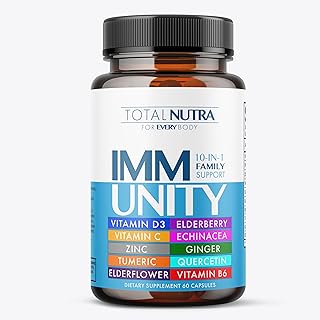
The question of whether vaccine efficacy declines over time is a critical concern in public health, particularly as vaccination campaigns expand globally. While vaccines are designed to provide robust and lasting immunity, emerging data suggests that protection against certain diseases may wane over months or years, influenced by factors such as the type of vaccine, the pathogen targeted, and individual immune responses. This phenomenon has sparked debates about the necessity of booster shots, especially in the context of COVID-19, where studies indicate a gradual decrease in antibody levels and vaccine effectiveness against infection and severe illness. Understanding the longevity of vaccine-induced immunity is essential for optimizing immunization strategies, ensuring sustained protection, and addressing potential gaps in public health defenses.
| Characteristics | Values |
|---|---|
| General Trend | Vaccine efficacy tends to decline over time for many vaccines. |
| COVID-19 Vaccines | Efficacy against symptomatic infection wanes after 6-12 months. |
| COVID-19 Booster Effect | Boosters restore efficacy to ~90% against severe disease. |
| Influenza Vaccines | Efficacy decreases within 6 months due to viral mutation and immunity fade. |
| Measles/Mumps/Rubella (MMR) | Long-lasting efficacy, often lifelong after two doses. |
| Tetanus/Diphtheria (Td) | Requires boosters every 10 years due to waning immunity. |
| Factors Affecting Decline | Immune system aging, viral evolution, vaccine type, and individual health. |
| Latest Studies (COVID-19) | Omicron variants show faster efficacy decline compared to earlier strains. |
| Public Health Recommendation | Regular boosters for vaccines with declining efficacy. |
| Individual Variability | Efficacy decline varies based on age, health, and immune response. |
Explore related products

$7.99 $14.95





What You'll Learn
- Antibody Levels Decrease: Studies show vaccine-induced antibodies wane months after vaccination, impacting protection
- Breakthrough Infections Rise: Declining immunity increases risk of vaccinated individuals contracting the virus
- Variant Impact: New variants may evade vaccine protection more as immunity weakens over time
- Booster Effectiveness: Boosters restore immunity, reducing severe illness and hospitalizations in vaccinated populations
- Immune Memory: Long-term immune memory cells may provide sustained protection despite antibody decline
![]()
Antibody Levels Decrease: Studies show vaccine-induced antibodies wane months after vaccination, impacting protection
Vaccine-induced antibodies, the body's frontline defense against pathogens, are not a permanent fixture in our immune system. Numerous studies have demonstrated a consistent trend: antibody levels decline over time, often significantly, within months of vaccination. This phenomenon is not unique to COVID-19 vaccines; it’s a well-documented characteristic of many vaccines, including those for influenza, measles, and tetanus. For instance, research published in *Nature Medicine* found that COVID-19 vaccine-induced antibodies can drop by 50–70% within 6–8 months post-vaccination, depending on the vaccine type and individual immune response.
This decline in antibody levels raises practical concerns about the durability of protection. While antibodies are just one component of immune memory, their reduction can leave individuals more susceptible to infection, particularly in the face of highly transmissible variants. For example, a study in *The Lancet* highlighted that waning antibodies contributed to increased breakthrough infections during the Delta and Omicron waves. However, it’s crucial to distinguish between antibody levels and overall immunity. Even as antibodies wane, other immune cells, such as memory B cells and T cells, often persist and can provide robust protection against severe disease, hospitalization, and death.
To mitigate the impact of declining antibody levels, health authorities have recommended booster doses for many vaccines. For COVID-19, boosters have been shown to restore antibody levels to peak post-vaccination levels, offering renewed protection against infection and severe outcomes. For instance, a Pfizer-BioNTech booster dose administered 6 months after the initial series increased antibody titers by 20-fold within a week, according to data from the CDC. Similarly, seasonal flu vaccines are reformulated annually to account for waning immunity and viral evolution, emphasizing the need for periodic reinforcement of immune responses.
Age and underlying health conditions play a significant role in how quickly antibody levels decline. Older adults and immunocompromised individuals often experience faster waning of antibodies due to age-related immune decline or suppressed immune function. For these populations, tailored vaccination strategies, such as additional doses or adjuvanted vaccines, may be necessary to maintain protective immunity. Practical tips include staying updated on booster recommendations, monitoring local disease prevalence, and adopting preventive measures like masking during outbreaks, especially for those at higher risk.
In conclusion, while declining antibody levels are a natural part of the immune response to vaccination, they underscore the importance of proactive measures to sustain protection. Boosters, personalized vaccination schedules, and public health awareness can help bridge the gap created by waning immunity. Understanding this dynamic not only informs individual health decisions but also shapes broader vaccination policies to ensure continued defense against evolving pathogens.
Vaccines, Mercury, and Fetus: Separating Fact from Fiction
You may want to see also
Explore related products






