The question of whether antibodies are as effective as vaccines in preventing diseases has sparked significant debate in the scientific community. While both antibodies and vaccines aim to protect the body from pathogens, they operate through distinct mechanisms. Vaccines stimulate the immune system to produce its own antibodies and memory cells, offering long-term immunity and often preventing infection altogether. In contrast, antibody treatments, such as monoclonal antibodies, provide immediate but temporary protection by directly introducing lab-created antibodies into the body. While antibodies can be lifesaving for those already infected or at high risk, vaccines remain the gold standard for disease prevention due to their ability to confer durable immunity and reduce transmission at a population level. This comparison highlights the complementary roles of these tools in modern medicine.
Explore related products






What You'll Learn
![]()
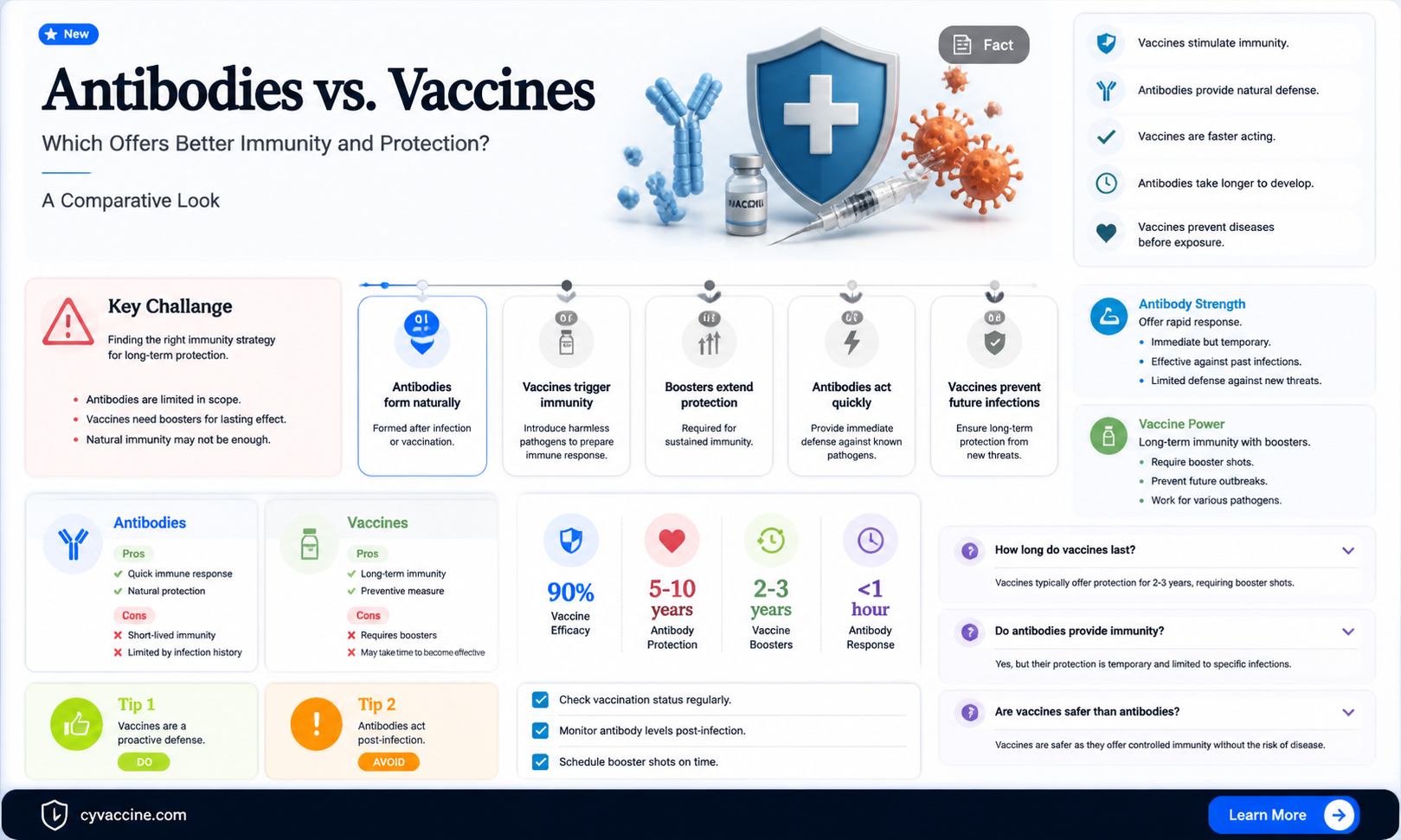
Antibody vs. Vaccine Efficacy
Antibodies and vaccines both play critical roles in immune defense, but their mechanisms and efficacy differ significantly. Vaccines stimulate the body’s immune system to produce its own antibodies and memory cells, offering long-term protection against specific pathogens. Antibodies, whether naturally produced or administered via monoclonal antibody treatments, provide immediate but temporary immunity. For instance, COVID-19 vaccines like Pfizer-BioNTech (95% efficacy in clinical trials) train the immune system to recognize and combat the virus, while monoclonal antibody treatments like Regeneron’s REGEN-COV offer short-term protection (70-80% reduction in hospitalization) but require repeated doses. This fundamental difference in duration underscores why vaccines are generally preferred for widespread prevention.
Consider the practical implications for different populations. Vaccines are particularly effective in healthy individuals aged 5–64, where robust immune responses are typical. However, in immunocompromised individuals or those over 65, antibody treatments can serve as a vital bridge until vaccination takes effect. For example, a 70-year-old with a weakened immune system might receive a 1,200 mg dose of REGEN-COV intravenously to prevent severe COVID-19 while awaiting a vaccine booster. This highlights the complementary, not competitive, nature of antibodies and vaccines in clinical practice.
