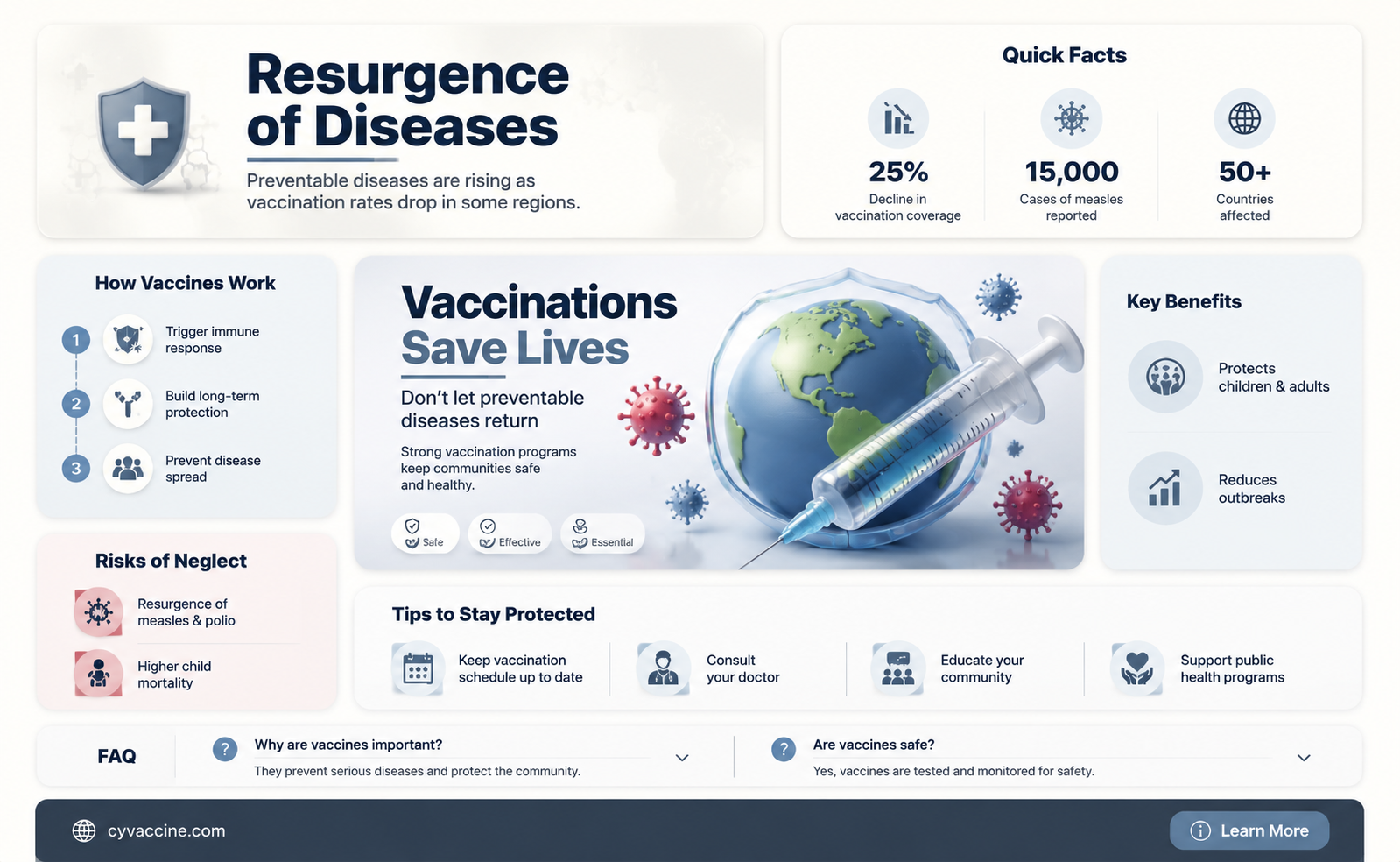
The resurgence of preventable diseases, such as measles and whooping cough, has sparked widespread concern about the impact of declining vaccination rates. As more individuals opt out of immunizations due to misinformation, personal beliefs, or lack of access, communities are experiencing outbreaks of diseases once thought to be under control. This alarming trend raises critical questions about the consequences of vaccine hesitancy, the role of public health policies, and the importance of collective immunity in protecting vulnerable populations. Understanding the factors driving this phenomenon is essential to addressing the growing threat of vaccine-preventable diseases and ensuring global health security.
