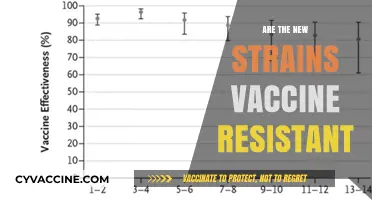
The question of whether mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna for COVID-19, qualify as gene therapy has sparked considerable debate. While both mRNA vaccines and gene therapy involve the use of genetic material, their mechanisms and purposes differ significantly. mRNA vaccines deliver messenger RNA into cells to temporarily instruct them to produce a harmless viral protein, triggering an immune response without altering the recipient’s DNA. In contrast, gene therapy aims to modify or replace faulty genes within a person’s DNA to treat or cure genetic disorders. Since mRNA vaccines do not integrate into the genome or permanently change genetic material, they are not classified as gene therapy by scientific and regulatory standards. This distinction is crucial for understanding their safety, efficacy, and intended use in medical applications.
| Characteristics | Values |
|---|---|
| Definition of Gene Therapy | Gene therapy involves introducing, removing, or altering genetic material (DNA) within a person's cells to treat or prevent disease. It typically targets the genome to correct mutations or introduce new genes. |
| Mechanism of mRNA Vaccines | mRNA vaccines deliver messenger RNA (not DNA) into cells, which temporarily instructs cells to produce a specific protein (e.g., the SARS-CoV-2 spike protein) to trigger an immune response. The mRNA does not alter the host's DNA. |
| Integration into Genome | mRNA vaccines do not integrate into the host's genome. The mRNA is degraded after protein production. |
| Permanence of Effect | The effects of mRNA vaccines are temporary, as the mRNA is broken down within days to weeks. Gene therapy often aims for long-term or permanent genetic modification. |
| Target of Modification | Gene therapy targets DNA, while mRNA vaccines target transient protein production without altering DNA. |
| Regulatory Classification | mRNA vaccines are classified as vaccines by regulatory agencies (e.g., FDA, EMA), not as gene therapy products. |
| Purpose | mRNA vaccines are prophylactic (preventive) tools against infectious diseases. Gene therapy is therapeutic, aiming to treat genetic disorders or diseases. |
| Scientific Consensus | The scientific and medical communities widely agree that mRNA vaccines are not gene therapy due to their mechanism and lack of genomic integration. |
| Examples | mRNA vaccines: Pfizer-BioNTech, Moderna COVID-19 vaccines. Gene therapy: CAR-T cell therapy, Zolgensma for spinal muscular atrophy. |
| Public Misconception | Misinformation has led some to incorrectly label mRNA vaccines as gene therapy, despite clear scientific distinctions. |
Explore related products






What You'll Learn
- mRNA vs. DNA vaccines: Key differences in mechanism and genetic impact
- Do mRNA vaccines alter human DNA or genetic material?
- Temporary vs. permanent effects: How long does mRNA stay in cells
- Regulatory classifications: Are mRNA vaccines considered gene therapy by agencies
- Ethical concerns: Public perception of mRNA vaccines as gene therapy
![]()
mRNA vs. DNA vaccines: Key differences in mechanism and genetic impact
The debate over whether mRNA vaccines constitute gene therapy hinges on understanding their mechanism and genetic impact, particularly when compared to DNA vaccines. Unlike DNA vaccines, which introduce a plasmid encoding the antigen directly into the cell nucleus, mRNA vaccines deliver a transient genetic blueprint that never enters the nucleus. This fundamental difference shapes their safety profiles, efficacy, and potential long-term effects. mRNA vaccines, such as Pfizer-BioNTech and Moderna’s COVID-19 shots, use lipid nanoparticles to ferry mRNA into the cytoplasm, where ribosomes translate it into proteins. DNA vaccines, still largely experimental, require nuclear entry and integration, raising concerns about genomic insertion and mutagenesis. This distinction is critical for addressing public skepticism and regulatory scrutiny.
Consider the practical implications of dosage and administration. mRNA vaccines typically require lower doses (30 µg for Pfizer, 100 µg for Moderna) compared to DNA vaccines, which often need higher quantities to elicit a robust immune response. mRNA’s ephemeral nature—it degrades within days—limits its genetic impact, whereas DNA vaccines’ persistence in cells poses theoretical risks of altering host DNA. For instance, mRNA vaccines are approved for individuals aged 5 and older, while DNA vaccines remain in clinical trials, often targeting specific age groups like adults aged 18–55. This highlights mRNA’s versatility and safety, making it a preferred choice for rapid deployment during pandemics.
