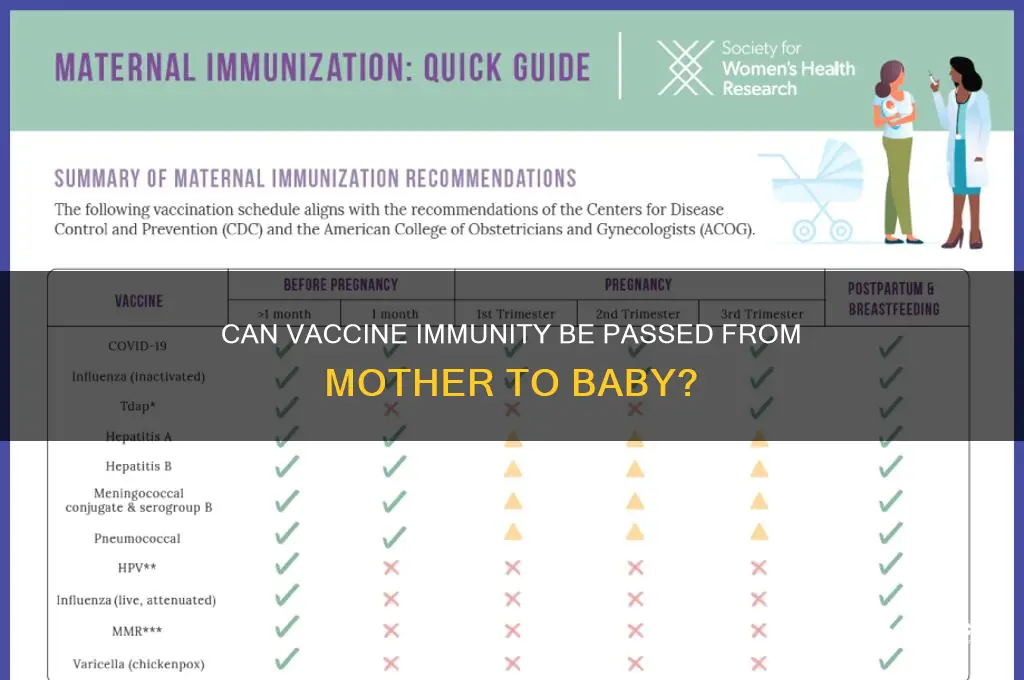
The question of whether vaccine-induced immunity can be passed from a mother to her baby is a critical aspect of maternal and infant health. During pregnancy, certain vaccines, such as the flu and Tdap (tetanus, diphtheria, and pertussis), are recommended to protect both the mother and the newborn. When a mother receives these vaccines, her body produces antibodies that can cross the placenta, providing the baby with passive immunity during the first few months of life. This transfer of antibodies is particularly important because newborns have underdeveloped immune systems and are highly vulnerable to infections. Additionally, breastfeeding further enhances this protection, as antibodies are also present in breast milk. Understanding this mechanism highlights the significance of maternal vaccination in safeguarding infants until they are old enough to receive their own vaccines.
| Characteristics | Values |
|---|---|
| Mechanism of Transfer | Maternal antibodies are transferred to the baby via the placenta during pregnancy (passive immunity). |
| Duration of Protection | Protection lasts for a few months after birth, typically 3-6 months, depending on the vaccine. |
| Vaccines Providing Immunity | Tdap (Tetanus, Diphtheria, Pertussis), Influenza, COVID-19, and others administered during pregnancy. |
| Effectiveness | Provides partial to moderate protection against specific diseases in newborns. |
| Breastfeeding Contribution | Breast milk contains antibodies, offering additional short-term immunity. |
| Limitations | Does not replace the need for childhood vaccinations; protection is temporary. |
| Safety | Vaccination during pregnancy is safe and recommended by health authorities (e.g., CDC, WHO). |
| Disease Prevention | Reduces the risk of severe illness in infants from diseases like pertussis, flu, and COVID-19. |
| Timing of Vaccination | Optimal transfer occurs when vaccines are administered during the recommended gestational period (e.g., Tdap in 27-36 weeks). |
| Research Support | Extensive studies confirm the safety and efficacy of maternal vaccination for infant protection. |
Explore related products




What You'll Learn
![]()
Placental Antibody Transfer
Vaccines administered during pregnancy can confer passive immunity to the newborn through placental antibody transfer, a critical process that occurs primarily in the third trimester. This mechanism allows maternal IgG antibodies to cross the placenta, providing the infant with temporary protection against specific pathogens until their own immune system matures. For instance, the Tdap vaccine (tetanus, diphtheria, and acellular pertussis) is recommended between 27 and 36 weeks of gestation, ensuring optimal antibody levels in the baby at birth. This targeted timing maximizes the transfer of pertussis antibodies, reducing the risk of whooping cough in the vulnerable early months of life.
