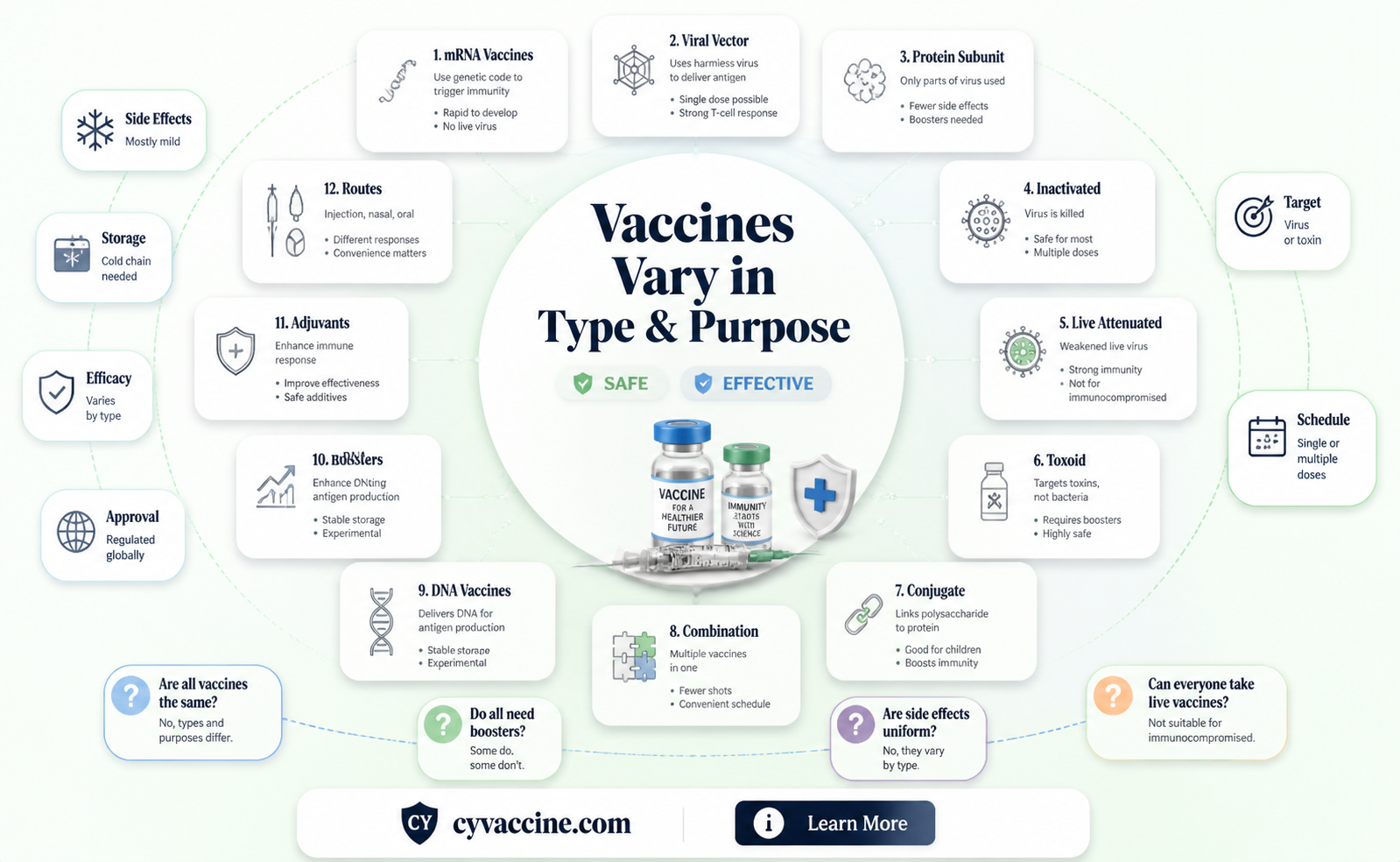
Vaccines are often perceived as a one-size-fits-all solution, but in reality, they are highly diverse in their composition, mechanisms, and purposes. While all vaccines aim to stimulate the immune system to protect against specific diseases, they differ significantly in their design, ingredients, and administration methods. For instance, some vaccines, like the mRNA vaccines used for COVID-19, deliver genetic instructions to cells, while others, such as inactivated or live-attenuated vaccines, use weakened or killed pathogens. Additionally, vaccines vary in their efficacy, side effects, and the duration of immunity they provide. Understanding these differences is crucial for appreciating why certain vaccines are recommended for specific populations, ages, or health conditions, and why not all vaccines can be treated interchangeably.