From a persuasive standpoint, mRNA vaccines offer a safer genetic intervention compared to DNA-based approaches. Their inability to integrate into the host genome eliminates the risk of insertional mutagenesis, a concern with DNA vaccines. mRNA’s transient presence ensures that any off-target effects are short-lived, whereas DNA vaccines’ prolonged activity could lead to unintended consequences. For example, a DNA vaccine encoding a viral protein might inadvertently disrupt cellular processes if misexpressed. mRNA vaccines, by contrast, are designed to degrade quickly, minimizing such risks. This makes mRNA technology not only a breakthrough in vaccinology but also a benchmark for ethical genetic interventions.
A comparative analysis reveals that while both platforms aim to induce immunity by expressing antigens, their routes and risks diverge. mRNA vaccines act like ephemeral instructions, quickly discarded after protein synthesis, whereas DNA vaccines leave a more permanent mark by relying on cellular machinery for prolonged expression. This difference is akin to writing in pencil versus ink—mRNA’s effects are erasable, while DNA’s are not. For parents hesitant about vaccinating their children, understanding this analogy can alleviate fears of genetic modification. mRNA vaccines do not alter DNA; they merely borrow the cell’s resources temporarily, much like a recipe used once and discarded.
In conclusion, the key differences between mRNA and DNA vaccines lie in their mechanisms and genetic footprints. mRNA vaccines offer a transient, non-integrative approach, making them safer and more efficient for widespread use. DNA vaccines, while promising, carry theoretical risks that necessitate further research. For healthcare providers and policymakers, emphasizing these distinctions can build trust and clarify misconceptions about mRNA vaccines being gene therapy. Practical tips include explaining mRNA’s short-lived nature and highlighting its absence from the nucleus, ensuring patients understand that their DNA remains unchanged. This clarity is essential for informed decision-making in an era of genetic innovation.
Varicella Vaccines: WI-38 Free Options
You may want to see also
Explore related products





![]()
Do mRNA vaccines alter human DNA or genetic material?
MRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna for COVID-19, operate on a fundamentally different mechanism than gene therapy. Gene therapy involves the direct modification of a person’s DNA to treat or prevent disease, often by inserting, deleting, or replacing genetic material. In contrast, mRNA vaccines deliver genetic instructions (messenger RNA) that temporarily prompt cells to produce a harmless protein, mimicking a viral component, to trigger an immune response. This process does not involve interaction with the cell’s nucleus, where DNA resides, and the mRNA itself is rapidly degraded by the body after fulfilling its role.
To understand why mRNA vaccines cannot alter human DNA, consider the cellular biology involved. DNA is housed within the nucleus, a highly protected compartment of the cell. mRNA vaccines enter cells in the cytoplasm, where protein synthesis occurs, and never cross the nuclear membrane. The mRNA molecules are designed to be short-lived, breaking down within days after vaccination. For DNA alteration to occur, the mRNA would need to reverse-transcribe into DNA, enter the nucleus, and integrate into the genome—a process that lacks the necessary enzymes and mechanisms in human cells. Scientific studies, including those published in *Nature* and *Cell*, have confirmed no evidence of mRNA vaccine integration into human DNA.
A common misconception arises from the term "genetic material" in mRNA vaccines. While mRNA is indeed genetic material, it is distinct from DNA and serves a different function. mRNA is a transient messenger, carrying instructions from DNA to the ribosomes for protein production. It does not possess the stability or structure to alter the genome. For context, the mRNA in vaccines degrades far more quickly than the weeks or months it would take for hypothetical DNA integration to occur. Regulatory bodies like the FDA and EMA have rigorously evaluated these vaccines, concluding that they do not modify human DNA.
Practical considerations further reinforce this point. mRNA vaccines are administered in specific dosages—30 micrograms for Pfizer and 100 micrograms for Moderna—optimized to elicit an immune response without overwhelming cellular processes. These doses are carefully calibrated to ensure safety and efficacy across age groups, from adolescents (12 and older for Pfizer, 18 and older for Moderna) to elderly populations. Adverse effects, such as myocarditis, are rare and unrelated to DNA alteration. Parents and individuals concerned about genetic changes can refer to CDC and WHO guidelines, which emphasize the vaccines’ inability to interact with DNA.