![]()
Breakthrough Infections Rise: Declining immunity increases risk of vaccinated individuals contracting the virus
Vaccine efficacy, while robust in the initial months post-inoculation, is not a static shield. Studies show a gradual decline in protection against infection over time, particularly for mRNA vaccines like Pfizer-BioNTech and Moderna. This waning immunity, coupled with the emergence of new variants, has led to a rise in breakthrough infections among vaccinated individuals. Data from the CDC indicates that while vaccines remain highly effective in preventing severe illness and hospitalization, their ability to prevent mild to moderate infection diminishes significantly 6-8 months after the second dose.
For instance, a study published in *The Lancet* found that Pfizer’s vaccine efficacy against infection dropped from 88% within one month of full vaccination to 47% after six months. This decline is more pronounced in older adults and those with underlying health conditions, whose immune systems may mount a less robust response to the vaccine.
Understanding this trend is crucial for public health strategies. Booster shots, administered 6-8 months after the initial series, have proven effective in restoring antibody levels and reducing the risk of breakthrough infections. Israel’s booster campaign, for example, demonstrated a 10-fold reduction in infections among those who received a third dose compared to those who did not. However, the timing and frequency of boosters remain under debate, with some experts cautioning against over-reliance on repeated doses without addressing the root causes of waning immunity, such as viral evolution.
From a practical standpoint, vaccinated individuals should not abandon preventive measures entirely. Mask-wearing in crowded indoor spaces, regular hand hygiene, and avoiding close contact with sick individuals remain essential, especially for those at higher risk. Additionally, staying informed about local infection rates and variant prevalence can guide decision-making. For those eligible, scheduling a booster dose is a proactive step to reinforce immunity. It’s also worth noting that certain populations, such as immunocompromised individuals, may require additional doses or alternative vaccination strategies to achieve adequate protection.
Comparatively, the decline in vaccine efficacy highlights the dynamic nature of the immune response and the virus itself. Unlike vaccines for diseases like measles, which confer near-lifelong immunity, COVID-19 vaccines face the challenge of a rapidly mutating virus. This underscores the need for ongoing research into next-generation vaccines that target conserved viral regions or induce broader immune responses. Until then, a multi-layered approach—combining vaccination, boosters, and behavioral precautions—remains the most effective strategy to mitigate the risk of breakthrough infections.
Home-Schooled Kids: Are Vaccines Mandatory?
You may want to see also
Explore related products





