The question of whether the military administers the smallpox vaccine is a significant one, rooted in historical context and modern preparedness. Smallpox, a devastating disease eradicated in the wild since 1980, remains a concern due to its potential use as a biological weapon. Historically, military personnel were routinely vaccinated against smallpox to protect troops in high-risk areas. However, with the disease's eradication, routine vaccination ceased for the general population. Today, select military personnel, particularly those deployed to regions with potential bioterrorism threats, may still receive the smallpox vaccine as part of their protective measures. This targeted approach balances the risks of the vaccine with the need to safeguard military forces against potential threats.
| Characteristics | Values |
|---|---|
| Current Military Smallpox Vaccination Policy (USA) | The U.S. military does not routinely administer the smallpox vaccine to all service members. |
| Target Groups for Vaccination | Only specific groups considered at high risk, such as certain laboratory workers and rapid response teams, receive the smallpox vaccine. |
| Vaccine Used | ACAM2000, a second-generation smallpox vaccine derived from the New York City Board of Health strain of vaccinia virus. |
| Reason for Limited Vaccination | Smallpox was eradicated globally in 1980, and the risk of natural exposure is extremely low. |
| Preparedness Measures | The U.S. government maintains a stockpile of smallpox vaccine for emergency use in case of a bioterrorism event or outbreak. |
| Historical Context | Routine smallpox vaccination ended in the U.S. in 1972, and globally in 1980 after eradication. |
| Military Vaccination Post-9/11 | After the 2001 anthrax attacks, the U.S. military vaccinated select personnel against smallpox as a precautionary measure, but this program was later discontinued. |
| Side Effects of ACAM2000 | Common side effects include soreness at the injection site, fever, and fatigue. Rare but serious adverse events include progressive vaccinia and myopericarditis. |
| Contraindications | The vaccine is not administered to individuals with weakened immune systems, certain skin conditions (e.g., eczema), or those who are pregnant. |
| Global Military Practices | Policies vary by country, but most militaries do not routinely vaccinate against smallpox due to the disease's eradication. |
Explore related products






What You'll Learn
- Vaccine Type: What specific smallpox vaccine does the military use for its personnel
- Administration Protocol: How and when is the smallpox vaccine administered to military members
- Side Effects: What are the common side effects of the military’s smallpox vaccine
- Mandatory Vaccination: Is smallpox vaccination mandatory for all military personnel
- Historical Use: Has the military historically administered smallpox vaccines, and why
![]()
Vaccine Type: What specific smallpox vaccine does the military use for its personnel?
The U.S. military administers the ACAM2000 smallpox vaccine to its personnel as part of its biodefense preparedness program. This vaccine, approved by the FDA in 2007, is a second-generation smallpox vaccine derived from the New York City Board of Health (Dryvax) strain of the vaccinia virus. Unlike earlier smallpox vaccines, ACAM2000 is produced under modern manufacturing standards, ensuring consistency and safety. It is administered using a bifurcated needle, which is dipped into the vaccine solution and then used to prick the skin 15 times in a specific pattern, typically on the upper arm. This method creates a localized immune response, resulting in a characteristic "take" lesion at the vaccination site.
Dosage and Administration
The ACAM2000 vaccine is administered as a single dose of 0.3 mL for primary vaccinations. For individuals who have previously received a smallpox vaccine, a lower dose of 0.1 mL may be used for revaccination. The vaccine is contraindicated in individuals with certain conditions, such as eczema, atopic dermatitis, or weakened immune systems, due to the risk of severe adverse reactions. Personnel must undergo a thorough screening process before vaccination, including a detailed medical history and skin examination, to identify potential risks. The vaccine is typically administered to service members deemed at high risk of exposure to smallpox, such as those deploying to areas of potential bioterrorism threats.
Efficacy and Side Effects
ACAM2000 provides robust immunity against smallpox, with studies showing that 97% of vaccinees develop a protective immune response within 28 days of vaccination. However, the vaccine is associated with a range of side effects, from mild to severe. Common reactions include pain, swelling, and itching at the vaccination site, as well as headache and fatigue. More serious adverse events, such as progressive vaccinia (a rare but life-threatening condition) and myopericarditis (inflammation of the heart), are rare but require immediate medical attention. The military closely monitors vaccinated personnel to manage and mitigate these risks, often providing educational materials and access to medical support.