In summary, mRNA vaccines are not gene therapy and do not alter human DNA. Their mechanism relies on temporary mRNA instructions that remain outside the nucleus, are rapidly cleared from the body, and lack the capacity to integrate into the genome. This distinction is critical for addressing public concerns and fostering trust in vaccine science. Understanding the biology behind these vaccines empowers individuals to make informed decisions, free from misinformation.
Rabies Vaccination: Adult Immunization Requirements and Recommendations
You may want to see also
Explore related products

$3.99 $19.99




![]()
Temporary vs. permanent effects: How long does mRNA stay in cells?
MRNA molecules in vaccines are designed to be transient visitors in our cells, not permanent residents. Once injected, they enter cells and serve as blueprints for producing a harmless piece of the virus's spike protein, triggering an immune response. But how long does this molecular visitor actually stick around?
Studies show that mRNA from vaccines like Pfizer-BioNTech and Moderna degrades rapidly, typically within days to a week. This is by design. The mRNA is encased in lipid nanoparticles, which protect it during delivery but also allow for its quick breakdown once its job is done. Enzymes in our cells, called RNases, swiftly recognize and destroy the mRNA, ensuring it doesn't linger.
This temporary nature is a key distinction from gene therapy, which aims to introduce permanent genetic changes. Gene therapy often uses viral vectors to deliver DNA that integrates into the host genome, potentially altering gene expression long-term. mRNA vaccines, in contrast, never enter the cell nucleus, where our DNA resides. They simply provide a temporary instruction manual for protein production, leaving no lasting mark on our genetic code.
Think of it like a recipe card versus a cookbook. Gene therapy adds a new recipe to your permanent collection, while mRNA vaccines are like a temporary note reminding you how to make a specific dish. Once you've learned the recipe, the note is discarded.
Understanding this temporary nature is crucial for addressing concerns about long-term effects. The rapid degradation of mRNA means it's highly unlikely to cause persistent changes in our bodies. This is why regulatory agencies like the FDA and WHO have confidently approved mRNA vaccines for widespread use, even in vulnerable populations like the elderly and immunocompromised individuals.
CDC Mask Guidelines Post-Vaccination: What You Need to Know
You may want to see also
Explore related products






![]()
Regulatory classifications: Are mRNA vaccines considered gene therapy by agencies?
Regulatory agencies worldwide have grappled with classifying mRNA vaccines, particularly in the context of gene therapy. The U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have both issued guidelines that distinguish mRNA vaccines from traditional gene therapies. While gene therapies typically aim to modify or replace genetic material in target cells to treat or cure diseases, mRNA vaccines function differently. They deliver genetic instructions to cells to produce a specific protein, often a viral antigen, triggering an immune response without altering the host’s DNA. This fundamental difference in mechanism has led regulators to classify mRNA vaccines as vaccines rather than gene therapies.
From a regulatory standpoint, the classification of mRNA vaccines as vaccines rather than gene therapies has practical implications. Vaccines are subject to well-established regulatory pathways, including expedited approval processes during public health emergencies, as seen with COVID-19. Gene therapies, on the other hand, often face more stringent requirements due to their potential for long-term genetic modification. For instance, the FDA’s Center for Biologics Evaluation and Research (CBER) oversees gene therapies, while vaccines fall under the purview of the same center but with distinct regulatory frameworks. This classification ensures that mRNA vaccines can be developed, approved, and distributed more rapidly, a critical factor during pandemics.
A comparative analysis of regulatory definitions highlights the nuances in classification. The EMA defines gene therapy as “the administration of nucleic acids to humans to treat, prevent, or diagnose disease,” but it explicitly excludes vaccines from this category. Similarly, the FDA’s guidance on gene therapy products does not include mRNA vaccines, emphasizing that these vaccines do not integrate into the host genome. This distinction is crucial, as gene therapies often involve viral vectors or other methods to permanently modify DNA, whereas mRNA vaccines are transient and degrade after protein synthesis. Such clarity in regulatory language ensures consistency across jurisdictions and industries.
Practical considerations for healthcare providers and patients arise from this classification. mRNA vaccines, such as Pfizer-BioNTech and Moderna’s COVID-19 vaccines, are administered in specific dosages—typically 30 µg for adults and adjusted for pediatric populations (e.g., 10 µg for children aged 5–11). These vaccines are not considered gene therapy, which means they do not carry the same risks of permanent genetic alteration. Patients with concerns about gene therapy can be reassured that mRNA vaccines are a safe and effective tool for disease prevention. Healthcare providers should emphasize this distinction to build trust and combat misinformation, particularly in vaccine-hesitant populations.
