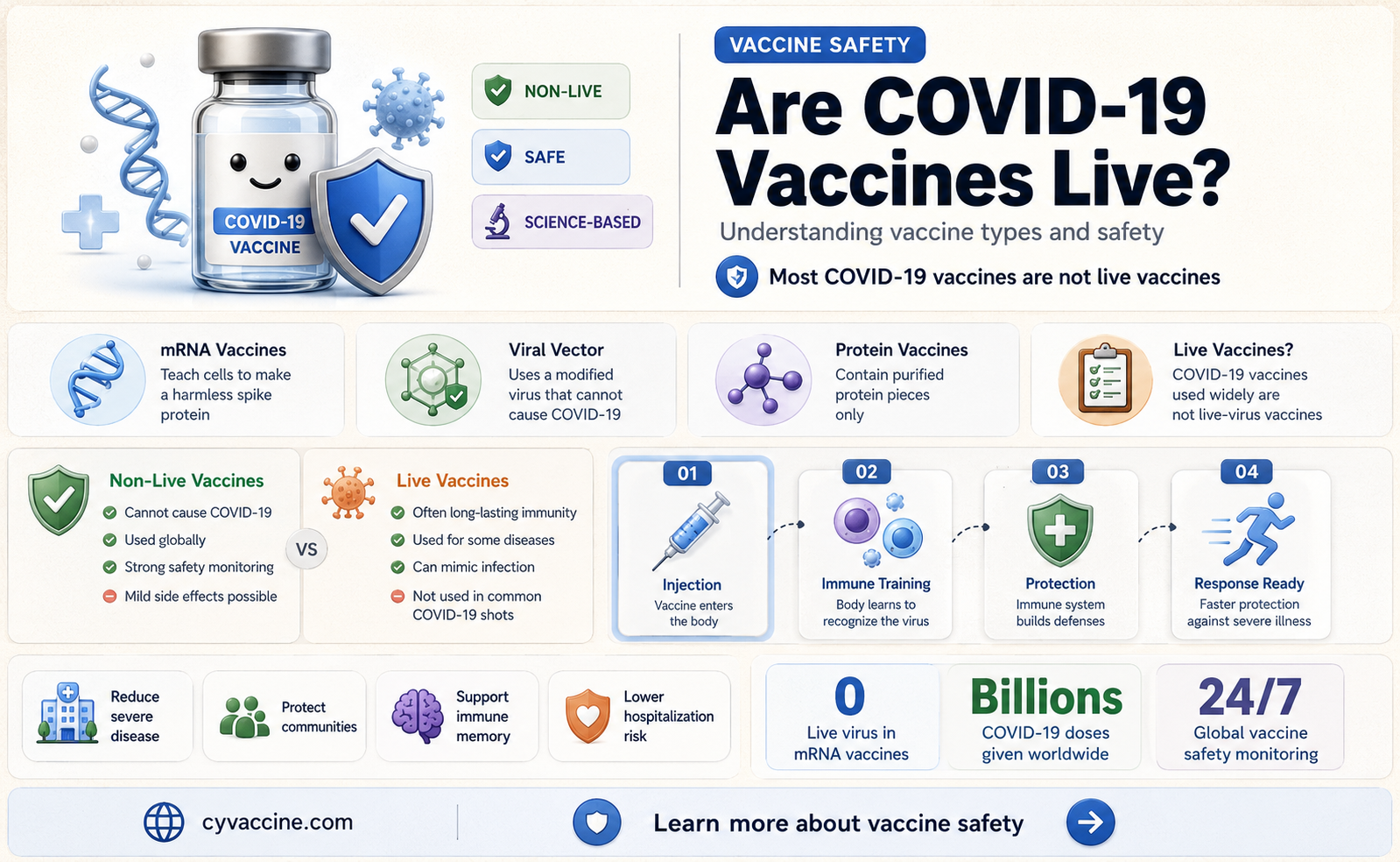
The question of whether coronavirus vaccines are live vaccines is a common one, given the variety of vaccine technologies used to combat COVID-19. Unlike live attenuated vaccines, which contain a weakened form of the virus to trigger an immune response, most COVID-19 vaccines, such as those developed by Pfizer-BioNTech and Moderna, utilize mRNA technology. These vaccines deliver genetic instructions to cells to produce a harmless piece of the virus’s spike protein, prompting the immune system to recognize and combat it without introducing any live virus. Other vaccines, like AstraZeneca’s and Johnson & Johnson’s, use viral vector technology, which employs a modified, non-replicating virus to deliver genetic material. None of these COVID-19 vaccines contain live coronavirus, making them safe for individuals with concerns about live vaccines. Understanding these distinctions is crucial for addressing vaccine hesitancy and ensuring public confidence in their safety and efficacy.