Practical Considerations for Military Personnel
Service members receiving ACAM2000 must follow specific post-vaccination care instructions to prevent complications. The vaccination site should be kept covered with a semi-occlusive bandage until the scab falls off naturally, typically within 3–4 weeks. Personnel are advised to avoid touching or scratching the site and to refrain from activities that could transfer the vaccinia virus to others, such as sharing clothing or towels. Additionally, individuals with a "take" lesion should avoid close contact with immunocompromised individuals, pregnant women, and those with skin conditions until the lesion is fully healed. The military emphasizes the importance of compliance with these guidelines to ensure both individual and collective safety.
Comparative Perspective
While ACAM2000 is the primary smallpox vaccine used by the U.S. military, it is worth noting that other countries and organizations may use different vaccines, such as LC16m8, a attenuated vaccinia virus vaccine developed in Japan. LC16m8 is associated with fewer adverse effects but is not approved for use in the United States. The military’s choice of ACAM2000 reflects a balance between efficacy, availability, and adherence to U.S. regulatory standards. This decision underscores the military’s commitment to protecting its personnel against bioterrorism threats while minimizing risks associated with vaccination. Understanding the specifics of ACAM2000 is essential for military personnel and healthcare providers involved in smallpox vaccination programs.
Access Your Nevada Vaccination Records Easily on MyNevada Portal
You may want to see also
Explore related products






![]()
Administration Protocol: How and when is the smallpox vaccine administered to military members?
The smallpox vaccine, known as the ACAM2000 vaccine, is administered to military personnel under specific protocols designed to ensure both safety and efficacy. The primary method of administration is through a unique technique called scarification, where the vaccine is introduced into the skin using a bifurcated needle. This needle is dipped into the vaccine solution and then used to prick the skin 15 times in a small area, typically on the upper arm. This process creates a localized immune response, leading to the formation of a vaccine "take," which appears as a red, itchy bump that eventually scabbed over. The goal is to achieve a major reaction, defined as a blister or ulcer at the vaccination site, surrounded by erythema and edema, which indicates a successful immune response.
Timing and Eligibility
The smallpox vaccine is administered to military members based on deployment risk and operational requirements. Typically, service members are vaccinated if they are deploying to areas deemed high-risk for smallpox exposure or bioterrorism threats. Vaccination is not routine for all personnel but is targeted to specific units or individuals. The initial vaccination is followed by a revaccination protocol, where boosters are given every 3 to 10 years, depending on ongoing risk assessments. Notably, the vaccine is contraindicated for certain groups, including individuals with weakened immune systems, skin conditions like eczema, or those who are pregnant. Screening for these conditions is mandatory before administration to prevent adverse reactions.
Dosage and Handling
The ACAM2000 vaccine is administered using a precise dosage of 0.0025 mL, delivered via the scarification method. The vaccine is stored frozen and must be reconstituted with diluent before use. Once prepared, it remains stable at room temperature for up to 8 hours but should be discarded if not used within this timeframe. Proper handling is critical, as the live vaccinia virus in the vaccine can cause inadvertent inoculation if mishandled. Healthcare providers administering the vaccine must wear gloves and ensure the vaccination site is covered with a semi-occlusive bandage to prevent transmission of the virus to others.
Post-Vaccination Care and Monitoring
After vaccination, military personnel are instructed to keep the vaccination site clean and covered until the scab falls off naturally, typically within 3 to 4 weeks. They are advised to avoid touching or scratching the site and to wash hands thoroughly if contact occurs. Close monitoring is essential, as adverse reactions, though rare, can include severe skin reactions, progressive vaccinia, or post-vaccinial encephalitis. Military medical teams provide education on recognizing symptoms of complications and emphasize the importance of reporting any unusual reactions immediately. Additionally, vaccinated individuals are restricted from close contact with immunocompromised persons or pregnant women until the vaccination site is fully healed to prevent secondary transmission of the vaccinia virus.
