The question of whether more men or women are vaccinated is a critical aspect of public health analysis, as it sheds light on potential gender disparities in vaccine uptake and access. Studies have shown that vaccination rates can vary significantly between genders due to a multitude of factors, including socioeconomic status, cultural norms, healthcare accessibility, and individual health beliefs. For instance, in some regions, women may face barriers to vaccination due to limited mobility or prioritization of family needs, while in others, men might be less likely to seek preventive care. Understanding these differences is essential for tailoring public health strategies to ensure equitable vaccine distribution and improve overall community immunity.
Explore related products


$24.99




What You'll Learn
- Gender disparities in vaccine uptake across different age groups
- Impact of socioeconomic factors on vaccination rates by gender
- Role of healthcare access in gender-based vaccination differences
- Influence of cultural beliefs on men’s and women’s vaccination choices
- Comparison of global vaccination trends between men and women
![]()
Gender disparities in vaccine uptake across different age groups
Vaccination rates often reveal intriguing gender disparities, particularly when examined across different age groups. For instance, in the United States, data from the Centers for Disease Control and Prevention (CDC) shows that women aged 65 and older are more likely to receive influenza vaccines than their male counterparts, with a 7% higher uptake rate. This trend, however, reverses in younger age groups, where men sometimes outpace women in COVID-19 vaccination rates, particularly in the 18–29 age bracket. Such variations underscore the need to explore the underlying factors driving these differences.
To address gender disparities in vaccine uptake, consider age-specific strategies. For older adults, where women lead in vaccination, the success may lie in targeted health messaging that emphasizes preventive care, a domain women historically engage with more frequently. Conversely, for younger age groups, where men occasionally show higher uptake, leveraging peer influence and digital platforms could be key. For example, social media campaigns featuring male influencers discussing vaccine benefits have shown promise in engaging hesitant young men. Tailoring approaches to age and gender can bridge gaps effectively.
A comparative analysis reveals that cultural norms and health-seeking behaviors play a significant role in these disparities. In many societies, women are often the primary caregivers, making them more likely to prioritize health interventions for themselves and their families. This could explain their higher vaccination rates in older age groups. In contrast, younger men may face societal pressures to appear invulnerable, leading to vaccine hesitancy. Understanding these dynamics is crucial for designing interventions that resonate with specific demographics.
Practical tips for improving vaccine uptake across genders and age groups include offering flexible vaccination hours to accommodate work schedules, particularly for younger adults. For older populations, integrating vaccine services into routine health check-ups can increase convenience. Additionally, addressing misinformation through trusted sources, such as local healthcare providers, can alleviate concerns. For instance, a study in the UK found that personalized text reminders increased vaccination rates by 15% among 30–49-year-olds, regardless of gender.
In conclusion, gender disparities in vaccine uptake are not uniform across age groups, requiring nuanced approaches to address them. By combining data-driven insights with tailored strategies, public health initiatives can effectively close these gaps. Whether through targeted messaging, cultural sensitivity, or practical solutions, the goal remains clear: ensure equitable access to vaccines for all, regardless of age or gender.
The Evolution of Meningitis Vaccination: A Historical Overview
You may want to see also
Explore related products