| Characteristics | Values |
|---|---|
| Vaccine Type | Most COVID-19 vaccines are not live vaccines. They are primarily mRNA, viral vector, or protein subunit vaccines. |
| mRNA Vaccines | Pfizer-BioNTech, Moderna (do not contain live virus; use genetic material to trigger immune response). |
| Viral Vector Vaccines | Johnson & Johnson (Janssen), AstraZeneca (use a harmless virus to deliver genetic instructions, but do not contain live SARS-CoV-2). |
| Protein Subunit Vaccines | Novavax (contains harmless pieces of the virus, not live virus). |
| Live Attenuated Vaccines | None of the widely approved COVID-19 vaccines are live attenuated. |
| Immune Response | All types induce immunity without introducing live virus, reducing risk of infection from the vaccine itself. |
| Storage Requirements | Varies by type (e.g., mRNA vaccines require ultra-cold storage initially, while others are more stable). |
| Efficacy | High efficacy against severe disease, hospitalization, and death across all types. |
| Safety Profile | Generally safe, with rare side effects (e.g., myocarditis in young males for mRNA vaccines). |
| Approval Status | Fully approved or authorized for emergency use in most countries, depending on the vaccine. |
Explore related products

$11.93 $21.99





What You'll Learn
- Definition of Live Vaccines: Live vaccines use weakened viruses to trigger immune responses
- COVID-19 Vaccine Types: Most COVID-19 vaccines are mRNA or viral vector, not live
- Live Vaccine Examples: Measles, mumps, rubella vaccines are live; COVID-19 is different
- Safety Concerns: Live vaccines are generally safe but not recommended for immunocompromised individuals
- COVID-19 Vaccine Myths: Misinformation claims COVID-19 vaccines are live, which is false
![]()
Definition of Live Vaccines: Live vaccines use weakened viruses to trigger immune responses
Live vaccines represent a cornerstone of immunization strategies, leveraging weakened pathogens to stimulate robust immune responses without causing disease. Unlike inactivated or subunit vaccines, live vaccines contain attenuated viruses that retain their ability to replicate, albeit at a reduced capacity. This replication mimics a natural infection, prompting the immune system to mount a comprehensive defense. For instance, the measles, mumps, and rubella (MMR) vaccine uses attenuated strains of these viruses to confer long-lasting immunity. This approach is particularly effective because it engages both humoral and cell-mediated immunity, often requiring fewer doses to achieve protection. However, the use of live viruses necessitates careful consideration of safety, especially in immunocompromised individuals or pregnant women.
When evaluating whether coronavirus vaccines fall into this category, it’s critical to examine their formulation. Most COVID-19 vaccines, such as Pfizer-BioNTech and Moderna, utilize mRNA technology, which instructs cells to produce a harmless spike protein, triggering an immune response. These are not live vaccines. However, some COVID-19 vaccines, like the Janssen (Johnson & Johnson) vaccine, employ a viral vector—a modified adenovirus—to deliver genetic material. While this vector is replication-competent, it does not constitute a live coronavirus vaccine. True live coronavirus vaccines, such as those developed in Russia (Sputnik V) and China (Convidecia), use weakened or modified adenoviruses to deliver SARS-CoV-2 antigens. These vaccines rely on the principles of live vaccination but do not contain live coronavirus itself.
The distinction matters for practical reasons. Live vaccines generally offer durable immunity but carry specific contraindications. For example, the MMR vaccine is not recommended for pregnant women or severely immunocompromised individuals due to the theoretical risk of viral replication. Similarly, live coronavirus vaccines, if developed, would require careful administration guidelines. Dosage would likely follow a single-shot regimen, as seen with the Janssen vaccine, but with heightened monitoring for adverse reactions. Age-specific recommendations might also apply, as children and older adults often have varying immune responses to live vaccines.
From a comparative standpoint, live vaccines excel in inducing strong, long-lasting immunity but pose challenges in storage and administration. They typically require refrigeration and must be handled with precision to maintain viral viability. In contrast, inactivated or mRNA vaccines offer greater stability but may necessitate booster doses. For coronaviruses, the decision to use a live vaccine would hinge on balancing efficacy, safety, and logistical feasibility. While no live SARS-CoV-2 vaccines are currently widely deployed, their potential remains a subject of research, particularly for regions with limited access to ultra-cold storage facilities.
