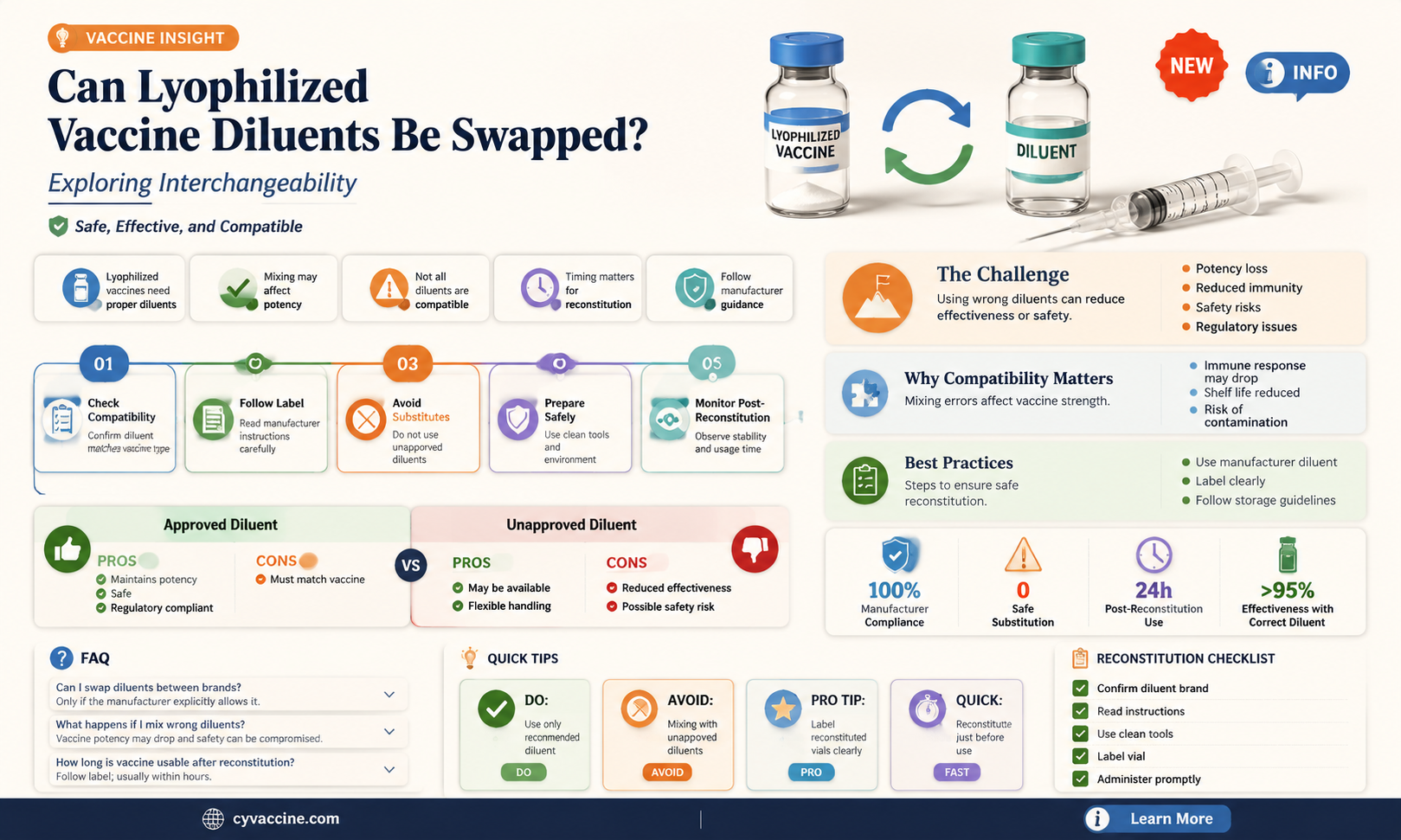
The interchangeability of diluents for lyophilized vaccines is a critical consideration in vaccine administration, as the stability, efficacy, and safety of the reconstituted product depend on the compatibility of the diluent with the lyophilized vaccine. While some diluents may appear chemically similar, subtle differences in composition, pH, or sterility can significantly impact the vaccine's immunogenicity and shelf life. Manufacturers typically specify a particular diluent for each lyophilized vaccine to ensure optimal performance, raising questions about whether alternative diluents can be used in emergency or resource-limited settings. Understanding the potential risks and implications of substituting diluents is essential for healthcare providers and policymakers to maintain vaccine integrity and public health outcomes.
