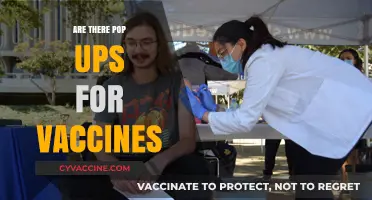
Hepatitis C, a liver infection caused by the hepatitis C virus (HCV), has long been a significant public health concern due to its potential for chronic liver damage, cirrhosis, and liver cancer. While antiviral treatments have advanced dramatically in recent years, offering cure rates exceeding 95%, the development of a vaccine for hepatitis C remains an ongoing challenge. Unlike hepatitis A and B, which have effective vaccines, no vaccine currently exists for hepatitis C. This is primarily due to the virus's high genetic variability and its ability to evade the immune system. However, research efforts continue, with several vaccine candidates in clinical trials, aiming to prevent HCV infection and reduce the global burden of this disease.
| Characteristics | Values |
|---|---|
| Vaccination Availability | No approved vaccine for Hepatitis C currently exists. |
| Research Status | Multiple vaccine candidates are in clinical trials (e.g., phase 1, 2, 3). |
| Challenges | High genetic diversity of HCV, lack of natural immunity after infection. |
| Prevention Methods | Harm reduction (e.g., safe injection practices), screening, antiviral treatment. |
| Global Efforts | WHO and research institutions actively pursuing vaccine development. |
| Estimated Timeline | No definitive timeline; progress depends on trial outcomes. |
| Current Treatment | Direct-acting antivirals (DAAs) cure >95% of cases but do not prevent reinfection. |
| Risk Factors | Injection drug use, unsafe medical procedures, unprotected sex. |
| Global Burden | ~58 million people chronically infected worldwide (as of 2023). |
| Public Health Goal | Eliminate Hepatitis C by 2030 (WHO target). |
Explore related products






What You'll Learn
![]()
Current Hepatitis C Vaccines
Unlike hepatitis A and B, there is currently no commercially available vaccine for hepatitis C. Despite decades of research, developing an effective vaccine has proven challenging due to the virus's remarkable ability to mutate and evade the immune system. Hepatitis C virus (HCV) exists in multiple genotypes, each with numerous subtypes, making a universal vaccine a complex endeavor. While this may seem discouraging, ongoing research offers a glimmer of hope.
Several promising candidates are in various stages of clinical trials, employing diverse strategies to tackle the virus. Some approaches focus on stimulating the production of neutralizing antibodies that can prevent HCV from entering liver cells. Others aim to boost the body's cellular immune response, enabling it to recognize and destroy infected cells.
One notable example is a vaccine candidate based on recombinant viral vectors, which uses a harmless virus to deliver HCV proteins into the body, triggering an immune response. Early trials have shown encouraging results, with participants developing both antibody and T-cell responses. Another strategy involves using synthetic peptides, short chains of amino acids, that mimic key HCV proteins, potentially offering a more targeted and controlled immune stimulation.
These advancements highlight the dedication of researchers to finding a preventive solution for hepatitis C. While a widely available vaccine remains a goal for the future, the progress made in recent years is a testament to the power of scientific innovation and our unwavering commitment to combating this global health challenge.
Preventing Tetanus Naturally: Safe Strategies for the Unvaccinated
You may want to see also
Explore related products





![]()
Challenges in Vaccine Development
Hepatitis C virus (HCV) infects an estimated 58 million people globally, yet no vaccine exists. This absence isn’t for lack of effort. Decades of research have revealed formidable obstacles that complicate vaccine development, each demanding innovative solutions. One primary challenge lies in HCV’s extraordinary genetic diversity. The virus exists in seven distinct genotypes, each with numerous subtypes, making a universal vaccine akin to hitting a moving target. Unlike hepatitis B, where a single vaccine protects broadly, HCV’s variability requires a vaccine capable of eliciting immune responses against multiple strains simultaneously.
Compounding this issue is HCV’s ability to evade the immune system. The virus mutates rapidly, altering its surface proteins to escape detection by antibodies. This phenomenon, known as immune evasion, frustrates traditional vaccine approaches that rely on inducing neutralizing antibodies. Researchers must identify conserved viral regions less prone to mutation, a task akin to finding a needle in a haystack. Additionally, HCV establishes chronic infections in 70-85% of cases, further complicating vaccine design. A successful vaccine must not only prevent initial infection but also disrupt viral persistence, a dual challenge few vaccines have tackled.
Another hurdle is the lack of a robust animal model. While chimpanzees were historically used, their endangered status and ethical concerns have halted their use. Current alternatives, such as humanized mouse models, fail to fully replicate HCV infection dynamics. This limits our ability to test vaccine candidates in vivo, slowing progress. Without an accurate model, researchers must rely heavily on in vitro studies and human trials, increasing costs and timelines.
Finally, the population most affected by HCV—individuals with a history of injection drug use, unscreened blood transfusions, or healthcare exposure—often faces barriers to vaccine access. Stigma, socioeconomic disparities, and fragmented healthcare systems complicate distribution efforts. Even if a vaccine were developed, ensuring equitable access would require addressing these systemic challenges. For instance, a multi-dose regimen might be impractical for marginalized populations, necessitating a single-dose formulation with long-lasting immunity.
Despite these challenges, recent advances offer hope. Novel technologies like mRNA platforms and viral vector-based vaccines, proven effective against COVID-19, are being explored for HCV. Early-stage trials are investigating T-cell-based vaccines that target conserved viral proteins, bypassing the need for neutralizing antibodies. While the path to an HCV vaccine remains fraught, each obstacle presents an opportunity for innovation. Success would not only prevent millions of infections but also serve as a blueprint for tackling other complex pathogens.
Breast Milk Composition: Vaccines and Changes
You may want to see also
Explore related products