$39.89 $52.95



$124.98 $132


![]()
Impact of socioeconomic factors on vaccination rates by gender
Socioeconomic factors significantly influence vaccination rates, often creating disparities between men and women. For instance, in low-income regions, women frequently face barriers such as limited access to healthcare facilities, lower health literacy, and cultural norms that prioritize male family members for medical resources. A 2021 study in sub-Saharan Africa revealed that women were 15% less likely than men to receive COVID-19 vaccines, partly due to these systemic challenges. Conversely, in high-income countries, women often exhibit higher vaccination rates, attributed to greater engagement with preventive healthcare services, such as routine check-ups and screenings, which include vaccine administration.
Analyzing education levels provides further insight into this gender gap. Women with higher education are more likely to be vaccinated across all age groups, as education correlates with better health awareness and access to information. For example, in the United States, college-educated women aged 25–40 had a 20% higher COVID-19 vaccination rate compared to their male counterparts. However, among less educated populations, men sometimes surpass women in vaccination rates, particularly in occupations requiring mandatory immunizations, such as construction or transportation. This highlights how socioeconomic roles and workplace policies intersect with gender to shape health behaviors.
Income inequality also plays a critical role in vaccination disparities. In middle-income countries like India, women from lower socioeconomic strata often forgo vaccines due to financial constraints or lack of autonomy in household decision-making. For instance, a 2022 survey found that only 45% of women in rural areas received full doses of the COVID-19 vaccine, compared to 60% of men. Practical solutions include targeted subsidies, mobile vaccination clinics, and community-based education campaigns to address these gaps. Policymakers must consider gender-specific barriers when designing interventions to ensure equitable vaccine distribution.
Cultural and societal norms further exacerbate these disparities. In patriarchal societies, women’s health needs are often deprioritized, leading to lower vaccination rates. For example, in parts of the Middle East, women require male consent for medical procedures, including vaccinations, which delays or prevents access. Conversely, in Western societies, where gender equality is more pronounced, women consistently outpace men in vaccination uptake. Addressing these norms requires not only policy changes but also community engagement to shift perceptions about gender roles and health priorities.
To bridge the gender gap in vaccination rates, tailored strategies are essential. For women in low-income settings, initiatives like door-to-door vaccination drives, female health workers, and flexible clinic hours can improve access. In high-income regions, campaigns targeting vaccine-hesitant men, such as workplace immunization programs or male-focused health fairs, could boost participation. Ultimately, understanding the interplay of socioeconomic factors with gender is crucial for designing effective, equitable vaccination programs that leave no one behind.
Skipping a Vaccine Round: Risks, Consequences, and What You Need to Know
You may want to see also
Explore related products






![]()
Role of healthcare access in gender-based vaccination differences
Healthcare access disparities significantly influence gender-based vaccination differences, often tipping the scales in favor of one gender over the other. In regions where women face barriers to healthcare—such as limited mobility, cultural restrictions, or financial constraints—vaccination rates among women tend to lag. For instance, in rural areas of India, women’s vaccination rates for COVID-19 were initially lower than men’s due to reduced access to clinics and lower health literacy. Conversely, in some Western countries, women often have higher vaccination rates because they are more likely to engage with preventive healthcare services, such as routine check-ups or prenatal care, which include vaccination opportunities.
Consider the practical steps needed to address these disparities. In low-resource settings, mobile vaccination clinics can bridge the gap by bringing vaccines directly to underserved communities, particularly targeting women who may lack transportation or face time constraints due to caregiving responsibilities. For example, during the Ebola vaccine rollout in the Democratic Republic of Congo, door-to-door campaigns ensured women in remote areas received doses. Additionally, integrating vaccination services into existing women’s health programs, such as maternal health clinics, can increase uptake. For men, who often underutilize preventive care, workplace vaccination drives or partnerships with sports clubs can be effective strategies.
A comparative analysis reveals that gender norms also play a role in healthcare access and vaccination. In societies where men are expected to avoid showing vulnerability, they may delay or refuse vaccines due to perceived stigma. For instance, in the U.S., studies show men are less likely to seek medical care, contributing to lower vaccination rates for diseases like influenza or HPV. Women, on the other hand, may face barriers in patriarchal cultures where their health decisions are controlled by male family members. Addressing these norms requires targeted education campaigns that challenge stereotypes and emphasize vaccination as a collective responsibility rather than a gendered choice.
Finally, data-driven policies are essential to closing the gender gap in vaccination. Governments and health organizations must collect and analyze gender-disaggregated data to identify specific barriers and tailor interventions. For example, in Brazil, health officials used such data to implement a campaign targeting men for COVID-19 vaccines, highlighting their role in protecting families. Similarly, in sub-Saharan Africa, programs that involve female community health workers have successfully increased vaccination rates among women by addressing cultural and logistical barriers. By focusing on equitable healthcare access, societies can ensure that vaccination efforts reach all genders effectively, regardless of systemic or cultural obstacles.
Understanding the Abbreviation for Polio Vaccine: A Quick Guide
You may want to see also
Explore related products