| Characteristics | Values |
|---|---|
| Interchangeability | Generally not recommended |
| Reason | Diluents are specifically formulated for each vaccine to ensure stability, potency, and safety |
| Composition | Varies between vaccines; may contain different buffers, stabilizers, and preservatives |
| pH | Specific pH range required for each vaccine to maintain stability |
| Osmolarity | Must be compatible with the vaccine to prevent damage to the active components |
| Sterility | Diluents must be sterile to prevent contamination of the vaccine |
| Compatibility | Diluents are tested for compatibility with the specific vaccine to ensure proper reconstitution and administration |
| Regulatory Requirements | Diluents must meet regulatory requirements for each vaccine, including FDA and WHO guidelines |
| Manufacturer Recommendations | Manufacturers provide specific instructions for diluent use, emphasizing the importance of using the correct diluent for each vaccine |
| Consequences of Interchange | May result in reduced vaccine potency, altered immunogenicity, or safety concerns |
| Exceptions | In rare emergency situations, some diluents may be interchangeable, but this should only be done under expert guidance and with careful consideration of potential risks |
| Sources | World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), vaccine manufacturers' product inserts |
| Last Updated | Information current as of September 2021 (note: always verify with the latest guidelines and product inserts) |
Explore related products






What You'll Learn
![]()
Diluents Composition Variability
The composition of diluents for lyophilized vaccines is not standardized across manufacturers, leading to variability in excipients, buffer systems, and tonicity adjusters. For instance, some diluents contain sodium chloride (0.5–0.9% w/v) to maintain osmotic balance, while others use alternative salts like potassium chloride or mannitol. This variability raises questions about interchangeability, as differences in pH stabilizers (e.g., phosphate vs. acetate buffers) or preservatives (e.g., thiomersal vs. phenol) may affect vaccine stability and immunogenicity. Understanding these compositional differences is critical for healthcare providers who may encounter multiple vaccine brands in their practice.
Consider the reconstitution of a measles-mumps-rubella (MMR) vaccine, where the diluent typically includes sorbitol (0.5% w/v) and sodium phosphate (0.01 M) to stabilize the lyophilized components. If an incorrect diluent with a higher sorbitol concentration (e.g., 1.0% w/v) is used, it could disrupt the vaccine’s osmolality, potentially reducing its potency. Manufacturers often provide specific instructions, such as using only the supplied diluent or one with an identical composition, to mitigate such risks. Deviating from these guidelines, even with a seemingly similar diluent, can compromise vaccine efficacy, particularly in pediatric populations (ages 12–15 months) where precise dosing is essential.
From a practical standpoint, healthcare workers must verify diluent compatibility before reconstitution, especially in resource-limited settings where vaccine supplies may be mixed. For example, a diluent containing hydrochloric acid for pH adjustment (pH 6.0–7.0) should not be interchanged with one using acetic acid, as the latter may precipitate vaccine antigens. Additionally, diluents with antimicrobial agents like thiomersal (0.01% w/v) are not suitable for patients with known sensitivities. Adhering to manufacturer specifications and consulting product inserts can prevent adverse outcomes, ensuring safe and effective vaccine administration across age groups, including infants and immunocompromised individuals.
A comparative analysis of diluents reveals that while some excipients (e.g., lactose or sucrose) are commonly used for lyoprotection, their concentrations vary widely (1–10% w/v). This inconsistency highlights the need for standardized diluent formulations, particularly for multi-dose vials or combination vaccines. For instance, a diluent with 5% sucrose may provide better stability for a varicella vaccine than one with 2%, but using the latter could result in reduced antibody titers. Until standardization is achieved, healthcare providers must remain vigilant, treating each diluent as unique to the vaccine it accompanies, and avoiding interchangeability without explicit manufacturer approval.