The efficiency of placental antibody transfer varies depending on the vaccine type, maternal immune response, and gestational age at vaccination. Studies show that vaccines like influenza and COVID-19 mRNA vaccines also facilitate robust antibody transfer, offering newborns protection during their first six months. For example, maternal COVID-19 vaccination has been linked to a 61% reduction in infant hospitalizations due to SARS-CoV-2. However, not all vaccines are equally effective in this regard; live-attenuated vaccines, such as MMR, are generally avoided during pregnancy due to theoretical risks, though passive immunity from pre-pregnancy vaccination may still benefit the baby.
To optimize placental antibody transfer, healthcare providers emphasize timely vaccination during pregnancy. The CDC recommends the flu vaccine at any time during pregnancy, as seasonal outbreaks can overlap with any trimester. For Tdap, adherence to the 27–36 week window is crucial, as earlier vaccination may result in lower antibody levels at birth. Pregnant individuals should consult their healthcare provider to tailor vaccination schedules to their specific needs, considering factors like pre-existing immunity and local disease prevalence.
While placental antibody transfer is a natural and effective process, it is not a substitute for childhood immunization. The protection conferred is temporary, typically lasting 3–6 months, after which the infant becomes susceptible to infections. Thus, adhering to the recommended childhood vaccination schedule is essential to ensure long-term immunity. Parents should also be aware that breastfeeding can further enhance passive immunity, as IgA antibodies in breast milk provide mucosal protection against pathogens like rotavirus and respiratory syncytial virus (RSV).
In summary, placental antibody transfer is a vital bridge between maternal and neonatal immunity, offering newborns immediate protection against specific diseases. By following evidence-based vaccination guidelines during pregnancy, parents can significantly reduce the risk of severe illness in their infants. This process underscores the interconnectedness of maternal and child health, highlighting the importance of proactive immunization strategies for both populations.
Mastering Shingrix Administration: Correct Technique for Optimal Vaccine Efficacy
You may want to see also
Explore related products






![]()
Breast Milk Immune Benefits
Breast milk is a dynamic, living fluid that transfers not only essential nutrients but also a sophisticated immune system from mother to baby. Unlike formula, it contains antibodies, immune cells, and antimicrobial proteins that actively protect the infant against pathogens. For instance, secretory IgA (sIgA) antibodies in breast milk coat the baby’s gut and respiratory tract, preventing harmful bacteria and viruses from attaching to mucosal surfaces. This passive immunity is particularly critical during the first six months of life, when a baby’s own immune system is still maturing. Studies show that breastfed infants have lower rates of respiratory infections, gastrointestinal illnesses, and ear infections compared to formula-fed infants, demonstrating the tangible immune benefits of breast milk.
To maximize these immune benefits, timing and consistency matter. Colostrum, the first milk produced after birth, is especially rich in antibodies and immune factors, making early initiation of breastfeeding (within the first hour of life) crucial. The World Health Organization (WHO) recommends exclusive breastfeeding for the first six months, followed by continued breastfeeding alongside complementary foods up to two years or beyond. Even partial breastfeeding offers some immune protection, though the benefits are dose-dependent. For mothers who cannot breastfeed exclusively, pumping and providing expressed milk can still transfer valuable immune components, though fresh milk is preferable as freezing may reduce the activity of certain immune cells.
One of the most fascinating aspects of breast milk immunity is its adaptability. A mother’s body responds to pathogens in her environment by producing specific antibodies that are then passed to her baby through milk. For example, if a mother is exposed to a cold virus, her immune system generates antibodies against that virus, which are then transferred to her baby, offering targeted protection. This dynamic process means breast milk is not just a static source of immunity but a personalized defense system tailored to the baby’s immediate needs. This adaptability is particularly beneficial in regions with high infectious disease prevalence, where it can significantly reduce infant morbidity and mortality.
Practical tips for optimizing breast milk’s immune benefits include maintaining a balanced diet rich in fruits, vegetables, and whole grains, as maternal nutrition influences the quality of milk. Staying hydrated and managing stress are also important, as both factors can affect milk production. For mothers who receive vaccinations, such as the flu or Tdap vaccine, breastfeeding can transfer vaccine-induced antibodies to the baby, providing additional protection. However, it’s essential to consult healthcare providers for personalized advice, especially for mothers with specific health conditions or concerns. By understanding and leveraging the immune power of breast milk, parents can give their babies a strong foundation for lifelong health.