![]()
Variant Impact: New variants may evade vaccine protection more as immunity weakens over time
The emergence of new variants poses a significant challenge to vaccine efficacy, particularly as immunity wanes over time. SARS-CoV-2, the virus causing COVID-19, has demonstrated a remarkable ability to mutate, leading to variants like Delta and Omicron that exhibit increased transmissibility and immune evasion. Studies show that while vaccines remain highly effective against severe disease and hospitalization, their protection against infection and mild illness can diminish within 6 to 12 months post-vaccination. This decline is more pronounced in older adults and immunocompromised individuals, whose immune systems may not mount as robust a response to the initial vaccine series.
Consider the Omicron variant, which harbors over 30 mutations in its spike protein—the primary target of most COVID-19 vaccines. These mutations reduce the binding affinity of neutralizing antibodies, rendering the immune response less effective. For instance, research published in *Nature Medicine* found that vaccine efficacy against symptomatic Omicron infection dropped to approximately 30% after 6 months, compared to over 80% efficacy against earlier strains like Alpha. Booster doses, however, have proven critical in restoring protection, with a third dose increasing neutralizing antibody titers by 20- to 30-fold, according to the CDC. This underscores the importance of timely boosters, particularly for high-risk populations.
To mitigate the impact of variants, public health strategies must adapt. First, individuals should adhere to booster schedules, with most health authorities recommending a booster 5 to 6 months after the initial series. Second, vaccine manufacturers are developing variant-specific formulations, such as bivalent vaccines targeting both the original strain and Omicron subvariants. These updated vaccines have shown improved efficacy against circulating strains. Third, monitoring viral evolution through genomic surveillance is essential to identify emerging variants early and guide vaccine updates.
Practical tips for individuals include staying informed about local variant prevalence and vaccination recommendations. For those over 65 or with underlying conditions, consulting a healthcare provider about additional precautions, such as masking in crowded settings, can provide an extra layer of protection. Finally, maintaining overall immune health through adequate sleep, nutrition, and physical activity supports the body’s ability to respond to vaccines and combat infections.
In conclusion, while vaccines remain a cornerstone of pandemic control, the interplay between waning immunity and variant evolution necessitates proactive measures. By combining booster doses, variant-specific vaccines, and individual vigilance, societies can stay ahead of the virus’s shifting landscape. This dynamic approach ensures that vaccine protection remains robust, even as new challenges arise.
U.S. Vaccination Rates: Tracking COVID-19 Immunization Progress Nationwide
You may want to see also
Explore related products





![]()
Booster Effectiveness: Boosters restore immunity, reducing severe illness and hospitalizations in vaccinated populations
Vaccine efficacy naturally wanes over time, a phenomenon observed across various vaccines, including those for influenza, tetanus, and COVID-19. This decline in immunity leaves individuals more susceptible to infection, severe illness, and hospitalization. Boosters, additional doses administered after the initial vaccine series, serve as a critical tool to counteract this waning immunity. By reintroducing the antigen to the immune system, boosters stimulate memory cells, enhancing antibody production and restoring protective immunity. This renewed immune response significantly reduces the risk of severe outcomes, even in the face of evolving variants.
Consider the COVID-19 vaccines as a prime example. Studies have shown that while initial vaccine efficacy against symptomatic infection may drop from around 95% to 60-70% within 6 months, protection against severe disease and hospitalization remains robust, often above 90%. However, this residual protection can also diminish over time, particularly in older adults and immunocompromised individuals. Boosters, typically administered 6-12 months after the primary series, have been shown to restore antibody levels to peak post-vaccination levels, providing a substantial increase in protection. For instance, a Pfizer-BioNTech booster dose has been found to increase antibody titers by 20-fold, significantly reducing the risk of hospitalization and death.
The effectiveness of boosters is not limited to antibody responses. They also enhance cellular immunity, which plays a crucial role in long-term protection. T cells, a key component of cellular immunity, recognize and destroy infected cells, providing a secondary line of defense. Boosters reinforce this T cell response, ensuring a more comprehensive and durable immune memory. This dual-action approach is particularly vital in combating viruses like SARS-CoV-2, which continues to mutate and evade immune responses.
Practical considerations for booster administration are essential. Timing is critical; boosters should be administered when vaccine efficacy has noticeably declined but before individuals become vulnerable to severe disease. For COVID-19 vaccines, the CDC recommends boosters for individuals aged 12 and older, with specific intervals depending on the primary vaccine series. For example, Pfizer and Moderna recipients should receive a booster 5 months after their second dose, while Johnson & Johnson recipients are advised to get a booster 2 months after their initial dose. Additionally, certain populations, such as those over 65 or with underlying health conditions, may benefit from additional boosters to maintain optimal protection.
In conclusion, boosters are a vital component of vaccine strategies, effectively restoring immunity and reducing the burden of severe illness and hospitalizations. Their ability to rejuvenate both antibody and cellular immune responses makes them indispensable in the fight against infectious diseases. By adhering to recommended booster schedules and staying informed about evolving guidelines, individuals can maximize their protection and contribute to public health efforts. As vaccine efficacy continues to be studied, boosters will remain a cornerstone of maintaining herd immunity and mitigating the impact of infectious diseases.
North Carolina Vaccine Exemptions: What You Need to Know
You may want to see also
Explore related products