From a cost-benefit perspective, vaccines are more cost-effective for population-level immunity. A single dose of the Moderna vaccine costs approximately $32–$37, providing protection for up to a year or more. In contrast, a dose of REGEN-COV costs around $2,100 and lasts only a few weeks. While antibody treatments are invaluable in high-risk scenarios, their expense and logistical challenges (e.g., intravenous administration) limit their scalability. Vaccines, therefore, remain the cornerstone of public health strategies due to their affordability and long-term efficacy.
A key takeaway is that antibodies and vaccines serve distinct purposes. Vaccines are proactive, building immunity before exposure, while antibodies are reactive, treating or preventing disease post-exposure. For travelers visiting high-risk areas, a vaccine like Yellow Fever (99% effective after one dose) is ideal for prevention, whereas a rabies antibody treatment (1,500 IU/kg intramuscularly) is crucial if bitten by a potentially rabid animal. Understanding these differences empowers individuals and healthcare providers to make informed decisions tailored to specific needs and contexts.
Exploring the Downsides of Various Vaccine Types and Their Impact
You may want to see also
Explore related products






![]()
Duration of Protection Comparison
The duration of protection offered by antibodies versus vaccines is a critical factor in public health strategies, particularly in managing infectious diseases. Vaccines, designed to stimulate the immune system to produce memory cells and antibodies, typically provide long-lasting immunity, often measured in years or even decades. For instance, the measles vaccine confers protection for over 20 years in most individuals, while the tetanus vaccine requires boosters every 10 years to maintain immunity. In contrast, naturally acquired antibodies from infection or passive antibody therapy (such as monoclonal antibodies) generally offer shorter-term protection, ranging from weeks to months. For example, convalescent plasma therapy for COVID-19 provides antibodies that wane within 3–6 months, necessitating repeated treatments for sustained protection.