| Characteristics | Values |
|---|---|
| Disease Resurgence | Measles, pertussis (whooping cough), mumps, diphtheria, polio (in some regions) |
| Cause of Resurgence | Declining vaccination rates due to vaccine hesitancy, misinformation, and access issues |
| Geographic Impact | Global, with hotspots in regions with low vaccination coverage (e.g., Africa, parts of Europe, and the U.S.) |
| Demographic Affected | Primarily children and unvaccinated adults |
| Health Impact | Increased hospitalizations, complications (e.g., encephalitis from measles), and deaths |
| Economic Impact | Higher healthcare costs, loss of productivity, and strain on public health systems |
| Vaccination Coverage Decline | Measles vaccination rates dropped globally from 86% in 2019 to 81% in 2021 (WHO data) |
| Recent Outbreaks | Measles outbreaks in 2022-2023 in the U.S., UK, and parts of Europe; polio resurgence in Pakistan and Afghanistan |
| Role of Misinformation | Social media and anti-vaccine campaigns contribute to declining trust in vaccines |
| Public Health Response | Campaigns to increase vaccination rates, education initiatives, and policy changes (e.g., vaccine mandates) |
| Long-Term Risks | Potential loss of herd immunity, increased risk of endemic diseases returning |
Explore related products






What You'll Learn
- Resurgence of Measles: Outbreaks increase globally due to declining vaccination rates in communities
- Whooping Cough Comeback: Pertussis cases rise as vaccine hesitancy grows among parents
- Polio Reemergence: Risk of polio returning in regions with low vaccination coverage
- Mumps Outbreaks: Colleges and schools see mumps outbreaks linked to vaccine refusal
- Tetanus Threat: Tetanus cases persist in areas with inadequate vaccination programs
![]()
Resurgence of Measles: Outbreaks increase globally due to declining vaccination rates in communities
Measles, once on the brink of eradication, is staging a comeback. Global data from the World Health Organization (WHO) reveals a startling 79% increase in measles cases between 2021 and 2022, with nearly 9 million infections and 136,000 deaths. This resurgence isn’t due to a new, more virulent strain, but rather to a predictable consequence: declining vaccination rates. The measles vaccine, administered in two doses (typically at 12–15 months and 4–6 years), provides 97% immunity. Yet, in communities where vaccination coverage dips below 95%, herd immunity falters, allowing the virus to spread rapidly among susceptible individuals.
The reasons for declining vaccination rates are multifaceted. Misinformation campaigns, often amplified on social media, have sown doubt about vaccine safety despite decades of evidence proving their efficacy and minimal side effects. In some regions, logistical challenges, such as disrupted healthcare services during the COVID-19 pandemic, have left millions of children unvaccinated. For instance, UNICEF reported that 25 million children missed out on routine immunizations in 2021, the highest number in over a decade. These gaps in immunity create fertile ground for measles outbreaks, as seen in recent crises in Somalia, Yemen, and parts of Europe.
Consider the 2019 measles outbreak in the Pacific Northwest of the United States, where a single case imported from overseas sparked over 70 infections in an undervaccinated community. Schools were forced to close, and public health officials scrambled to contain the spread. This scenario underscores a critical point: measles is not just a childhood illness but a highly contagious virus that can infect anyone without immunity. Adults who received only one dose of the vaccine or those born before 1957 (when measles was widespread) may be particularly vulnerable. A simple blood test can verify immunity, and adults without it can receive a catch-up dose, ensuring protection.
To combat this resurgence, a multi-pronged approach is essential. Public health campaigns must counter misinformation with clear, evidence-based messaging about vaccine safety and efficacy. Healthcare systems need to prioritize routine immunizations, especially in underserved areas, and offer flexible scheduling to accommodate families. Schools and workplaces can play a role by promoting vaccination drives and requiring proof of immunity for attendance. For travelers, the CDC recommends ensuring measles immunity before visiting regions with active outbreaks, as the virus knows no borders.
The takeaway is clear: measles outbreaks are preventable, but only if communities prioritize vaccination. The decline in immunization rates isn’t just a statistical trend—it’s a ticking time bomb that threatens global health. By understanding the risks, addressing barriers to access, and fostering trust in science, we can reverse this alarming resurgence and protect future generations from a disease that should have been consigned to history.
Understanding Moderna's COVID-19 Vaccine: Key Ingredients Explained
You may want to see also
Explore related products






![]()
Whooping Cough Comeback: Pertussis cases rise as vaccine hesitancy grows among parents
The resurgence of whooping cough, or pertussis, serves as a stark reminder of the consequences of declining vaccination rates. Once considered a relic of the past, this highly contagious respiratory disease is making a comeback, particularly among children. The Centers for Disease Control and Prevention (CDC) reports a steady rise in pertussis cases over the past decade, coinciding with growing vaccine hesitancy among parents. This trend is not merely a statistical anomaly but a public health crisis with tangible impacts on communities.