In conclusion, live vaccines harness weakened viruses to provoke potent immune responses, a strategy that has proven effective for diseases like measles and polio. While most coronavirus vaccines do not fall into this category, the principles of live vaccination continue to inform vaccine development. Understanding these distinctions empowers individuals to make informed decisions about their health, ensuring that vaccination strategies align with both scientific evidence and practical considerations. Whether through live, inactivated, or novel technologies, the goal remains the same: to protect populations from infectious threats with safe, effective, and accessible solutions.
Essential Nursing Strategies for Effective Vaccine Implementation and Patient Care
You may want to see also
Explore related products






![]()
COVID-19 Vaccine Types: Most COVID-19 vaccines are mRNA or viral vector, not live
The majority of COVID-19 vaccines authorized for use globally are either mRNA or viral vector types, not live vaccines. This distinction is crucial for understanding how these vaccines work and addressing concerns about their safety and efficacy. mRNA vaccines, such as Pfizer-BioNTech and Moderna, deliver genetic instructions to cells to produce a harmless piece of the SARS-CoV-2 spike protein, triggering an immune response. Viral vector vaccines, like AstraZeneca and Johnson & Johnson, use a modified virus (e.g., adenovirus) to transport genetic material into cells, prompting a similar immune reaction. Neither type contains live coronavirus, eliminating the risk of causing COVID-19.
Analyzing the mechanisms reveals why live vaccines are not the primary approach for COVID-19. Live vaccines, such as those for measles or chickenpox, use weakened forms of the virus to induce immunity. While effective, this method carries a small risk of the virus reverting to a virulent form, particularly in immunocompromised individuals. For COVID-19, the urgency of vaccine development and the need for safety across diverse populations led researchers to prioritize mRNA and viral vector technologies. These platforms offer rapid scalability, fewer safety concerns, and the ability to adapt quickly to emerging variants.
For practical application, understanding vaccine types helps individuals make informed decisions. mRNA vaccines typically require two doses, administered 3–4 weeks apart, with a booster recommended 6 months later for sustained immunity. Viral vector vaccines often require one dose, though some regions recommend a second dose for enhanced protection. Age-specific guidelines vary: Pfizer’s mRNA vaccine is approved for individuals aged 5 and older, while Moderna’s is for those 18 and up. Viral vector vaccines are generally approved for adults, though Johnson & Johnson’s single-dose option has been particularly useful in hard-to-reach populations.
Comparatively, the absence of live vaccines in the COVID-19 arsenal highlights the evolution of vaccine technology. Traditional live vaccines have been cornerstone tools in public health, but modern platforms like mRNA and viral vectors represent a leap forward in precision and safety. For instance, mRNA vaccines degrade quickly in the body after delivering their instructions, leaving no long-term genetic footprint. Viral vector vaccines, while relying on a virus, ensure the delivered material cannot replicate or cause disease. This innovation minimizes risks while maximizing immune response efficiency.
In conclusion, the dominance of mRNA and viral vector vaccines in the COVID-19 response underscores a strategic shift in vaccine development. By avoiding live viruses, these technologies provide a safer, more adaptable solution for a global pandemic. For individuals, knowing the type of vaccine they receive can alleviate concerns and ensure compliance with dosing schedules. As research progresses, these platforms may become the standard for future vaccines, reshaping how we combat infectious diseases.
Claiming Religious Exemption for Vaccines in Massachusetts: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Live Vaccine Examples: Measles, mumps, rubella vaccines are live; COVID-19 is different
The measles, mumps, and rubella (MMR) vaccine is a cornerstone of childhood immunization, administered typically in two doses: the first at 12–15 months and the second at 4–6 years. This vaccine contains live, attenuated viruses, meaning they are weakened but still alive, triggering a robust immune response without causing the disease. The MMR vaccine’s live nature allows it to confer long-lasting immunity, often for life, with effectiveness rates exceeding 97% after two doses. This approach contrasts sharply with COVID-19 vaccines, which predominantly use mRNA or viral vector technologies, not live viruses. Understanding this distinction is crucial for appreciating the diversity of vaccine mechanisms and their suitability for different diseases.
