on voluntary submissions from healthcare providers and the public. While they don’t prove causation, they serve as early warning signals, prompting further investigation. For instance, the rare link between the AstraZeneca COVID-19 vaccine and thrombosis with thrombocytopenia syndrome (TTS) was first flagged through such systems, leading to age-based restrictions in several countries.
Analyzing global adverse event data requires careful interpretation. Reports of deaths following vaccination are not automatically attributed to the vaccine itself. Confounding factors like pre-existing conditions, age, and concurrent illnesses must be considered. For example, during the COVID-19 vaccine rollout, many recipients were elderly or had comorbidities, populations already at higher risk of mortality. A 2021 study in *The Lancet* found that out of 20 million vaccine doses administered, 74 deaths were reported within 14 days of vaccination. However, upon review, none were conclusively linked to the vaccine, highlighting the importance of rigorous analysis.
To effectively use global adverse event data, stakeholders must follow structured steps. First, standardize reporting formats across countries to ensure comparability. Second, employ advanced analytics, such as disproportionality analysis, to identify signals of potential safety concerns. Third, cross-reference data with population-level mortality rates to contextualize findings. For instance, if 1 in 100,000 vaccinated individuals dies within a week, compare this to the baseline death rate in the same demographic. Finally, communicate findings transparently to maintain public trust. Misinterpretation of raw data can fuel misinformation, as seen in unfounded claims linking COVID-19 vaccines to sudden deaths.
Despite its utility, global adverse event data has limitations. Underreporting is a persistent issue, with estimates suggesting only 1-10% of adverse events are reported. Additionally, the absence of a control group makes it difficult to establish causality. To address these gaps, active surveillance systems like the CDC’s V-safe have been introduced, collecting real-time data from vaccine recipients. Combining passive and active monitoring provides a more comprehensive safety profile. For example, V-safe data reassured the public about the safety of COVID-19 vaccines in pregnant individuals, a group often excluded from clinical trials.
In conclusion, global adverse event data is an indispensable tool for vaccine safety, but its interpretation requires nuance. By standardizing reporting, employing advanced analytics, and integrating active surveillance, we can better distinguish between coincidental events and true vaccine-related risks. This approach not only safeguards public health but also strengthens confidence in vaccination programs. As vaccines continue to evolve, so too must our methods for monitoring their safety, ensuring that every dose administered is as safe as possible.
Soothing Sore Arms: Post-Meningitis Vaccine Care Tips and Remedies
You may want to see also
Explore related products

$20.41 $29.99





![]()
Causality vs. Correlation Studies
A search for 'has anyone died from the vaccine' yields a mix of anecdotal reports, news articles, and scientific studies. While some sources claim deaths have occurred post-vaccination, establishing a direct causal link between the vaccine and these fatalities is complex. This is where the distinction between causality and correlation becomes critical. Understanding this difference is essential for interpreting data accurately and making informed decisions about vaccine safety.
Analyzing the Data: A Case Study Approach
Consider a hypothetical scenario: a 75-year-old individual with pre-existing cardiovascular disease receives a COVID-19 vaccine and dies two days later from a heart attack. This event, if reported, might be correlated with the vaccination. However, correlation does not imply causation. To establish causality, researchers would need to conduct a thorough investigation, considering factors such as the individual's medical history, the temporal relationship between vaccination and death, and the biological plausibility of the vaccine causing a heart attack. In this case, studies have shown that the risk of severe COVID-19 outcomes, including cardiovascular complications, is significantly higher than any potential vaccine-related risks. For instance, a study published in *The Lancet* found that the risk of myocardial infarction (heart attack) within 28 days of a COVID-19 diagnosis was 1.6 times higher than in the general population, whereas the same risk post-vaccination was not statistically significant.
Instructive Steps to Differentiate Causality and Correlation
- Identify Temporal Relationship: Determine if the event (e.g., death) occurred after the vaccination. For example, adverse events monitored by the CDC’s Vaccine Adverse Event Reporting System (VAERS) are tracked within specific timeframes, such as 0-7 days for anaphylaxis or 4-42 days for thrombosis with thrombocytopenia syndrome (TTS) after the Johnson & Johnson vaccine.
- Assess Biological Plausibility: Evaluate whether the vaccine’s mechanism of action could reasonably cause the observed outcome. For instance, mRNA vaccines like Pfizer and Moderna do not interact with DNA or alter human genes, debunking claims of long-term genetic modifications.
- Control for Confounding Variables: Consider pre-existing conditions, age, and other factors. For example, individuals over 65 are both more likely to receive vaccines and more susceptible to age-related health issues, making correlation studies prone to misinterpretation.
- Utilize Comparative Data: Compare vaccinated and unvaccinated populations. A study in *JAMA* found that the rate of deaths within 30 days of vaccination was 0.004% among 20 million recipients, comparable to background mortality rates, suggesting no causal link.
Persuasive Argument for Rigorous Methodology
Critics often point to isolated cases of post-vaccination deaths as evidence of causality. However, without controlled studies, these claims remain speculative. For example, the rare occurrence of TTS after the Johnson & Johnson vaccine (approximately 7 per 1 million doses in women aged 18-49) was identified through rigorous pharmacovigilance, not anecdotal reports. This highlights the importance of large-scale, peer-reviewed studies over individual cases. Regulatory bodies like the FDA and WHO employ causality assessment frameworks, such as the Bradford Hill criteria, to systematically evaluate whether a relationship is causal or merely correlational.
Comparative Analysis: Vaccine Safety vs. Disease Risks
While correlation studies may raise alarms, causality studies provide context. For instance, the risk of severe COVID-19 in unvaccinated individuals aged 65 and older is 50 times higher than in younger populations. In contrast, the risk of a severe adverse event from the vaccine in this age group is approximately 1 in 100,000 doses. This comparison underscores the importance of weighing relative risks. Practical tips for healthcare providers include explaining these statistics to patients and emphasizing that temporal associations (e.g., dying days after vaccination) do not negate the overwhelming evidence of vaccine safety.
Descriptive Takeaway: Navigating Misinformation
Misinterpretation of causality and correlation fuels vaccine hesitancy. For example, a widely shared claim that "thousands have died from the vaccine" often stems from VAERS data, which includes unverified reports. Understanding that VAERS is a passive surveillance system, not a causality database, is crucial. To combat misinformation, focus on peer-reviewed studies, such as those in *The New England Journal of Medicine*, which consistently demonstrate vaccine safety across diverse populations. By prioritizing causality over correlation, individuals can make evidence-based decisions, ensuring public health remains the priority.
Understanding AAHS Control in Gardasil Vaccine Research: Key Insights
You may want to see also
Explore related products