Strategic Considerations and Practical Tips
The administration of the smallpox vaccine in the military is a strategic decision tied to national security and force readiness. Commanders and medical officers must balance the need for protection against the potential disruption caused by vaccine-related adverse events. Practical tips for service members include wearing loose-fitting clothing to avoid friction on the vaccination site and avoiding strenuous activity that could exacerbate the reaction. Units are often staggered in their vaccination schedules to ensure operational readiness is maintained. This protocol underscores the military’s commitment to safeguarding personnel while maintaining mission capability in the face of potential biological threats.
Unraveling the Origins of the Autism-Vaccine Study Controversy
You may want to see also
Explore related products






![]()
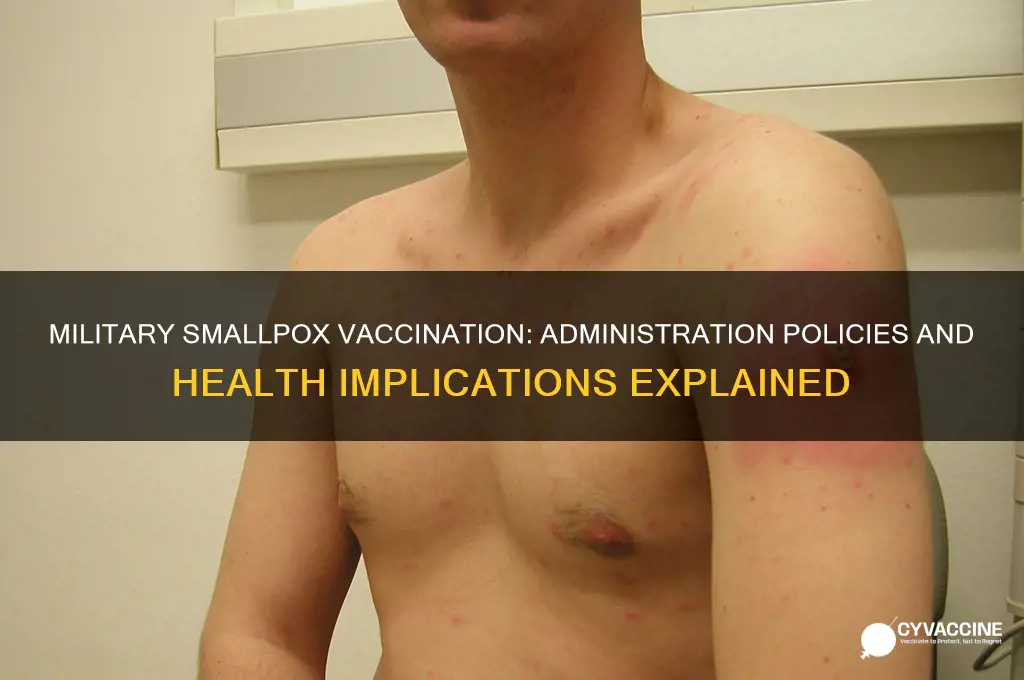
Side Effects: What are the common side effects of the military’s smallpox vaccine?
The military's smallpox vaccine, known as the ACAM2000, is a live virus vaccine that has been administered to service members and certain civilian populations as part of preparedness efforts against potential bioterrorism threats. While the vaccine is highly effective in preventing smallpox, it is associated with a range of side effects that can vary in severity. Understanding these side effects is crucial for anyone receiving the vaccine, as it helps in managing symptoms and recognizing when medical attention is necessary.
Common Local Reactions: The most frequent side effects are localized to the vaccination site. After receiving the vaccine, a small bump appears, which progresses into a blister and eventually forms a scab. This process is normal and indicates a successful immune response. However, some individuals may experience more pronounced reactions, such as swelling, redness, and tenderness around the site. These symptoms typically resolve within a few weeks but can be managed with clean dressings and over-the-counter pain relievers like acetaminophen. It’s essential to keep the area clean and avoid scratching or picking at the scab to prevent infection.