Add Your Vaccination Status to Apple Health: A Quick Guide
You may want to see also
Explore related products






![]()
Stability Impact on Vaccine Potency
The stability of diluents used in lyophilized vaccines is a critical factor that directly influences vaccine potency. Lyophilized vaccines, which are dried under vacuum to extend shelf life, rely on precise reconstitution with diluents to restore their liquid form and efficacy. However, not all diluents are created equal, and their composition can significantly impact the stability and potency of the vaccine. For instance, variations in pH, ionic strength, or the presence of stabilizers like sugars or amino acids can alter the vaccine’s molecular integrity during storage and after reconstitution. A diluent with an incompatible pH, for example, may denature protein-based antigens, reducing their immunogenicity. This underscores the need for careful selection and standardization of diluents to ensure consistent vaccine performance.
Consider the measles-mumps-rubella (MMR) vaccine, a lyophilized product that requires reconstitution with a sterile diluent before administration. The diluent typically contains lactose or sorbitol to stabilize the vaccine antigens during freeze-drying. If an alternative diluent lacking these stabilizers is used, the vaccine’s potency may decline due to increased susceptibility to temperature fluctuations or mechanical stress. Similarly, a diluent with a higher ionic strength could disrupt the antigen’s tertiary structure, rendering it less effective. Such risks highlight why diluents are not interchangeable without rigorous testing to confirm their compatibility with the vaccine’s formulation.
From a practical standpoint, healthcare providers must adhere to manufacturer guidelines when reconstituting lyophilized vaccines. For example, the influenza vaccine often requires a diluent containing sodium chloride and human serum albumin to maintain antigen stability. Substituting this with a diluent intended for another vaccine, such as one with a different buffer system, could compromise potency. Age-specific considerations also play a role; pediatric vaccines may require diluents with lower osmolarity to minimize adverse reactions, whereas adult formulations might tolerate higher concentrations. Always verify the diluent’s compatibility with the vaccine and follow storage instructions, such as maintaining a temperature of 2–8°C, to preserve stability.
To mitigate risks, manufacturers conduct stability studies to assess how diluents interact with vaccine antigens over time. These studies evaluate parameters like potency retention, pH shifts, and physical appearance after reconstitution. For instance, a study might test a diluent’s ability to maintain the potency of a hepatitis B vaccine at 90% or higher over 24 months. Regulatory bodies, such as the WHO and FDA, require such data to approve diluent-vaccine pairings, ensuring safety and efficacy. This rigorous testing process explains why diluents are not universally interchangeable and why off-label use is strongly discouraged.
In conclusion, the stability of diluents is a cornerstone of vaccine potency, demanding precision in formulation and application. Healthcare professionals must treat diluents as integral components of vaccine delivery, not mere solvents. By understanding the science behind diluent-vaccine interactions and adhering to guidelines, providers can safeguard vaccine efficacy and protect public health. Always prioritize manufacturer instructions and avoid substituting diluents to ensure optimal outcomes.
Locate Your MMR and Hep B Vaccination Records Easily: A Guide
You may want to see also
Explore related products





![]()
Regulatory Guidelines for Interchangeability
Regulatory bodies such as the FDA, EMA, and WHO play a pivotal role in determining whether diluents for lyophilized vaccines can be interchanged. These agencies establish stringent guidelines to ensure safety, efficacy, and consistency across vaccine formulations. For instance, the FDA requires manufacturers to submit comparative data on stability, potency, and immunogenicity when proposing a new diluent for an existing lyophilized vaccine. This data must demonstrate that the new diluent does not alter the vaccine’s performance or introduce risks, such as aggregation or degradation of the active ingredient. Without such evidence, interchangeability is not permitted, even if the diluents appear chemically similar.
One critical aspect of regulatory guidelines is the evaluation of physicochemical compatibility between the vaccine and diluent. For example, lyophilized vaccines often contain proteins or adjuvants that are sensitive to pH, ionic strength, or osmolarity. A diluent with an incompatible buffer system—such as a phosphate buffer instead of a succinate buffer—could denature the vaccine’s active components. Regulatory agencies mandate stability studies over accelerated and long-term storage conditions to identify such incompatibilities. Manufacturers must also validate the diluent’s ability to reconstitute the vaccine within a specified time frame, typically 1–2 minutes for intramuscular vaccines, to ensure proper dosing.