Vaccine vs. Virus: Weighing Risks and Realities of Immunization
You may want to see also
Explore related products





![]()
Vaccine Timing in Pregnancy
Pregnancy reshapes a woman’s immune system, making her more susceptible to certain infections while also protecting the fetus. Vaccines during this period not only shield the mother but can confer passive immunity to the baby through the placenta and breast milk. However, the timing of vaccination matters. For instance, the Tdap vaccine (tetanus, diphtheria, and pertussis) is recommended between 27 and 36 weeks of gestation to maximize antibody transfer to the fetus, offering the newborn critical protection during the first two months of life, when they are too young to be vaccinated themselves.
The flu vaccine is another example where timing is crucial. Pregnant women are advised to get the inactivated influenza vaccine (IIV) during any trimester, as it reduces the risk of flu-related complications for both mother and baby. Studies show that maternal vaccination can provide the infant with antibodies that persist for up to six months after birth, significantly lowering the risk of hospitalization due to flu. However, the vaccine’s efficacy in antibody transfer peaks when administered in the second or third trimester, making this the optimal window for most women.
Not all vaccines are recommended during pregnancy. Live-attenuated vaccines, such as the MMR (measles, mumps, rubella) vaccine, are generally avoided due to theoretical risks to the fetus, though no evidence of harm has been documented. Instead, these vaccines should be given at least four weeks before conception or postponed until after delivery. This distinction highlights the importance of pre-pregnancy counseling and planning to ensure immunity is established before pregnancy or safely managed afterward.
Practical considerations also play a role in vaccine timing. For example, if a woman receives the Tdap vaccine too early in pregnancy, antibody levels may wane before birth, reducing protection for the baby. Conversely, delaying the flu vaccine until late in the third trimester might leave the mother vulnerable during earlier stages of pregnancy, when complications from the flu can be severe. Healthcare providers must balance these factors, often tailoring recommendations to individual risk profiles and seasonal considerations, such as flu activity peaks.
Ultimately, vaccine timing in pregnancy is a delicate balance of maximizing maternal and fetal protection while minimizing risks. Clear communication between healthcare providers and expectant mothers is essential, ensuring that vaccines are administered at the right time to optimize immunity transfer. By adhering to evidence-based guidelines, such as those from the CDC or WHO, women can safeguard their health and provide their babies with a vital immune head start in life.
California's Vaccine Wastage: Unraveling the Truth Behind Unused Doses
You may want to see also
Explore related products






![]()
Infant Protection Duration
Vaccines administered to pregnant individuals can confer passive immunity to their infants, but the duration of this protection varies widely depending on the vaccine type and the antibody transfer mechanism. For instance, the Tdap vaccine (tetanus, diphtheria, and pertussis) given during the third trimester provides newborns with antibodies that typically last 2-3 months, offering critical protection during the early weeks of life before the infant’s own immunizations begin. In contrast, maternal influenza vaccination can transfer antibodies that persist for up to 6 months, shielding infants from flu-related complications during their first flu season. Understanding these timelines is essential for healthcare providers to counsel parents on the transient nature of this immunity and the importance of adhering to the infant vaccination schedule.
The duration of infant protection is also influenced by the timing of maternal vaccination and the efficiency of antibody transfer across the placenta. For example, administering the Tdap vaccine between 27 and 36 weeks of gestation maximizes antibody levels in the newborn, as this window aligns with peak placental transfer. However, vaccines given earlier in pregnancy may result in lower antibody concentrations in the infant, reducing protection duration. Similarly, maternal factors such as health status, nutrition, and pre-existing immunity can affect antibody production and transfer, further complicating predictions of how long immunity will last. Parents should be aware that while maternal vaccination provides a vital early defense, it is not a substitute for the infant’s own immunizations.
A comparative analysis of different vaccines reveals disparities in protection duration that highlight the need for tailored strategies. For instance, maternal COVID-19 vaccination during pregnancy has been shown to provide infants with antibodies that can last up to 6 months, depending on the vaccine type and dosage. In contrast, antibodies from vaccines like MMR (measles, mumps, rubella) are generally not transferred in sufficient quantities to offer meaningful protection to the infant. This underscores the importance of vaccinating eligible household members to create a protective cocoon around the newborn, particularly for diseases like measles, which pose a significant risk to unvaccinated infants.