Systemic Symptoms: Beyond local reactions, the smallpox vaccine can cause systemic side effects, particularly in the first two weeks after vaccination. These may include fatigue, headache, muscle aches, and low-grade fever. Such symptoms are generally mild to moderate and can be alleviated with rest and hydration. However, if a high fever (above 102°F or 38.9°C) develops, it could indicate a more serious reaction, such as vaccine-induced encephalitis or eczema vaccinatum, especially in individuals with weakened immune systems or skin conditions. Immediate medical evaluation is necessary in these cases.
Rare but Serious Complications: While uncommon, the smallpox vaccine carries risks of severe adverse events. One such complication is progressive vaccinia, where the virus spreads beyond the vaccination site, causing widespread skin lesions. Another is postvaccinial encephalitis, a potentially life-threatening inflammation of the brain. These conditions are more likely to occur in immunocompromised individuals, including those with HIV, cancer, or autoimmune disorders. Pregnant women and individuals with eczema or other skin conditions are also at higher risk. Exclusion criteria for vaccination are strictly enforced to minimize these risks, and anyone with a history of these conditions should not receive the vaccine.
Practical Tips for Management: To minimize side effects, recipients should follow post-vaccination care guidelines. Avoid touching or covering the vaccination site unnecessarily, and ensure that anyone who comes into contact with the lesion or scab takes precautions to prevent transmission. Immunocompromised individuals and close contacts of vaccine recipients should be particularly vigilant, as they are at higher risk of contracting vaccinia virus. If unusual symptoms develop, such as severe pain, confusion, or rapid spread of the rash, seek medical attention promptly. Understanding and monitoring these side effects ensures the safe and effective use of the smallpox vaccine in military and civilian populations.
Pharmaceutical Companies' Role in Vaccine Manufacturing for LMICs
You may want to see also
Explore related products






![]()
Mandatory Vaccination: Is smallpox vaccination mandatory for all military personnel?
Smallpox vaccination policies within the military are not uniform across all branches or nations, reflecting a complex interplay of historical context, current threat assessments, and logistical considerations. In the United States, for instance, the Department of Defense (DoD) has historically mandated smallpox vaccination for specific personnel, particularly those deployed to high-risk areas or involved in critical missions. This policy is rooted in the vaccine's proven efficacy in preventing smallpox, a disease eradicated in the wild but still considered a potential bioterrorism threat. The vaccine, known as ACAM2000, is administered as a single dose via a prong-like device that punctures the skin, delivering the live vaccinia virus. This method, while effective, carries risks such as myocarditis and pericarditis, necessitating careful screening of recipients.
From an analytical perspective, the decision to mandate smallpox vaccination for military personnel hinges on balancing individual health risks against collective security needs. The vaccine’s side effects, though rare, can be severe, particularly in individuals with compromised immune systems or certain skin conditions. However, the strategic importance of maintaining a healthy, mission-ready force often outweighs these concerns. For example, during the 2002-2003 U.S. smallpox vaccination program, over 450,000 service members were vaccinated, with adverse events monitored closely. This data-driven approach allows military health authorities to refine protocols, ensuring that only those at minimal risk receive the vaccine.
Instructively, the process of administering smallpox vaccines in the military involves rigorous pre-vaccination screening. Personnel are evaluated for contraindications such as atopic dermatitis, HIV/AIDS, or pregnancy. Post-vaccination care includes monitoring the vaccination site for the characteristic "take"—a raised bump indicating a successful immune response—and educating recipients on preventing transmission of the vaccinia virus to others. Practical tips include covering the site with a bandage and avoiding contact with immunocompromised individuals until the lesion heals, typically within 3-4 weeks.
Persuasively, the argument for mandatory smallpox vaccination in the military rests on its role as a deterrent against bioterrorism. Smallpox, with its high mortality rate and ease of dissemination, remains a credible threat in an increasingly volatile global landscape. Vaccinating military personnel not only protects individual service members but also ensures operational continuity in the event of an outbreak. Critics argue that the risks of adverse reactions outweigh the benefits, but proponents counter that the vaccine’s track record in eradicating smallpox globally demonstrates its safety and efficacy when properly administered.