![]()
Influence of cultural beliefs on men’s and women’s vaccination choices
Cultural beliefs significantly shape vaccination choices, often leading to disparities between men and women. In many societies, traditional gender roles influence health-seeking behaviors, with women frequently taking on the role of family caregivers and thus being more proactive about preventive measures like vaccination. For instance, in a study across several low-income countries, women were found to be 10% more likely than men to receive vaccines, partly due to maternal health programs that prioritize female immunization. This trend highlights how cultural expectations of women as guardians of family health can drive higher vaccination rates among them.
However, cultural norms can also create barriers for women in certain contexts. In some conservative communities, women’s mobility and decision-making autonomy are restricted, limiting their access to vaccination services. For example, in parts of rural India and Pakistan, cultural taboos around women traveling alone or interacting with male healthcare workers have resulted in lower vaccination rates among women, despite their willingness to get vaccinated. Conversely, men in these regions may face societal pressure to avoid appearing weak or fearful, leading to vaccine hesitancy. A survey in Brazil revealed that 30% of unvaccinated men cited fear of side effects as a reason, compared to 20% of women, suggesting that cultural expectations of masculinity may discourage men from seeking preventive care.
The influence of cultural beliefs is further evident in age-specific vaccination trends. Among older adults, cultural attitudes toward aging and health often differ by gender. In Japan, for example, women over 65 are 15% more likely than men to receive flu and pneumonia vaccines, possibly because Japanese culture encourages older women to prioritize health maintenance. In contrast, younger men in Western countries, particularly those aged 18–30, exhibit higher vaccine hesitancy rates, with 25% expressing skepticism compared to 18% of women. This disparity may stem from cultural narratives that associate risk-taking with masculinity, making young men less likely to engage in preventive behaviors.
Practical strategies to address these cultural influences must be tailored to specific demographics. For women in restrictive cultures, mobile vaccination clinics and female-led health teams can improve access. In regions where men are hesitant, campaigns featuring male role models or emphasizing vaccines as a way to protect family and community can be effective. For instance, a Kenyan initiative that engaged local male leaders in promoting HPV vaccination increased uptake by 20%. Additionally, age-specific messaging—such as framing vaccines as a way to maintain independence for older adults or as a social responsibility for younger individuals—can resonate more deeply with cultural values.
Ultimately, understanding the interplay between cultural beliefs and gender is crucial for designing equitable vaccination programs. By acknowledging how societal expectations shape health behaviors, policymakers and healthcare providers can create interventions that respect cultural norms while encouraging vaccination for all. For example, offering flexible vaccination schedules for working men or integrating vaccine education into women’s community groups can address specific barriers. Such targeted approaches not only bridge the gender gap in vaccination rates but also foster a culture of health that benefits entire communities.
Legal Options for Declining Vaccines in Florida: A Comprehensive Guide
You may want to see also
Explore related products