In conclusion, regulatory agencies have consistently classified mRNA vaccines as vaccines, not gene therapies, based on their mechanism of action and lack of permanent genetic modification. This classification facilitates faster approvals, clearer guidelines, and broader public acceptance. Understanding these regulatory distinctions is essential for healthcare professionals, policymakers, and the public to navigate the evolving landscape of biotechnology and vaccination. By focusing on the specifics of mRNA vaccines, stakeholders can make informed decisions and contribute to global health initiatives effectively.
Join the J&J Vaccine Trial: Your Step-by-Step Sign-Up Guide
You may want to see also
Explore related products






![]()
Ethical concerns: Public perception of mRNA vaccines as gene therapy
The public's perception of mRNA vaccines as gene therapy has sparked ethical concerns, particularly around informed consent and trust in medical institutions. When individuals believe mRNA vaccines alter their DNA—a misconception fueled by misinformation—they may feel their autonomy is compromised. This perception can lead to vaccine hesitancy, as seen in surveys where 30% of respondents expressed concern that mRNA vaccines could modify their genetic makeup. Addressing this requires clear communication: mRNA vaccines deliver genetic instructions to cells to produce a harmless protein, triggering an immune response, but they do not integrate into the genome. Clinicians and health communicators must emphasize this distinction, using analogies like “temporary recipe cards” rather than “permanent DNA editors,” to rebuild trust and ensure informed decision-making.
Another ethical concern arises from the historical context of gene therapy trials, which have occasionally resulted in severe adverse events, such as the death of Jesse Gelsinger in 1999. While mRNA vaccines are distinct from traditional gene therapies, public memory of these incidents can blur the lines, fostering fear and skepticism. To counteract this, health campaigns should transparently differentiate mRNA vaccines from gene therapy, highlighting their safety profiles—for instance, the Pfizer-BioNTech and Moderna vaccines underwent rigorous Phase 3 trials involving tens of thousands of participants, with no evidence of genetic alteration. Pairing scientific data with empathetic messaging can help disentangle mRNA vaccines from the shadow of past gene therapy controversies.
The framing of mRNA vaccines as gene therapy also intersects with broader societal debates about biotechnology and corporate influence. Critics argue that labeling mRNA vaccines as gene therapy could be exploited by anti-vaccine groups to stoke fears of “Big Pharma” manipulating human genetics. This narrative can disproportionately affect marginalized communities, who may already face systemic healthcare disparities and historical medical exploitation. Ethical communication strategies must acknowledge these concerns, involving community leaders and culturally tailored messaging to ensure inclusivity. For example, translating materials into multiple languages and addressing specific cultural beliefs can foster trust and reduce the impact of misinformation.
Finally, the ethical challenge extends to policymakers and regulators, who must balance scientific accuracy with public perception. Misclassifying mRNA vaccines as gene therapy could lead to unnecessary regulatory hurdles, delaying access to life-saving treatments. Conversely, dismissing public concerns outright risks alienating those already skeptical of medical innovations. A pragmatic approach involves engaging bioethicists and social scientists to design communication frameworks that respect public fears while correcting inaccuracies. For instance, public forums or town halls where experts address questions directly can demystify mRNA technology and its ethical implications, bridging the gap between scientific consensus and public understanding.
Scarlet Fever Vaccine: Current Status and Prevention Strategies Explained
You may want to see also
Frequently asked questions
No, mRNA vaccines are not gene therapy. They deliver genetic material (mRNA) that instructs cells to produce a harmless protein (like the spike protein of COVID-19), triggering an immune response. This mRNA does not alter or interact with your DNA.
No, mRNA vaccines do not change your genetic code. The mRNA they contain is temporary and degrades quickly after delivering its instructions. It never enters the cell’s nucleus, where DNA is stored.
Yes, there is a significant difference. Gene therapy aims to modify or replace faulty genes in a person’s DNA to treat genetic disorders. mRNA vaccines, on the other hand, use mRNA to produce a specific protein to stimulate immunity, without altering DNA.
The confusion arises because both involve genetic material. However, mRNA vaccines use mRNA to produce proteins temporarily, while gene therapy involves directly modifying or replacing DNA. They serve different purposes and function in distinct ways.