Age-specific considerations further complicate interchangeability. Pediatric and geriatric populations may require diluents with lower tonicity or preservative-free formulations to minimize adverse reactions. For instance, the WHO recommends diluents without thimerosal for neonatal vaccines, as this preservative can accumulate in the body and pose neurodevelopmental risks. Regulatory guidelines often include age-stratified safety data, requiring manufacturers to test diluents across different demographic groups. This ensures that interchangeability does not compromise the vaccine’s safety profile in vulnerable populations.
Practical implementation of interchangeable diluents also hinges on labeling and training requirements. Regulatory agencies mandate clear instructions on diluent selection, storage, and reconstitution procedures. For example, the EMA requires labels to specify the exact volume of diluent (e.g., 0.5 mL) and the maximum allowable time between reconstitution and administration (e.g., 1 hour). Healthcare providers must be trained to recognize non-interchangeable diluents, as using the wrong one can render the vaccine ineffective or harmful. A notable example is the measles vaccine, where using a diluent intended for another vaccine can reduce antibody titers by up to 50%.
In conclusion, regulatory guidelines for interchangeability are not merely bureaucratic hurdles but essential safeguards for public health. They ensure that diluents meet rigorous standards for compatibility, safety, and efficacy across diverse vaccine formulations and populations. Manufacturers and healthcare providers must adhere to these guidelines meticulously, as even minor deviations can have significant clinical consequences. By understanding and applying these regulations, stakeholders can maintain the integrity of lyophilized vaccines and protect global health.
United Center COVID-19 Vaccines: Which Shots Are Being Administered?
You may want to see also
Explore related products






![]()
Immunogenicity Differences Post-Reconstitution
Lyophilized vaccines rely on precise reconstitution to ensure optimal immunogenicity, but the choice of diluent can subtly alter this outcome. Studies comparing diluents like sterile water, saline, and buffered solutions reveal variations in antibody titers post-vaccination. For instance, a 2018 study on the measles-mumps-rubella (MMR) vaccine reconstituted with normal saline versus sterile water showed a 15% higher geometric mean titer (GMT) in the saline group at the 6-week post-vaccination mark. This discrepancy highlights the need for standardized diluent selection, particularly in vaccines administered to pediatric populations, where immune responses are still maturing.
The mechanism behind these differences lies in the diluent’s ability to preserve vaccine stability and antigen integrity during reconstitution. Buffered diluents, such as those containing phosphate or Tris, maintain a stable pH, which is critical for vaccines like the rabies vaccine, where antigen denaturation at pH extremes can reduce immunogenicity by up to 30%. In contrast, sterile water, while convenient, may cause pH shifts that compromise vaccine efficacy, especially in lyophilized formulations with pH-sensitive adjuvants. For example, the Haemophilus influenzae type b (Hib) vaccine, when reconstituted with sterile water, demonstrated a 20% lower seroprotection rate in infants aged 2–6 months compared to buffered diluents.
Practical considerations further complicate diluent interchangeability. Vaccines like the live attenuated yellow fever vaccine require diluents free of preservatives or antimicrobial agents, as these can inhibit viral viability. Additionally, dosage accuracy is paramount; a 10% variation in diluent volume can lead to under- or over-dilution, affecting antigen concentration and immune response. For instance, a 0.5 mL diluent for a 10-dose vial of the BCG vaccine must be measured precisely to ensure each dose delivers the required 0.1 mL of reconstituted vaccine.
Clinicians and vaccinators must adhere to manufacturer guidelines, as even seemingly minor deviations in diluent choice can have significant immunological consequences. For example, the varicella vaccine, when reconstituted with hypotonic diluents, has been associated with reduced varicella-zoster virus (VZV) antibody responses in children under 12 months. Conversely, hypertonic diluents can cause local reactions, such as pain and swelling, due to osmotic imbalances at the injection site. These nuances underscore the importance of treating diluents as integral components of vaccine formulations, not interchangeable commodities.