| Characteristics | Values |
|---|---|
| Type of Vaccine | mRNA (e.g., Pfizer-BioNTech, Moderna), Viral Vector (e.g., AstraZeneca, J&J), Protein Subunit (e.g., Novavax), Inactivated (e.g., Sinovac, Sinopharm) |
| Technology | mRNA vaccines use genetic material, viral vector uses modified viruses, protein subunit uses viral proteins, inactivated uses killed viruses |
| Efficacy Against Symptomatic Disease | mRNA: 90-95%, Viral Vector: 60-90%, Protein Subunit: ~90%, Inactivated: 50-80% (varies by study) |
| Efficacy Against Severe Disease/Hospitalization | All vaccines show high efficacy (80-100%) against severe disease and hospitalization |
| Dose Regimen | mRNA: 2 doses (3-4 weeks apart), Viral Vector: 1-2 doses, Protein Subunit: 2 doses, Inactivated: 2-3 doses |
| Storage Requirements | mRNA: Ultra-cold (-70°C to -20°C), Viral Vector: Standard refrigeration (2-8°C), Protein Subunit: Standard refrigeration, Inactivated: Standard refrigeration |
| Side Effects | Common: Pain at injection site, fatigue, headache, muscle pain, fever (severity varies by vaccine type) |
| Approval Status | Varies by country; mRNA and viral vector vaccines widely approved in Western countries, inactivated and protein subunit in others |
| Booster Recommendations | Boosters recommended for all types, especially mRNA, to maintain immunity against variants |
| Effectiveness Against Variants | mRNA and viral vector vaccines show reduced efficacy against some variants (e.g., Omicron), but still effective against severe disease |
| Cost | Varies by region and vaccine type; mRNA vaccines generally more expensive than inactivated or viral vector |
| Global Distribution | mRNA vaccines predominantly in high-income countries, inactivated and viral vector more widely distributed in low- and middle-income countries |
Explore related products


$11.93 $21.99




What You'll Learn
- Vaccine Types: Different vaccines (e.g., mRNA, viral vector, protein subunit) work uniquely in the body
- Efficacy Rates: Vaccines vary in effectiveness against infection, severe illness, and hospitalization
- Side Effects: Common side effects differ by vaccine type and individual immune response
- Dosage & Schedule: Number of doses and timing vary depending on the vaccine and age group
- Storage Requirements: Some vaccines need ultra-cold storage, while others are stable at standard refrigeration
![]()
Vaccine Types: Different vaccines (e.g., mRNA, viral vector, protein subunit) work uniquely in the body
Vaccines are not one-size-fits-all. Each type—whether mRNA, viral vector, or protein subunit—operates through distinct mechanisms to trigger immune responses. mRNA vaccines, like Pfizer-BioNTech and Moderna, deliver genetic instructions to cells, prompting them to produce a harmless spike protein that mimics the virus. This protein triggers the immune system to generate antibodies, preparing the body for future encounters with the actual virus. A typical mRNA vaccine regimen involves two doses, administered 3–4 weeks apart, with booster shots recommended for sustained immunity, especially in adults over 50 or immunocompromised individuals.
In contrast, viral vector vaccines, such as Johnson & Johnson and AstraZeneca, use a modified, harmless virus to transport genetic material into cells. This material instructs cells to create the viral protein, eliciting an immune response. Unlike mRNA vaccines, which require ultra-cold storage, viral vector vaccines are more stable and often require just a single dose, making them logistically advantageous in resource-limited settings. However, rare side effects like thrombosis with thrombocytopenia syndrome (TTS) have been reported, primarily in younger adults, prompting careful consideration of recipient age and health status.
Protein subunit vaccines, exemplified by Novavax, take a different approach by directly delivering a piece of the virus—often the spike protein—to the immune system. This method avoids introducing genetic material or live viruses, making it a safer option for individuals with specific allergies or concerns. Administered in two doses, spaced 3–4 weeks apart, protein subunit vaccines are particularly appealing for those hesitant about newer technologies. Their storage requirements are also less stringent, typically needing only standard refrigeration, which simplifies distribution.
Understanding these differences is crucial for informed decision-making. For instance, mRNA vaccines offer high efficacy rates (around 95% against severe disease), but their side effects, such as fatigue and muscle pain, are more pronounced after the second dose. Viral vector vaccines provide robust protection with fewer doses but carry a small risk of rare complications. Protein subunit vaccines combine safety and efficacy, making them suitable for broader populations, including pregnant individuals and those with compromised immune systems. Tailoring vaccine choice to individual needs ensures optimal protection while minimizing risks.
Practically, healthcare providers should educate patients about these distinctions, emphasizing that no single vaccine is universally superior. Factors like age, health status, and accessibility should guide selection. For example, a young, healthy adult in a remote area might benefit from a single-dose viral vector vaccine, while an elderly individual with chronic conditions may prefer the high efficacy of an mRNA option. By demystifying vaccine types, we empower individuals to make choices aligned with their health priorities and circumstances.