![]()
Rare Severe Reactions Overview
Vaccine safety monitoring systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the United States and the Yellow Card scheme in the UK, have identified rare but severe reactions associated with COVID-19 vaccines. These reactions, while uncommon, are critical to understand for both healthcare providers and recipients. For instance, anaphylaxis—a severe allergic reaction—has been reported in approximately 2 to 5 people per million doses administered, primarily within 15–30 minutes of vaccination. Immediate recognition and treatment with epinephrine are essential, as delays can be life-threatening.
Another rare but severe reaction is thrombosis with thrombocytopenia syndrome (TTS), linked primarily to adenovirus vector vaccines like Johnson & Johnson’s Janssen. TTS occurs in about 7 per 1 million vaccinated individuals, predominantly in women aged 18–49. Symptoms include severe headaches, abdominal pain, and easy bruising, typically appearing 4–28 days post-vaccination. Treatment involves avoiding heparin and administering non-heparin anticoagulants and intravenous immunoglobulin. Recognizing these symptoms early is crucial, as misdiagnosis can lead to fatal outcomes.
Myocarditis and pericarditis, inflammation of the heart muscle and lining, respectively, have been associated with mRNA vaccines (Pfizer-BioNTech and Moderna), particularly in males aged 12–29 after the second dose. Incidence rates range from 10 to 69 cases per million doses, depending on age and sex. Symptoms include chest pain, shortness of breath, and palpitations, usually appearing within a week of vaccination. Most cases resolve with rest and anti-inflammatory medications, but monitoring for complications is vital.
Practical tips for minimizing risks include screening for contraindications (e.g., severe allergies to vaccine components) before administration and ensuring access to emergency medical care at vaccination sites. Recipients should be educated about potential symptoms and advised to seek immediate care if they occur. While these severe reactions are rare, their prompt identification and management are key to maintaining public trust in vaccine safety.
Ice or Heat: Which Soothes Vaccination Site Discomfort Best?
You may want to see also
Frequently asked questions
While extremely rare, there have been reports of deaths following COVID-19 vaccination. However, investigations by health authorities like the CDC and WHO have found no direct causal link between the vaccines and these deaths. Most reported cases involved individuals with underlying health conditions or other contributing factors.
No, COVID-19 vaccine-related deaths are exceptionally rare. The risk of severe complications or death from the vaccine is significantly lower than the risk of severe illness or death from COVID-19 itself.
The exact number varies by region and reporting system, but the rate is extremely low compared to the billions of doses administered globally. For example, in the U.S., the Vaccine Adverse Event Reporting System (VAERS) has received a small number of reports, but causality has not been established in most cases.
No, avoiding the vaccine is riskier than getting vaccinated. The COVID-19 vaccines have been proven to reduce the risk of severe illness, hospitalization, and death from the virus. The benefits of vaccination far outweigh the extremely rare risks associated with the vaccine.