Analyzing the mechanisms behind these differences reveals why vaccines often outperform antibodies in longevity. Vaccines introduce a controlled antigen, triggering both humoral and cell-mediated immunity, including the development of memory B and T cells. These memory cells persist in the body, enabling a rapid and robust response upon re-exposure to the pathogen. Antibodies, whether naturally acquired or administered, lack this memory component. They circulate in the bloodstream and provide immediate protection but gradually decline over time, leaving the individual susceptible once levels drop below a protective threshold. This is why vaccinated individuals often maintain immunity for years, while those relying on antibody therapy require frequent interventions.
For practical purposes, understanding these differences is essential for tailoring interventions to specific populations. For example, elderly individuals or those with compromised immune systems may benefit from antibody therapies for immediate protection but still require vaccination for long-term immunity. In the case of COVID-19, monoclonal antibody treatments like casirivimab-imdevimab provided a 70–80% reduction in hospitalization risk for up to 3 months but were not a substitute for vaccination. Similarly, pregnant women, who are at higher risk for severe illness, may receive antibody treatments during outbreaks but should also be vaccinated to ensure prolonged protection for both themselves and their infants.
A comparative analysis highlights the trade-offs between the two approaches. Vaccines are cost-effective and scalable, making them ideal for population-wide immunity. However, their development and distribution can take months or years, as seen during the COVID-19 pandemic. Antibody therapies, on the other hand, offer rapid protection and can be deployed quickly in emergencies but are more expensive and require repeated administration. For instance, a single dose of monoclonal antibodies for COVID-19 costs around $2,000, compared to $20–50 for a vaccine dose. This makes vaccines the more sustainable option for long-term public health strategies, while antibodies serve as a valuable stopgap for high-risk groups or during outbreaks.
In conclusion, while antibodies provide immediate and effective protection, vaccines remain superior in terms of duration and sustainability. Public health strategies should prioritize vaccination for broad, long-term immunity while leveraging antibody therapies for targeted, short-term interventions. For individuals, staying up-to-date with recommended vaccines and consulting healthcare providers about antibody treatments when necessary ensures optimal protection against infectious diseases.
Mpox Vaccine: Effective Against Clade 1?
You may want to see also
Explore related products






![]()
Cost-Effectiveness Analysis
Antibodies and vaccines serve distinct roles in immune protection, but their cost-effectiveness varies significantly depending on context. A cost-effectiveness analysis (CEA) evaluates the financial efficiency of these interventions by comparing their costs to health outcomes, typically measured in dollars per quality-adjusted life year (QALY). For vaccines, the upfront investment is often recouped through long-term prevention of disease, reducing healthcare costs and productivity losses. For example, the measles vaccine costs approximately $1–$2 per dose but prevents a disease with treatment costs exceeding $5,000 per case. In contrast, antibody therapies, such as monoclonal antibodies for COVID-19, can cost $2,000 per dose and provide short-term protection, making them less cost-effective for widespread use but valuable in high-risk populations.
To conduct a CEA for antibodies versus vaccines, follow these steps: first, define the population (e.g., elderly individuals, immunocompromised patients, or general public). Second, calculate the total costs, including administration, storage, and adverse event management. Third, measure health outcomes using metrics like QALYs or disability-adjusted life years (DALYs). For instance, a vaccine with 90% efficacy in preventing hospitalizations may save $10,000 per avoided case, while antibody therapy might cost $5,000 per treated individual with a 50% reduction in severe outcomes. Tools like decision trees or Markov models can simulate these scenarios to estimate long-term cost savings.
A critical caution in CEA is the time horizon. Vaccines often yield greater cost savings over decades, while antibodies provide immediate but temporary benefits. For example, a seasonal flu vaccine costing $20 may prevent $1,000 in healthcare costs annually, but an antibody treatment for a rare infection might cost $10,000 with limited long-term impact. Additionally, herd immunity from vaccines reduces overall disease burden, indirectly lowering costs for society, a factor absent in antibody therapies. Thus, CEA must account for both direct and indirect economic effects.