Consider the vaccination schedule for pertussis, which is part of the DTaP (diphtheria, tetanus, and acellular pertussis) vaccine. Infants receive doses at 2, 4, and 6 months, followed by boosters at 15–18 months and 4–6 years. Adolescents and adults require a Tdap booster to maintain immunity. Despite this clear roadmap, misinformation about vaccine safety has led some parents to delay or refuse vaccinations, creating pockets of vulnerability. For instance, in 2020, California saw a 40% drop in kindergarten vaccination rates, correlating with localized pertussis outbreaks. The irony is palpable: a disease once nearly eradicated is now thriving in communities where skepticism outweighs science.
The mechanics of pertussis transmission underscore the urgency of vaccination. The bacterium *Bordetella pertussis* spreads through respiratory droplets, and its symptoms—initially mild, then escalating to violent coughing fits—can be life-threatening, especially in infants too young to be fully vaccinated. Herd immunity, which protects these vulnerable populations, falters when vaccination rates drop below 95%. A single unvaccinated child can become a vector, reintroducing the disease into schools and households. This is not a theoretical risk; in 2019, a pertussis outbreak in an Oregon school district infected over 20 students, many of whom were unvaccinated due to parental exemptions.
Addressing this issue requires a multi-pronged approach. Healthcare providers must engage in open, empathetic conversations with hesitant parents, debunking myths while emphasizing the proven safety and efficacy of vaccines. Schools can play a role by enforcing vaccination requirements and offering educational resources. Policymakers should strengthen immunization mandates while ensuring equitable access to vaccines. For parents, the takeaway is clear: vaccination is not just a personal choice but a communal responsibility. The whooping cough comeback is a preventable tragedy, and reversing this trend begins with informed, decisive action.
Are 100% Effective Vaccines Common? Exploring Real-World Efficacy Rates
You may want to see also
Explore related products






![]()
Polio Reemergence: Risk of polio returning in regions with low vaccination coverage
Polio, once on the brink of eradication, is staging a comeback in regions with low vaccination coverage. In 2022, the United States detected poliovirus in New York wastewater, leading to an emergency vaccination campaign. This resurgence underscores a chilling reality: when vaccination rates drop below 95%, herd immunity falters, and the virus finds fertile ground to spread. The oral polio vaccine (OPV), requiring multiple doses (typically 3–4) for full protection in children under 5, is particularly critical in low-resource areas. Yet, misinformation, vaccine hesitancy, and disrupted healthcare systems have left gaps in immunity, allowing polio to reemerge.
Consider the mechanics of this reemergence. Polio is highly contagious, spreading through fecal-oral transmission or contaminated water. In communities with inadequate sanitation and low vaccination rates, a single case can quickly escalate into an outbreak. The inactivated polio vaccine (IPV), often used in wealthier nations, provides individual protection but does not stop viral shedding, making OPV essential in outbreak settings. However, OPV’s rarity in some regions, coupled with its occasional reversion to a virulent form (vaccine-derived poliovirus), complicates eradication efforts. This dual challenge—insufficient coverage and vaccine limitations—creates a perfect storm for polio’s return.
To combat this threat, targeted strategies are essential. First, strengthen routine immunization programs, ensuring at least 95% of children receive all recommended doses of OPV and IPV. Second, conduct door-to-door campaigns in high-risk areas, prioritizing accessibility and dispelling myths through trusted community leaders. Third, integrate polio vaccination with other health services, such as vitamin A supplementation, to maximize reach. For travelers to endemic regions, the CDC recommends a single lifetime IPV booster if their last dose was over 10 years ago. These steps, though resource-intensive, are far less costly than managing a full-blown outbreak.
The takeaway is clear: polio’s reemergence is not inevitable but a consequence of preventable gaps in immunity. History shows that eradication is possible—cases have dropped 99% since 1988—but only with sustained vigilance. Regions with low vaccination coverage must act now, combining scientific rigor with community engagement to close the immunity gap. The alternative is a return to a world where polio paralyzes thousands annually, a grim reminder of the stakes in the fight against vaccine-preventable diseases.
Essential Puppy Vaccinations: Understanding the 5-Way Shot Components
You may want to see also
Explore related products

![[Vaccine Safety Manual for Concerned Families and Health Practitioners: Guide to Immunization Risks and Protection] (By: Neil Z. Miller) [published: December, 2011]](https://m.media-amazon.com/images/I/61NT9afIQyL._AC_UY218_.jpg)




![]()
Mumps Outbreaks: Colleges and schools see mumps outbreaks linked to vaccine refusal
Mumps outbreaks are resurging in colleges and schools, with a startling correlation to vaccine refusal. Once considered a rarity in the U.S. due to widespread vaccination, mumps cases have climbed in recent years, particularly in close-quarters environments like dormitories and classrooms. The CDC reports that between 2016 and 2017, over 150 outbreaks occurred nationwide, many linked to under-vaccinated populations. This trend underscores a critical issue: declining vaccination rates are not just individual choices but communal risks.