Consider the practical implications of live vaccines like MMR. They are contraindicated in immunocompromised individuals, pregnant women, and those with severe allergies to vaccine components. For instance, a child with HIV or undergoing chemotherapy cannot receive the MMR vaccine due to the risk of the attenuated virus causing illness. COVID-19 vaccines, however, are generally safe for these populations because they do not contain live viruses. This difference highlights the importance of tailoring vaccine technology to the disease and the recipient’s health status, ensuring both efficacy and safety.
From a comparative perspective, live vaccines like MMR rely on the body’s ability to mount a response to a weakened pathogen, mimicking natural infection. COVID-19 vaccines, on the other hand, introduce genetic material (mRNA) or a harmless virus (viral vector) to instruct cells to produce a spike protein, prompting an immune response. While both strategies aim to prevent disease, the absence of live virus in COVID-19 vaccines eliminates the risk of vaccine-induced illness, making them a safer option for vulnerable populations. This innovation underscores the evolution of vaccine technology in response to specific viral challenges.
For parents and caregivers, understanding these differences can alleviate concerns about vaccine safety. The MMR vaccine’s live nature has been proven safe and effective for decades, with rare side effects limited to mild fever or rash. COVID-19 vaccines, despite being newer, have undergone rigorous testing and monitoring, with side effects typically mild and short-lived. A practical tip: ensure children receive their MMR doses on schedule, as delays can leave them susceptible to outbreaks. For COVID-19, follow age-specific guidelines—for example, the Pfizer vaccine is approved for children as young as 6 months, with dosages adjusted for age groups.
In conclusion, while live vaccines like MMR have been a gold standard for preventing infectious diseases, COVID-19 vaccines represent a technological leap, avoiding live viruses altogether. This divergence reflects the adaptability of vaccine science to address unique viral threats. Whether live or not, vaccines remain one of the most powerful tools in public health, each designed with precision to protect against specific diseases while minimizing risks. Recognizing these differences empowers individuals to make informed decisions about their health and the health of their loved ones.
Yellow Fever Vaccine Introduction in Nigeria: A Historical Overview
You may want to see also
Explore related products






![]()
Safety Concerns: Live vaccines are generally safe but not recommended for immunocompromised individuals
Live vaccines, such as those for measles, mumps, and chickenpox, contain weakened forms of the virus that trigger an immune response without causing severe illness. This approach has proven effective in preventing infectious diseases, but it comes with a critical caveat: immunocompromised individuals should avoid them. These vaccines rely on a functional immune system to handle the attenuated virus safely. For those with weakened immunity—due to conditions like HIV, cancer treatments, or organ transplants—the risk of the vaccine strain replicating unchecked and causing disease is significantly higher. This isn’t merely theoretical; documented cases of vaccine-associated illness in immunocompromised patients underscore the need for caution.
Consider the MMR (measles, mumps, rubella) vaccine, a live vaccine administered in two doses, typically at 12–15 months and 4–6 years. While it’s safe for the general population, it’s contraindicated for severely immunocompromised children. For example, a child undergoing chemotherapy would need to defer vaccination until their immune system recovers. Similarly, adults with conditions like leukemia or those on high-dose corticosteroids must consult their healthcare provider before receiving live vaccines. The risk isn’t just theoretical—it’s quantifiable. Studies show that immunocompromised individuals receiving live vaccines face a 10–20% risk of vaccine-related complications, compared to near-zero risk in immunocompetent individuals.
The COVID-19 vaccines, however, differ significantly from traditional live vaccines. None of the authorized COVID-19 vaccines (Pfizer, Moderna, Johnson & Johnson, AstraZeneca, etc.) contain live coronavirus. mRNA vaccines (Pfizer, Moderna) use genetic material to instruct cells to produce a harmless spike protein, while viral vector vaccines (Johnson & Johnson, AstraZeneca) use a modified, non-replicating virus to deliver instructions. This design eliminates the risk of the vaccine causing COVID-19, making them safer for immunocompromised individuals. However, their immune response to these vaccines may be suboptimal, necessitating additional doses or precautions, such as Pfizer’s recommendation for a third primary dose in immunocompromised adults.
For immunocompromised individuals, the decision to vaccinate involves balancing risk and benefit. While live vaccines are off-limits, non-live alternatives like inactivated or subunit vaccines (e.g., flu shots, COVID-19 vaccines) are generally safe. Practical steps include verifying vaccine type before administration, spacing vaccines appropriately (e.g., waiting 2 weeks after stopping high-dose steroids), and consulting specialists for tailored advice. For instance, a transplant recipient might receive a COVID-19 vaccine but should avoid the live shingles vaccine. Clear communication with healthcare providers is essential, as is staying updated on evolving guidelines, such as the CDC’s recommendations for additional COVID-19 doses in immunocompromised populations.