Persuasively, vaccines emerge as more cost-effective for population-level prevention due to their scalability and durability. However, antibodies have a niche role in high-risk groups or outbreaks where rapid protection is critical. For instance, during the Ebola outbreak, monoclonal antibodies were prioritized for healthcare workers despite high costs, as their protection was immediate and lifesaving. Policymakers should weigh these trade-offs, considering disease prevalence, population vulnerability, and healthcare infrastructure when allocating resources.
In conclusion, a CEA reveals that while antibodies offer targeted, short-term benefits, vaccines dominate in cost-effectiveness for broad, long-term protection. Practical tips include prioritizing vaccines for widespread immunization campaigns and reserving antibodies for specific high-risk scenarios. For example, a country with limited resources should invest in childhood vaccination programs (e.g., $15 per child for DTaP) rather than allocating funds to expensive antibody treatments ($1,000 per dose) for rare diseases. By balancing these interventions, healthcare systems can maximize health outcomes while minimizing costs.
Cat Vomiting After Vaccination? Quick Steps to Help Your Feline
You may want to see also
Explore related products






![]()
Side Effects and Safety Profiles
Antibodies, whether naturally produced or administered through therapies like monoclonal antibodies, carry distinct side effect and safety profiles compared to vaccines. While vaccines stimulate the immune system to produce its own antibodies with generally mild and transient side effects—such as soreness at the injection site, fatigue, or low-grade fever—antibody therapies introduce pre-formed proteins directly into the body. This bypasses the immune activation process but introduces risks like allergic reactions, anaphylaxis, or infusion-related symptoms, particularly in high-dose treatments. For instance, COVID-19 monoclonal antibody infusions have been associated with nausea, vomiting, and dizziness in up to 5% of recipients, requiring monitored administration settings.
Consider the age and health-specific implications: vaccines are rigorously tested across diverse populations, including children, pregnant individuals, and the elderly, with well-established safety data. Antibody therapies, however, often have narrower approval criteria. For example, COVID-19 monoclonal antibodies are typically recommended only for high-risk adults and adolescents, excluding younger children due to limited safety data. Vaccines, with their standardized dosing (e.g., 0.5 mL for Pfizer’s COVID-19 vaccine), offer predictable outcomes, whereas antibody dosages vary widely—from 500 mg to 4,000 mg depending on the condition and product—increasing the complexity of risk management.
A critical safety distinction lies in long-term effects. Vaccines, with decades of research behind them, have proven track records for safety beyond immediate side effects. Antibody therapies, particularly newer ones, lack this longitudinal data. For instance, while rare, there are concerns about antibody-dependent enhancement (ADE) in some viral infections, where antibodies may paradoxically worsen disease. Vaccines, by contrast, train the immune system holistically, reducing such risks. Practical tip: Always disclose pre-existing conditions like heart disease or allergies before receiving antibody therapies, as these may heighten adverse event risks.
Persuasively, the safety profile of vaccines aligns with their preventive role, making them a cornerstone of public health. Antibody therapies, while lifesaving in acute scenarios (e.g., severe COVID-19 or Ebola), are not substitutes for vaccination due to their transient nature and potential risks. A vaccinated individual may still require antibodies in emergencies, but relying solely on antibodies leaves one vulnerable without active immunity. For example, a 60-year-old with diabetes benefits more from a vaccine’s sustained protection than a single antibody infusion, which lasts only weeks to months.
Instructively, monitoring side effects is crucial for both interventions. Vaccines typically require only self-care post-administration, while antibody therapies demand observation for at least an hour post-infusion. Keep a symptom diary if you receive antibodies, noting any unusual reactions like rash, shortness of breath, or swelling. For vaccines, mild side effects can be managed with over-the-counter pain relievers (e.g., 650 mg acetaminophen every 4–6 hours), but severe reactions warrant immediate medical attention. Ultimately, while both tools combat disease, vaccines’ safety and preventive efficacy make them the gold standard, with antibodies reserved for targeted, high-risk scenarios.