Practical tips for maximizing infant protection duration include ensuring timely maternal vaccination, maintaining a healthy lifestyle during pregnancy to optimize antibody production, and strictly following the infant vaccination schedule. For example, breastfeeding can extend the duration of certain antibody protections, as maternal antibodies are also passed through breast milk. However, this is not a replacement for maternal vaccination during pregnancy, as the initial antibody transfer via the placenta provides higher concentrations and more immediate protection. Parents should consult healthcare providers to understand the specific risks and benefits of maternal vaccination for their unique circumstances, ensuring the best possible start for their infant’s immune system.
Vaccines: A Depopulation Conspiracy or a Health Essential?
You may want to see also
Explore related products






![]()
Vaccine Safety for Mother & Baby
Vaccines during pregnancy are a critical tool for protecting both mother and baby, but safety is paramount. The World Health Organization and the Centers for Disease Control and Prevention (CDC) recommend specific vaccines, such as the flu shot and Tdap (tetanus, diphtheria, and pertussis), during pregnancy. These vaccines are rigorously tested and monitored to ensure they pose no risk to the developing fetus. For instance, the flu vaccine has been safely administered to millions of pregnant women, reducing the risk of severe illness in both mother and baby. The Tdap vaccine, given between 27 and 36 weeks of pregnancy, not only protects the mother but also passes protective antibodies to the baby, offering crucial immunity during the first few months of life before the infant can be vaccinated.
One common concern is whether vaccine ingredients could harm the baby. Vaccines recommended during pregnancy, such as the flu and Tdap shots, are inactivated or contain only a portion of the pathogen, eliminating the risk of infection. For example, the flu vaccine contains no live virus, and the Tdap vaccine’s components are carefully dosed to ensure safety. Studies show no increased risk of miscarriage, birth defects, or developmental issues associated with these vaccines. In fact, the benefits far outweigh any theoretical risks, as maternal vaccination reduces the likelihood of life-threatening infections like whooping cough, which can be fatal in infants too young to be vaccinated.
Practical considerations are key to ensuring vaccine safety. Pregnant individuals should discuss their medical history with a healthcare provider before vaccination, especially if they have severe allergies or a history of adverse reactions to vaccines. For instance, those with a severe egg allergy should receive the flu vaccine in a medical setting where allergic reactions can be managed. Timing is also crucial: the Tdap vaccine should be administered during the third trimester to maximize antibody transfer to the baby. After vaccination, mild side effects like soreness at the injection site or fatigue are normal and typically resolve within a day or two.
Comparing maternal vaccination to other protective measures highlights its unique value. While breastfeeding and good hygiene are essential, they do not provide the targeted immunity that vaccines offer. For example, breastfeeding passes some antibodies but does not protect against diseases like pertussis or influenza as effectively as vaccination. Similarly, avoiding sick individuals is impractical and insufficient, especially for highly contagious diseases. Maternal vaccination acts as a bridge, safeguarding the baby during the vulnerable period before their own immunizations begin, typically at 2 months of age.
In conclusion, vaccine safety for mother and baby is a cornerstone of prenatal care. By following evidence-based guidelines and practical tips, pregnant individuals can confidently protect themselves and their infants. The flu and Tdap vaccines are safe, effective, and specifically designed to address the unique needs of pregnancy. Their ability to transfer immunity to the baby underscores their importance in preventing severe illnesses during the critical early months of life. Always consult a healthcare provider to address concerns and ensure the best care for both mother and baby.
Vaccines and Surrogacy: Understanding the Impact on Eligibility and Process
You may want to see also
Frequently asked questions
Yes, vaccine immunity can pass to the baby during pregnancy. Antibodies produced by the mother in response to vaccination can cross the placenta, providing the baby with temporary protection against certain diseases after birth.
The duration of vaccine immunity in the baby varies depending on the vaccine. Generally, maternal antibodies can protect the baby for the first few months of life, typically up to 6 months, but this can differ based on the specific disease and vaccine.
Vaccines such as Tdap (tetanus, diphtheria, and pertussis) and influenza vaccines are recommended during pregnancy. These vaccines not only protect the mother but also pass immunity to the baby, reducing the risk of severe illness in infancy.
Yes, breastfeeding can pass some vaccine-induced immunity to the baby. Antibodies from the mother are present in breast milk, offering additional protection against certain infections during the baby’s early months.
Yes, it is safe and recommended to get certain vaccines during pregnancy, such as Tdap and flu vaccines. These vaccines protect both the mother and the baby, reducing the risk of complications from preventable diseases. Always consult your healthcare provider for personalized advice.