The MMR (measles, mumps, rubella) vaccine, typically administered in two doses at 12–15 months and 4–6 years, provides 78% effectiveness against mumps after one dose and 88% after two. However, immunity can wane over time, and crowded living conditions accelerate transmission. Colleges often require proof of vaccination, but exemptions for personal or philosophical reasons have created pockets of vulnerability. For instance, a 2016 outbreak at Harvard University infected 58 students, many of whom had received both doses but were exposed to unvaccinated peers. This highlights the vaccine’s limitations in the face of declining herd immunity.
To mitigate mumps outbreaks, schools and health departments must take proactive steps. First, enforce stricter vaccination policies with limited exemptions, ensuring at least 95% coverage for herd immunity. Second, offer on-campus MMR booster shots for students, particularly those in high-density housing. Third, educate communities about mumps symptoms—fever, swollen glands, and jaw pain—and the importance of isolation during illness. Parents and students should also be reminded that mumps complications, such as deafness or infertility, are rare but serious, making vaccination a critical preventive measure.
Critics of vaccine mandates argue for personal freedom, but the data is clear: unvaccinated individuals are 9 times more likely to contract mumps. This isn’t just about protecting oneself; it’s about safeguarding those who cannot be vaccinated due to medical conditions. Schools must balance individual rights with public health, prioritizing evidence-based policies. As mumps cases continue to rise, the choice to vaccinate isn’t just personal—it’s a responsibility to the community.
Verify Your Vaccine Certificate: Quick Steps to Check Validity
You may want to see also
Explore related products






![]()
Tetanus Threat: Tetanus cases persist in areas with inadequate vaccination programs
Tetanus, a potentially fatal bacterial infection, remains a persistent threat in regions with inadequate vaccination programs. Unlike diseases that spread from person to person, tetanus is caused by Clostridium tetani spores found in soil, dust, and animal feces. These spores enter the body through breaks in the skin, such as puncture wounds, burns, or even minor cuts, and produce a toxin that causes muscle stiffness and spasms. While global vaccination efforts have significantly reduced tetanus cases, areas with low immunization rates continue to report outbreaks, highlighting the critical role of vaccination in prevention.
Understanding the Vaccine: The tetanus vaccine, often administered as part of the DTaP (diphtheria, tetanus, and pertussis) or Tdap series, provides robust protection against the disease. For children, the CDC recommends a series of five DTaP shots, starting at 2 months of age, followed by a Tdap booster at 11–12 years. Adults need Tdap boosters every 10 years to maintain immunity. A single dose of the tetanus vaccine is approximately 95% effective in preventing the disease, making it one of the most reliable tools in public health. However, in regions where access to healthcare is limited, vaccination rates drop, leaving populations vulnerable to infection.
Case Studies and Trends: In countries with weak healthcare infrastructure, tetanus cases often spike during natural disasters or conflicts, when injuries are common and medical resources scarce. For instance, following the 2010 Haiti earthquake, tetanus cases surged due to widespread injuries and inadequate vaccination coverage. Similarly, in parts of Africa and Southeast Asia, neonatal tetanus—a form of the disease affecting newborns—remains a concern in areas where mothers are unvaccinated and childbirth occurs in unsanitary conditions. These examples underscore the direct correlation between vaccination rates and disease prevalence.
Practical Prevention Tips: For individuals traveling to or living in areas with low vaccination coverage, taking proactive measures is essential. Always ensure tetanus vaccination is up to date before travel, especially if engaging in outdoor activities that increase the risk of injury. Clean wounds thoroughly with soap and water, and seek medical attention for deep or dirty injuries, as a booster shot may be necessary. For communities, public health initiatives should focus on increasing vaccine accessibility, educating populations about the importance of immunization, and strengthening healthcare systems to respond to outbreaks.
The Takeaway: Tetanus is a preventable disease, yet it continues to pose a threat in regions with inadequate vaccination programs. The persistence of cases serves as a stark reminder of the importance of global immunization efforts. By prioritizing vaccination, improving healthcare access, and raising awareness, societies can effectively combat this ancient scourge and protect vulnerable populations from its devastating effects.
B Cell Activation and Vaccines: Unlocking Immune Memory Mechanisms
You may want to see also
Frequently asked questions
Yes, diseases like measles, pertussis (whooping cough), and polio have seen resurgence in areas with declining vaccination rates, as vaccines are key to preventing their spread.
Declining vaccination rates, often due to misinformation or vaccine hesitancy, reduce herd immunity, allowing diseases to spread more easily among unprotected populations.
Yes, diseases like polio and measles can return if vaccination rates fall, as they can be reintroduced through international travel or local transmission in unvaccinated communities.
Vaccine hesitancy contributes significantly by lowering immunity levels in populations, creating opportunities for diseases to spread and cause outbreaks.
Maintaining high vaccination rates, educating the public about vaccine safety and efficacy, and addressing misinformation are crucial to preventing the resurgence of preventable diseases.