Comirnaty Vaccine Availability in the United States: What You Need to Know
You may want to see also
Explore related products






![]()
Passive vs. Active Immunity Mechanisms
Antibodies and vaccines both play critical roles in protecting the body against pathogens, but they operate through distinct mechanisms: passive and active immunity. Understanding these differences is essential for evaluating whether antibodies can truly replace vaccines.
Passive immunity, the mechanism through which antibodies function, involves the direct transfer of pre-formed antibodies into the body. This can occur naturally, such as when a mother passes antibodies to her infant through breast milk, or artificially, via medical interventions like antibody injections. For instance, monoclonal antibody treatments for COVID-19 provide immediate protection by neutralizing the virus. However, this protection is short-lived, typically lasting weeks to months, as the body does not produce its own immune memory. Dosage is critical here; for example, COVID-19 monoclonal antibody treatments require a single infusion of 1,000–2,000 mg, depending on the specific antibody and patient weight. This approach is particularly useful for high-risk individuals or during outbreaks when immediate protection is needed.
In contrast, active immunity, induced by vaccines, stimulates the body’s own immune system to produce antibodies and memory cells. Vaccines introduce a harmless form of a pathogen (e.g., inactivated virus, mRNA, or viral vector) to trigger an immune response. For example, the Pfizer-BioNTech COVID-19 vaccine requires two doses of 30 µg each, administered 3–4 weeks apart, to build robust immunity. This process takes time—typically weeks—but results in long-lasting protection, often years or even a lifetime. Booster doses may be needed to maintain immunity, as seen with seasonal flu vaccines. Active immunity also confers immunological memory, enabling a faster and stronger response upon future exposure to the pathogen.
A key distinction lies in sustainability. Passive immunity is a temporary solution, ideal for urgent protection but impractical for long-term defense. Active immunity, on the other hand, is a durable investment in health, making it more cost-effective and logistically feasible for population-wide protection. For example, vaccinating children against measles at 12–15 months and again at 4–6 years provides lifelong immunity, whereas relying on antibody treatments would require repeated interventions.
Practical considerations further highlight the limitations of antibodies as a vaccine substitute. Antibody treatments are often expensive and require specialized administration, such as intravenous infusion. Vaccines, however, are generally administered via simple injections or nasal sprays, making them accessible even in resource-limited settings. Additionally, vaccines can prevent infection altogether, reducing transmission and protecting communities, while antibodies primarily treat or prevent severe disease in individuals.
In conclusion, while antibodies offer immediate protection through passive immunity, vaccines excel in providing long-term, cost-effective defense via active immunity. Each has its place in public health, but vaccines remain the cornerstone of disease prevention, offering both individual and collective benefits that antibodies cannot replicate.
Robert Malone's Vaccine Concerns: Insights and Controversies Explained
You may want to see also
Frequently asked questions
Vaccines stimulate the immune system to produce antibodies and memory cells, providing long-term protection. While antibodies (whether naturally acquired or via monoclonal antibody treatments) can offer immediate protection, they are generally short-lived compared to the durable immunity vaccines provide.
No, receiving antibodies from a recovered person (via convalescent plasma, for example) is not a substitute for vaccination. Vaccines train the immune system to recognize and fight the pathogen, whereas transferred antibodies offer temporary protection and do not create lasting immunity.
Monoclonal antibody treatments are used for prevention or treatment in specific cases, such as high-risk individuals or those with compromised immune systems. However, they do not replace vaccines, as vaccines provide broader and longer-lasting protection by activating the body’s own immune response.
Yes, vaccination is still recommended for individuals with natural antibodies from a previous infection. Vaccines provide a more robust and consistent immune response, reducing the risk of reinfection and severe disease, whereas natural immunity can vary widely in strength and duration.