Comparatively, smallpox vaccination policies in the military differ significantly from civilian practices. While civilians are generally vaccinated only in response to a confirmed outbreak, military personnel may be vaccinated preemptively based on deployment locations or mission profiles. This proactive approach underscores the military’s unique role in safeguarding national security, even at the cost of individual inconvenience or risk. For instance, the U.S. military’s smallpox vaccination program contrasts with the CDC’s recommendation for civilians, which limits vaccination to laboratory workers and first responders.
In conclusion, smallpox vaccination is not universally mandatory for all military personnel but is selectively required based on strategic and operational considerations. The process involves careful screening, precise administration, and vigilant monitoring to maximize benefits while minimizing risks. As bioterrorism threats evolve, so too will vaccination policies, reflecting the military’s dual commitment to protecting its members and fulfilling its mission. For service members, understanding these policies and their rationale is essential for informed participation in this critical public health measure.
Disease vs. Vaccines: Which Triggers Autoimmunity More Often?
You may want to see also
Explore related products






![]()
Historical Use: Has the military historically administered smallpox vaccines, and why?
The military's role in smallpox vaccination dates back to the 18th century, when armies were among the first institutions to systematically administer the vaccine. During the American Revolutionary War, General George Washington mandated smallpox inoculation for all Continental soldiers, recognizing the disease as a greater threat than enemy fire. This decision was driven by the devastating impact of smallpox outbreaks on troop readiness and morale. By 1777, Washington’s campaign had significantly reduced smallpox cases in the army, demonstrating the military’s early adoption of vaccination as a strategic health measure.
In the 19th and early 20th centuries, military vaccination programs expanded globally, particularly during colonial campaigns and World Wars I and II. British and French forces routinely vaccinated troops deployed to regions where smallpox was endemic, such as India and West Africa. The U.S. military, for instance, administered the Dryvax vaccine—a lyophilized (freeze-dried) form of the smallpox vaccine—to millions of service members during World War II and the Vietnam War. Dosage typically involved a single application of the vaccine using a bifurcated needle, creating a localized infection that conferred immunity. These efforts were not only protective but also preventive, aiming to halt the spread of smallpox in densely populated military camps.
The rationale behind military smallpox vaccination was twofold: operational necessity and public health. Smallpox posed a unique threat to military operations due to its high transmissibility and mortality rate. A single case could incapacitate entire units, disrupt supply lines, and undermine mission success. Moreover, soldiers returning home risked introducing smallpox to civilian populations, making vaccination a dual-purpose tool for both military and societal protection. This dual role underscores the military’s historical position as both a consumer and a distributor of smallpox vaccines.
Comparatively, military vaccination campaigns differed from civilian efforts in scale, urgency, and enforcement. While civilian programs often relied on voluntary participation, military vaccination was mandatory, ensuring high compliance rates. The military also pioneered techniques for mass vaccination, such as the use of bifurcated needles, which were later adopted by global eradication efforts. For example, the World Health Organization’s smallpox eradication campaign in the 1960s and 1970s drew heavily on military logistics and vaccination strategies.
Today, the military’s historical role in smallpox vaccination serves as a case study in the intersection of defense and public health. While routine smallpox vaccination ceased globally after eradication in 1980, the military retains stockpiles of the vaccine (e.g., ACAM2000) for emergency use, such as bioterrorism threats. This legacy highlights the military’s enduring responsibility to protect both its personnel and the broader population from infectious diseases, a role that continues to evolve in the face of emerging health challenges.
Yellow Fever Vaccine: Who Needs It?
You may want to see also
Frequently asked questions
No, the military does not routinely administer the smallpox vaccine to all service members. Vaccination is reserved for specific high-risk groups, such as certain laboratory personnel and select military units with potential exposure risks.
The military maintains a stockpile of smallpox vaccine as a precautionary measure against potential bioterrorism threats or outbreaks. Smallpox was eradicated globally, but concerns about weaponized smallpox persist.
Only specific military personnel, such as those involved in biodefense or deployed to high-risk areas, receive the smallpox vaccine. It is not part of standard immunizations for all service members.
Yes, the smallpox vaccine can cause side effects, including a sore arm, fever, fatigue, and a localized rash at the vaccination site. Rarely, more serious reactions like progressive vaccinia or eczema vaccinatum can occur, particularly in immunocompromised individuals.