![]()
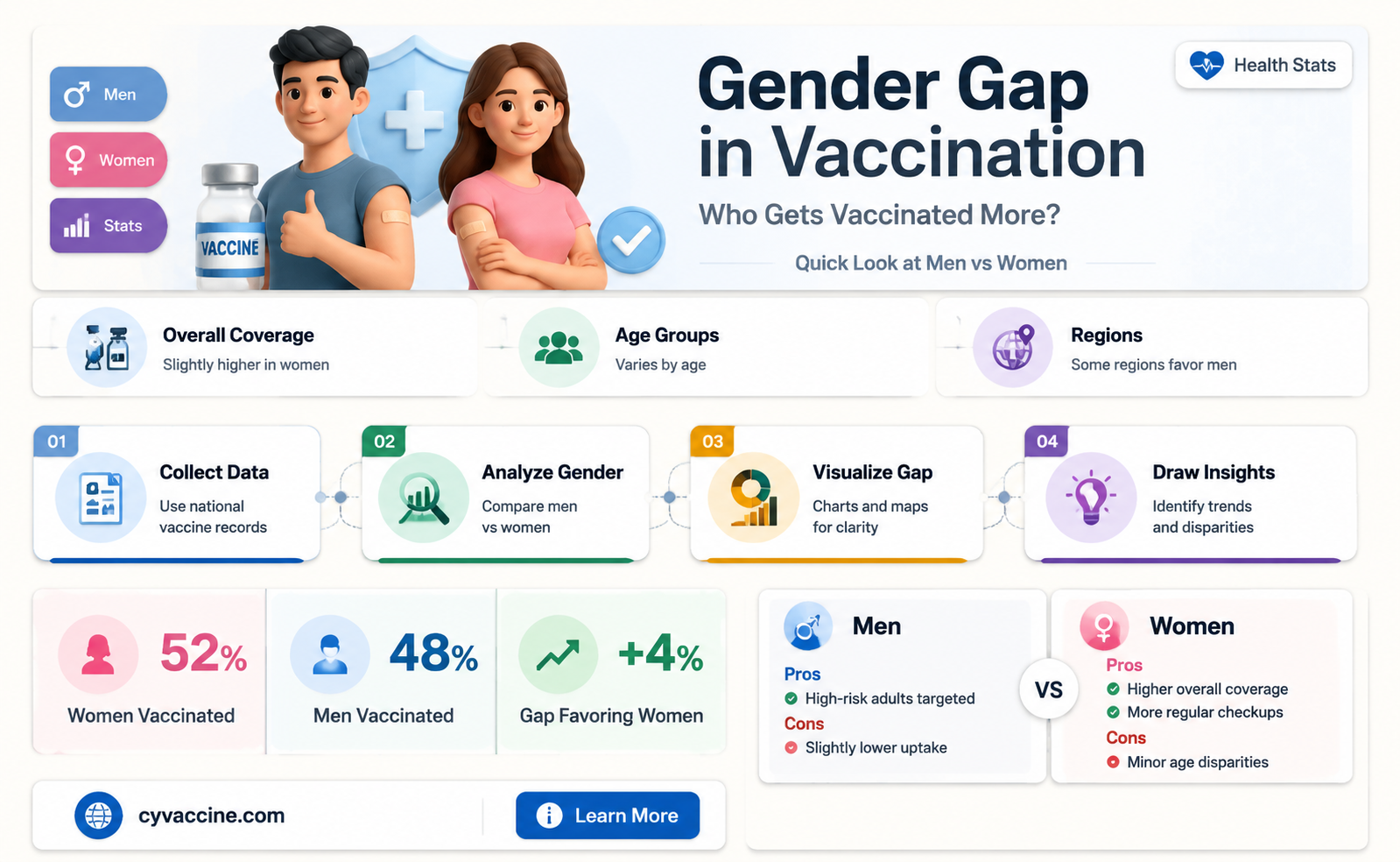
Comparison of global vaccination trends between men and women
Global vaccination data reveals a persistent gap between men and women, with women consistently showing higher vaccination rates across various age groups and regions. This trend is particularly evident in routine immunizations, such as influenza and COVID-19 vaccines. For instance, during the COVID-19 pandemic, countries like the United States and the United Kingdom reported that women were 5-10% more likely to receive both doses of the vaccine compared to men. This disparity raises questions about the underlying factors driving these differences and their implications for public health strategies.
Analyzing the reasons behind this gap highlights several key factors. Women generally exhibit higher health-seeking behavior, often prioritizing preventive care and regular check-ups. Additionally, societal roles, such as women being primary caregivers, may increase their exposure to health information and vaccination campaigns. Conversely, men often face societal pressures to appear invulnerable, leading to vaccine hesitancy or avoidance. For example, studies show that men are more likely to cite concerns about vaccine side effects or question their efficacy, contributing to lower uptake rates.
To address this imbalance, targeted interventions are essential. Public health campaigns should focus on educating men about the benefits of vaccination, using male-centric messaging and role models to encourage participation. For instance, sports figures or community leaders could be enlisted to promote vaccine confidence among men. Simultaneously, efforts should ensure that women’s higher vaccination rates are sustained, particularly in regions where access to healthcare remains a challenge. Practical steps include offering flexible vaccination hours, integrating vaccine services with maternal and child health programs, and leveraging digital platforms to reach diverse populations.
A comparative analysis of high- and low-income countries further underscores the complexity of this issue. In wealthier nations, the gender gap in vaccination is often more pronounced due to greater access to healthcare and stronger health systems, which amplify behavioral differences. In contrast, low-income countries may see smaller gaps or even reversed trends due to limited access and gender disparities in healthcare utilization. For example, in some African nations, men have been reported to receive vaccines at higher rates due to occupational requirements or targeted campaigns in male-dominated industries.
In conclusion, the comparison of global vaccination trends between men and women highlights a multifaceted issue shaped by behavioral, societal, and systemic factors. Bridging this gap requires tailored strategies that address gender-specific barriers while ensuring equitable access for all. By understanding these dynamics, policymakers and healthcare providers can design more effective vaccination programs that improve overall public health outcomes.
Polio Vaccine Breakthrough: A Historical Turning Point in Eradicating the Disease
You may want to see also
Frequently asked questions
Data varies by region, but globally, women tend to have slightly higher vaccination rates than men, particularly for COVID-19 vaccines.
Differences can stem from factors like healthcare access, occupational roles, and societal norms influencing health-seeking behaviors.
Yes, disparities can vary by age group, with women often having higher rates in older populations and men catching up in younger demographics.
Yes, some countries report higher male vaccination rates due to factors like workforce participation, vaccine mandates, or cultural attitudes toward health.



![International Certificate of Vaccination with Vinyl Document Holder - World Health Organization Bilingual Version [cards] World Health Organization [Jan 01, 2007]](https://m.media-amazon.com/images/I/61SHjBP1VYL._AC_UL320_.jpg)