![]()
Preventive Measures Without Vaccination
Unlike hepatitis A and B, there is currently no vaccine available for hepatitis C. This leaves prevention strategies focused on behavioral changes and harm reduction techniques.
Understanding how the virus spreads is crucial. Hepatitis C is primarily transmitted through contact with infected blood. This means sharing needles or other drug paraphernalia is a major risk factor. Even a microscopic amount of blood can carry the virus.
Harm Reduction Strategies:
The cornerstone of prevention without vaccination lies in harm reduction practices. For individuals who inject drugs, accessing sterile needles and syringes through needle exchange programs is vital. These programs not only provide clean equipment but often offer testing, counseling, and referrals to treatment. Additionally, never share personal care items like razors, toothbrushes, or nail clippers, as they can carry trace amounts of blood.
In healthcare settings, strict adherence to universal precautions is essential. This includes wearing gloves when handling blood or bodily fluids, proper disposal of sharps, and thorough disinfection of equipment.
Sexual Transmission and Awareness:
While less common than bloodborne transmission, sexual contact can also spread hepatitis C, especially among individuals with multiple partners or those engaging in rough sex. Using condoms consistently and correctly significantly reduces this risk. Open communication with sexual partners about hepatitis C status and practicing safer sex are crucial preventive measures.
Screening and Early Detection:
Early detection is key to preventing the spread of hepatitis C and ensuring timely treatment. Individuals at higher risk, such as those with a history of injection drug use, blood transfusions before 1992, or long-term hemodialysis, should be regularly screened for the virus. Modern antiviral treatments can cure hepatitis C in most cases, preventing long-term complications like cirrhosis and liver cancer.
Public Health Initiatives:
Public health efforts play a vital role in preventing hepatitis C transmission. This includes educating at-risk populations about the virus, promoting harm reduction strategies, and ensuring access to testing and treatment. By addressing the social and economic factors that contribute to risk behaviors, we can create a more comprehensive approach to hepatitis C prevention.
Skipping Your Second Vaccine Dose: Risks and Consequences Explained
You may want to see also
Explore related products





![]()
Ongoing Research and Trials
Despite the absence of a hepatitis C vaccine, ongoing research and trials are pushing the boundaries of what’s possible. One promising approach involves mRNA technology, the same platform that revolutionized COVID-19 vaccines. Researchers are exploring mRNA-based vaccines that encode hepatitis C virus (HCV) antigens, aiming to stimulate a robust immune response. Early preclinical studies show that these vaccines can elicit neutralizing antibodies in animal models, offering a glimmer of hope for future human trials. If successful, this could be a game-changer, particularly for high-risk populations like healthcare workers and injection drug users.
Another avenue of research focuses on therapeutic vaccines designed to treat chronic hepatitis C rather than prevent it. These vaccines aim to boost the immune system’s ability to clear the virus in individuals already infected. For instance, a peptide-based vaccine, currently in Phase II trials, targets specific HCV proteins to activate T-cell responses. Participants receive three doses over 12 weeks, with preliminary data suggesting improved viral control in some cases. While not a cure, this approach could reduce the need for costly antiviral treatments and improve long-term outcomes for patients.
Comparatively, some trials are investigating combination strategies, pairing vaccines with direct-acting antivirals (DAAs) to enhance efficacy. A recent study tested a prime-boost regimen—an initial DNA vaccine followed by a modified vaccinia Ankara (MVA) vector—in conjunction with DAAs. Results showed a higher sustained virologic response (SVR) rate in the combination group compared to DAAs alone. This hybrid approach underscores the potential of vaccines not as standalone solutions but as complementary tools in the fight against HCV.
Practical challenges remain, however. HCV’s high mutation rate complicates vaccine development, as the virus can evade immune responses. Researchers are addressing this by targeting conserved regions of the virus or developing multivalent vaccines that cover multiple HCV genotypes. Additionally, ensuring accessibility in low-resource settings will be critical, as these regions bear a disproportionate burden of HCV infection. Trials are increasingly focusing on cost-effective formulations and scalable manufacturing processes to bridge this gap.
For those interested in participating in trials, resources like ClinicalTrials.gov provide up-to-date information on ongoing studies, including eligibility criteria and locations. Volunteers typically undergo screening to assess their health status and HCV history, with some trials targeting specific age groups (e.g., 18–65 years) or infection stages. While participation carries risks, it offers a chance to contribute to groundbreaking science and potentially benefit from experimental treatments. As research accelerates, the dream of a hepatitis C vaccine moves closer to reality, fueled by innovation and collaboration across the scientific community.
Global Hotspots: Regions with Highest Non-Vaccination Rates Revealed
You may want to see also
Explore related products