![]()
Immune Memory: Long-term immune memory cells may provide sustained protection despite antibody decline
Vaccine efficacy often appears to wane over time, with antibody levels dropping months or years after immunization. However, this decline doesn’t necessarily signal a loss of protection. The immune system’s memory cells—specifically memory B cells and memory T cells—play a critical role in maintaining long-term defense. Unlike antibodies, which circulate in the blood and can diminish, memory cells persist in lymphoid tissues, ready to rapidly respond if the pathogen reappears. For instance, studies on the measles vaccine show that while antibody titers decrease over decades, memory cells remain active, ensuring swift and effective protection upon re-exposure.
Consider the immune response as a well-rehearsed orchestra. Antibodies are the first violins, leading the initial attack, but memory cells are the conductors, ensuring the symphony can restart at a moment’s notice. Memory B cells, upon encountering the same pathogen, quickly differentiate into antibody-producing plasma cells, restoring immunity. Memory T cells, particularly CD8+ T cells, target and destroy infected cells, preventing the pathogen from establishing a foothold. This dual mechanism explains why vaccines like the yellow fever vaccine provide lifelong immunity despite declining antibody levels.
Practical implications of this immune memory are evident in booster recommendations. For example, the COVID-19 mRNA vaccines initially induce high antibody levels, which wane over 6–12 months. However, memory cells persist, enabling a robust response to boosters or infection. Adults over 50, who often experience age-related immune decline (immunosenescence), benefit significantly from boosters, as they reactivate memory cells and enhance protection. Similarly, the Tdap vaccine (tetanus, diphtheria, pertussis) relies on memory cells to provide sustained immunity, even as antibody levels drop.
To maximize the benefits of immune memory, timing and dosage matter. Spacing vaccine doses optimally (e.g., 4–8 weeks apart for COVID-19 boosters) allows memory cells to mature fully. For children, adhering to the CDC’s immunization schedule ensures memory cells develop during critical immune system maturation periods. For travelers to high-risk areas, a booster dose 1–2 months before departure can reactivate memory cells, providing immediate protection. Understanding this mechanism also reduces reliance on frequent antibody testing, as memory cell activity is a more reliable indicator of long-term immunity.
In summary, while antibody decline may raise concerns about vaccine efficacy, immune memory cells provide a durable safety net. This knowledge shifts the focus from antibody titers to the immune system’s ability to “remember” and respond. By leveraging this mechanism through strategic vaccination schedules and boosters, individuals can maintain robust protection against pathogens, even years after initial immunization. The takeaway? Antibodies may fade, but immune memory endures, offering sustained defense against disease.
Antibiotics and Vaccines: How Long Do They Stay in Your System?
You may want to see also
Frequently asked questions
Yes, vaccine efficacy can decline over time due to factors like waning immunity, viral mutations, or individual differences in immune response.
The rate of decline varies by vaccine type and individual factors, but studies show efficacy may start to wane after 6–12 months for some vaccines.
No, declining efficacy typically means reduced protection against mild or moderate illness, but vaccines often remain highly effective at preventing severe disease, hospitalization, and death.
Yes, booster shots can significantly increase antibody levels and restore or enhance protection, especially against emerging variants.
Yes, vaccines targeting rapidly mutating viruses (e.g., influenza, COVID-19) may show more noticeable declines in efficacy compared to those for stable viruses (e.g., measles).








![Premium 10 in 1 Immune Support Supplement [10 Potent Ingredients] with Elderberry, Vitamin C, Echinacea, Zinc and Probiotic for Immune Support, Gut Health and Better Digestion, 60 Veg Caps](https://m.media-amazon.com/images/I/81oOkSABw-L._AC_UL320_.jpg)