Aaron Rodgers' COVID-19 Vaccination Status: The Real Story
You may want to see also
Explore related products





![]()
Efficacy Rates: Vaccines vary in effectiveness against infection, severe illness, and hospitalization
Vaccines are not one-size-fits-all solutions. Their efficacy rates—the measure of how well they prevent infection, severe illness, and hospitalization—vary widely depending on the vaccine type, the pathogen it targets, and the population receiving it. For instance, the Pfizer-BioNTech COVID-19 vaccine demonstrated 95% efficacy against symptomatic infection in clinical trials, while the Johnson & Johnson vaccine showed 66% efficacy globally. These differences highlight the importance of understanding what each vaccine is designed to achieve.
Consider the influenza vaccine, which is reformulated annually to match circulating strains. Its efficacy typically ranges between 40% and 60%, yet it remains a critical tool in reducing hospitalizations and deaths, especially among high-risk groups like the elderly and immunocompromised. In contrast, the measles vaccine boasts an impressive 97% efficacy after two doses, providing near-complete protection against infection and severe complications. These examples illustrate how efficacy rates are not just numbers but reflect the vaccine’s ability to meet specific health goals.
When evaluating vaccine efficacy, it’s crucial to distinguish between prevention of infection and prevention of severe outcomes. For example, the Moderna COVID-19 vaccine showed 94% efficacy against symptomatic infection but even higher protection—over 98%—against severe illness and hospitalization. This distinction matters in public health strategies, as vaccines with lower infection prevention rates can still significantly reduce the burden on healthcare systems by minimizing severe cases.
Practical considerations also play a role in vaccine effectiveness. Dosage and administration schedules can impact outcomes. The Pfizer-BioNTech vaccine requires two doses, 21 days apart, for optimal protection, while the AstraZeneca vaccine’s efficacy increases from 70% to 82% when the second dose is delayed by 12 weeks. Age is another factor; some vaccines, like the shingles vaccine Shingrix, are specifically formulated for older adults, with efficacy rates exceeding 90% in those over 50. Always follow the recommended schedule and dosage for maximum benefit.
In summary, vaccines are not interchangeable in their efficacy profiles. Understanding these differences empowers individuals and healthcare providers to make informed decisions. Whether it’s choosing the right vaccine for a specific age group or interpreting efficacy data, recognizing these variations ensures vaccines are used effectively to protect public health.
Puerto Rico's COVID-19 Vaccination Requirements: Understanding Fully Vaccinated Status
You may want to see also
Explore related products






![]()
Side Effects: Common side effects differ by vaccine type and individual immune response
Vaccines, while sharing a common goal of disease prevention, are not one-size-fits-all solutions. Their side effects vary widely, influenced by both the vaccine’s design and the recipient’s immune system. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna, which teach cells to produce a harmless protein triggering an immune response, often cause fatigue, headache, and muscle pain in over 50% of recipients after the second dose. In contrast, viral vector vaccines such as Johnson & Johnson may lead to rare but serious side effects like thrombosis with thrombocytopenia syndrome (TTS), occurring in approximately 7 per 1 million vaccinated women aged 18–49. Understanding these differences is crucial for informed decision-making and managing expectations.
Consider the influenza vaccine, which uses inactivated viruses and typically causes milder reactions, such as soreness at the injection site or low-grade fever, in less than 20% of recipients. This contrasts sharply with the live attenuated shingles vaccine (Shingrix), where over 50% of adults experience substantial arm pain, fatigue, and even fever for 2–3 days post-vaccination. Age plays a significant role here: older adults, whose immune systems may respond more vigorously, often report more pronounced side effects. For example, a 70-year-old receiving Shingrix might need to plan for a day of rest after vaccination, while a 30-year-old may experience minimal disruption.
Individual immune responses further complicate the picture. Factors like genetics, pre-existing conditions, and even stress levels can influence how one reacts to a vaccine. For instance, someone with a history of allergies might be more prone to localized reactions, while another with an autoimmune disorder could experience amplified systemic symptoms. Practical tips include staying hydrated, applying a cool compress to injection sites, and scheduling vaccinations during periods of lower stress to mitigate discomfort. Always consult a healthcare provider if side effects persist beyond 48 hours or worsen.
Comparing COVID-19 vaccines highlights these disparities further. The AstraZeneca vaccine, another viral vector type, has been linked to rare cases of vaccine-induced immune thrombotic thrombocytopenia (VITT), primarily in younger adults. Meanwhile, Novavax, a protein subunit vaccine, tends to cause less systemic reactions, with only 10–20% of recipients reporting fatigue or headaches. Dosage also matters: pediatric COVID-19 vaccines contain one-third the dosage of adult formulations, reducing side effect severity in children aged 5–11. This tailored approach underscores the importance of vaccine-specific guidelines and individualized care.