![]()
High-Risk Groups and Protection
Currently, there is no vaccine available for hepatitis C, a fact that underscores the critical importance of identifying and protecting high-risk groups. Unlike hepatitis A and B, which have effective vaccines, hepatitis C prevention relies heavily on behavioral changes and targeted interventions. High-risk groups include individuals who inject drugs, healthcare workers exposed to contaminated blood, people with multiple sexual partners, and those who received blood transfusions or organ transplants before 1992. Understanding these groups is the first step in mitigating the spread of the virus.
For individuals who inject drugs, harm reduction programs are a cornerstone of protection. Needle and syringe exchange programs (NSPs) provide sterile equipment, reducing the risk of transmission through shared needles. These programs often include education on safer injection practices and access to testing and treatment. Studies show that communities with robust NSPs experience significantly lower rates of hepatitis C. Additionally, medication-assisted treatment (MAT) for opioid use disorder, such as methadone or buprenorphine, can reduce injection frequency and further lower transmission risk.
Healthcare workers face a unique set of risks due to occupational exposure to bloodborne pathogens. The Occupational Safety and Health Administration (OSHA) mandates the use of universal precautions, including gloves, masks, and eye protection, to minimize exposure. Post-exposure prophylaxis (PEP) with antiviral medications may be considered if a needle stick injury occurs, though its effectiveness for hepatitis C is less established than for HIV. Regular training and adherence to safety protocols are essential to protect this high-risk group.
Sexual transmission of hepatitis C is less common but remains a concern, particularly among individuals with multiple partners or those in serodiscordant relationships (where one partner has hepatitis C and the other does not). Consistent condom use is recommended for those at risk, though it does not eliminate the risk entirely. For serodiscordant couples, antiviral treatment for the infected partner can reduce the viral load to undetectable levels, significantly lowering the risk of transmission. Testing and early treatment are key strategies for protecting this group.
Finally, individuals who received blood transfusions or organ transplants before 1992 are at higher risk due to the lack of widespread hepatitis C screening during that period. While screening of blood products has since improved, those with a history of transfusions should be tested for hepatitis C. Early detection allows for timely treatment with direct-acting antivirals (DAAs), which cure over 95% of cases within 8–12 weeks. Public health initiatives should focus on outreach to this group, ensuring they are aware of their risk and the availability of effective treatment.
In the absence of a vaccine, protecting high-risk groups requires a multifaceted approach tailored to their specific vulnerabilities. From harm reduction programs for people who inject drugs to occupational safety measures for healthcare workers, each strategy plays a vital role in preventing the spread of hepatitis C. By addressing these groups with targeted interventions, we can significantly reduce the burden of this disease until a vaccine becomes available.
Is the Tetanus Shot a Live Virus? Unraveling the Facts
You may want to see also
Frequently asked questions
No, there is currently no vaccine available to prevent Hepatitis C.
Developing a Hepatitis C vaccine is challenging due to the virus’s ability to mutate rapidly, making it difficult for the immune system to recognize and combat it effectively.
No, other vaccines like those for Hepatitis A or B do not provide protection against Hepatitis C, as they target different viruses.
Yes, researchers are actively working on developing a Hepatitis C vaccine, and several candidates are in clinical trials, but none have been approved yet.
Prevention involves avoiding exposure to infected blood, using sterile needles, practicing safe sex, and not sharing personal items like razors or toothbrushes.