In summary, while live vaccines are a cornerstone of preventive medicine, their safety profile excludes immunocompromised individuals due to the risk of vaccine-induced illness. COVID-19 vaccines, being non-live, offer a safer alternative but require careful management in this population. By understanding these distinctions and following evidence-based protocols, healthcare providers and patients can navigate vaccination safely, ensuring protection without compromising health.
Essential Vaccine Shots: Names, Types, and What You Need to Know
You may want to see also
Explore related products






![]()
COVID-19 Vaccine Myths: Misinformation claims COVID-19 vaccines are live, which is false
Misinformation about COVID-19 vaccines has led some to believe these vaccines contain live coronavirus, a claim that is entirely false. The Pfizer-BioNTech and Moderna mRNA vaccines, for instance, work by delivering genetic instructions to cells to produce a harmless piece of the virus’s spike protein, triggering an immune response. These vaccines do not contain any live virus and cannot cause COVID-19. Similarly, the Johnson & Johnson vaccine uses a modified adenovirus vector that cannot replicate in the body, making it impossible to transmit or cause infection. Understanding these mechanisms is crucial to dispelling myths and building trust in vaccine safety.
One common misconception stems from confusing "live vaccines" with "viral vector" or "mRNA" technologies. Live vaccines, like those for measles or chickenpox, use a weakened form of the virus to stimulate immunity. COVID-19 vaccines, however, employ different approaches. For example, the mRNA vaccines degrade quickly after delivering their instructions, while the adenovirus vector in the Johnson & Johnson vaccine is engineered to be non-replicating. These designs ensure the vaccines cannot cause COVID-19 or alter human DNA, addressing two widespread fears fueled by misinformation.
Practical tips can help individuals verify vaccine information. Always consult reputable sources such as the CDC, WHO, or local health authorities. Be wary of sensationalist claims on social media or unverified platforms. For parents concerned about vaccinating children (ages 5 and up for Pfizer, 18 and up for Moderna and Johnson & Johnson), understanding the vaccine’s mechanism can alleviate fears. For example, the pediatric Pfizer dose is 10 micrograms, one-third of the adult dosage, tailored for younger immune systems while maintaining safety and efficacy.
Comparing COVID-19 vaccines to traditional live vaccines highlights their differences. While live vaccines introduce a weakened virus to stimulate immunity, COVID-19 vaccines use innovative technologies to mimic viral components without the virus itself. This distinction is vital for countering misinformation. For instance, the flu vaccine, which can be live-attenuated (nasal spray), is fundamentally different from the COVID-19 vaccines, which are not live in any form. Recognizing these differences empowers individuals to make informed decisions and challenge false narratives.
Finally, addressing the root of this myth requires a persuasive approach. Fear of the unknown often drives misinformation, but science provides clarity. COVID-19 vaccines have undergone rigorous testing and are continuously monitored for safety. Millions of doses administered globally have demonstrated their effectiveness in preventing severe illness and death. By focusing on evidence-based facts and sharing accurate information, we can combat myths and protect public health. The takeaway is clear: COVID-19 vaccines are not live vaccines, and understanding this truth is essential for widespread vaccination efforts.
Same Vaccine for Boosters: Better Immunity or Mix-and-Match?
You may want to see also
Frequently asked questions
No, none of the authorized COVID-19 vaccines in the U.S. (Pfizer-BioNTech, Moderna, or Johnson & Johnson) are live vaccines. They do not contain a live virus.
COVID-19 vaccines, such as mRNA vaccines (Pfizer and Moderna) and viral vector vaccines (Johnson & Johnson), teach the body to recognize and fight the virus without using a live virus. They introduce harmless genetic material or a modified virus to trigger an immune response.
No, COVID-19 vaccines cannot give you COVID-19. Since they do not contain a live virus, they cannot cause infection. Side effects like fever or fatigue are normal signs of the immune system responding, not the disease itself.
COVID-19 vaccines were developed using newer technologies like mRNA and viral vectors, which are safer and faster to produce than live vaccines. These methods avoid the risks associated with using a live virus, especially for a novel virus like SARS-CoV-2.
Live vaccines are highly effective for many diseases, but COVID-19 vaccines have proven to be extremely effective in preventing severe illness, hospitalization, and death. The choice of technology depends on the virus and the goals of vaccination, not on effectiveness alone.