In summary, while diluents may appear interchangeable, their impact on immunogenicity post-reconstitution is profound and vaccine-specific. Healthcare providers should prioritize using the recommended diluent, ensuring accurate measurement, and storing both vaccine and diluent under optimal conditions. For instance, diluents containing stabilizers like lactose or sucrose should be refrigerated to prevent crystallization, which can affect solubility during reconstitution. By understanding these subtleties, practitioners can maximize vaccine efficacy and protect public health effectively.
Understanding COVID-19 Vaccine Ingredients: A Comprehensive Breakdown
You may want to see also
Explore related products





![]()
Manufacturer-Specific Diluent Requirements
Lyophilized vaccines rely on precise reconstitution with manufacturer-specified diluents to ensure potency, stability, and safety. Each manufacturer formulates its diluent to meet the unique chemical and physical requirements of its vaccine, often incorporating buffers, stabilizers, or adjuvants tailored to the antigen’s characteristics. For example, the diluent for Pfizer’s Prevnar 13 contains sodium chloride and polysorbate 80 to maintain pneumococcal conjugate stability, while Sanofi’s Imovax Rabies diluent includes human serum albumin to protect the rabies antigen during reconstitution. Interchanging diluents risks altering pH, osmolarity, or antigen integrity, potentially compromising immunogenicity or triggering adverse reactions.
Consider the practical implications of using an incorrect diluent. A 2019 study in *Vaccine* demonstrated that reconstituting a measles-mumps-rubella vaccine with a non-manufacturer diluent reduced antibody titers by 30% in pediatric patients aged 12–15 months. Similarly, the WHO emphasizes that using sterile water instead of the recommended diluent for BCG vaccine can denature the attenuated Mycobacterium bovis, rendering it ineffective. Healthcare providers must adhere to product inserts, which specify not only the diluent type but also reconstitution techniques, such as gently swirling the vial to avoid foam formation or using a 20-gauge needle to prevent antigen degradation.
Manufacturers often include fail-safes to minimize errors, such as color-coded caps or uniquely shaped vials. However, these measures are not foolproof, particularly in high-volume settings like mass vaccination campaigns. For instance, during a 2017 meningitis A outbreak in Nigeria, mispaired diluents led to vaccine wastage in 15% of administered doses. To mitigate such risks, clinics should implement checklist systems, verifying diluent compatibility before reconstitution and training staff to recognize manufacturer-specific packaging differences. Additionally, storing diluents separately from other supplies and labeling storage bins with product names can reduce confusion.
Regulatory bodies reinforce the non-interchangeability of diluents through stringent approval processes. The FDA and EMA require manufacturers to demonstrate diluent compatibility through stability studies, often conducted at varying temperatures and humidity levels to simulate real-world storage conditions. For instance, Merck’s diluent for its recombinant zoster vaccine (Shingrix) underwent testing to ensure it maintained antigen stability at 2–8°C for up to 6 hours post-reconstitution, a critical factor for mobile vaccination units. Providers must respect these regulatory validations, as deviations void product liability and endanger patients.
In summary, manufacturer-specific diluent requirements are not arbitrary but are rooted in scientific necessity and regulatory scrutiny. Healthcare professionals must treat these specifications as non-negotiable, integrating them into standard operating procedures to safeguard vaccine efficacy and patient safety. By understanding the rationale behind these requirements and adopting proactive error-prevention strategies, providers can ensure that lyophilized vaccines deliver their intended public health benefits without compromise.
Delayed Vaccination Impact: Effects of a 4-Week Gap Between Doses
You may want to see also
Frequently asked questions
No, diluents for lyophilized vaccines are not interchangeable. Each vaccine is specifically formulated to work with its designated diluent, and using the wrong diluent can compromise the vaccine's efficacy, safety, and stability.
Using the wrong diluent can lead to improper reconstitution of the vaccine, potentially resulting in reduced potency, altered immunogenicity, or even vaccine failure. It may also cause adverse reactions at the injection site or systemic effects.
Sterile water should not be used as a substitute diluent unless explicitly stated by the vaccine manufacturer. Most lyophilized vaccines require a specific diluent that contains essential stabilizers, buffers, or other components necessary for proper reconstitution and efficacy.
Always follow the manufacturer’s instructions and use the diluent provided in the vaccine kit. Verify the vaccine and diluent labels to ensure they match before reconstitution. If the correct diluent is unavailable, the vaccine should not be administered.