In conclusion, while vaccines share the purpose of disease prevention, their side effects are far from uniform. Recognizing these differences empowers individuals to prepare for potential reactions and fosters trust in vaccination programs. Whether it’s planning for post-vaccination rest or understanding rare risks, knowledge of these variations ensures a smoother experience. Always follow healthcare provider instructions and report unusual symptoms promptly, ensuring both safety and efficacy in immunization efforts.
Get Vaccinated, Get Paid: Cities Offering $100 Incentives Revealed
You may want to see also
Explore related products






![]()
Dosage & Schedule: Number of doses and timing vary depending on the vaccine and age group
Vaccines are not one-size-fits-all, and their dosage and scheduling requirements can differ significantly based on the type of vaccine and the recipient's age. For instance, the COVID-19 vaccines from Pfizer-BioNTech, Moderna, and Johnson & Johnson each have distinct protocols. Pfizer and Moderna require two doses, typically administered 3–4 weeks apart for Pfizer and 4–6 weeks apart for Moderna, while Johnson & Johnson is a single-dose vaccine. These variations are designed to optimize immune response and protection levels, highlighting the importance of following specific guidelines for each vaccine.
Age groups further complicate dosage and scheduling. Children, adolescents, and adults often receive vaccines at different intervals and in varying amounts. For example, the HPV vaccine (Gardasil 9) is given in a two-dose series for individuals aged 9–14, but those aged 15–26 require three doses over 6 months. Similarly, the influenza vaccine dosage differs for children under 9, who may need two doses in their first year of vaccination, compared to a single annual dose for older individuals. These age-specific schedules ensure that immune systems at different developmental stages receive the appropriate protection.
Practical considerations also play a role in adhering to vaccine schedules. Missed doses or delays can occur due to illness, scheduling conflicts, or lack of access. In such cases, healthcare providers often follow catch-up schedules, which may involve restarting the series or adjusting intervals. For example, if the second dose of the Pfizer COVID-19 vaccine is delayed beyond the recommended 3 weeks, it can still be administered up to 6 weeks later without restarting the series. However, prolonged delays may reduce efficacy, emphasizing the need for timely administration.
Understanding these variations is crucial for both healthcare providers and recipients. Parents should consult vaccination records and healthcare professionals to ensure their children are up to date, while adults must prioritize scheduling and follow-through. Digital tools, such as vaccine reminder apps or immunization registries, can help track doses and due dates. Ultimately, adherence to specific dosage and timing guidelines maximizes the effectiveness of vaccines, safeguarding individuals and communities against preventable diseases.
Survivor Show: Vaccination Requirements for Contestants
You may want to see also
Explore related products






![]()
Storage Requirements: Some vaccines need ultra-cold storage, while others are stable at standard refrigeration
Vaccines are not one-size-fits-all, especially when it comes to storage. While some, like the measles-mumps-rubella (MMR) vaccine, remain stable at standard refrigerator temperatures (2°C to 8°C), others demand ultra-cold conditions. For instance, the Pfizer-BioNTech COVID-19 vaccine requires storage at -70°C ±10°C, a logistical challenge for many healthcare systems. This stark contrast in storage needs highlights the complexity of vaccine distribution and administration, particularly in resource-limited settings.
Consider the practical implications: a rural clinic with limited access to ultra-cold freezers may struggle to administer vaccines like Pfizer’s, whereas the Moderna COVID-19 vaccine, stable at -20°C, offers more flexibility. Similarly, the Oxford-AstraZeneca vaccine can be stored at standard refrigeration temperatures, making it a more viable option for widespread distribution. These differences underscore the importance of matching vaccine selection to available infrastructure, ensuring that doses remain effective from production to injection.
From a logistical standpoint, ultra-cold storage requirements introduce significant costs and complexities. Specialized equipment, such as dry ice or liquid nitrogen freezers, is expensive and not universally available. For example, transporting the Pfizer vaccine involves meticulous planning, including the use of GPS-enabled thermal shipping containers and dry ice replenishment every five days. In contrast, vaccines stable at standard refrigeration, like the annual influenza vaccine, can be stored in basic medical refrigerators, reducing both cost and operational burden.
For healthcare providers, understanding these storage requirements is critical. Improper storage can render vaccines ineffective, wasting resources and compromising immunity. The World Health Organization (WHO) provides guidelines, such as the "Vaccine Storage and Handling Toolkit," to assist in maintaining proper conditions. For instance, vaccines stored at ultra-cold temperatures must be thawed carefully, often at 2°C to 25°C for a limited time, before administration. Standard refrigeration vaccines, however, can be used directly from the fridge, simplifying the process.
In conclusion, storage requirements are a defining factor in vaccine accessibility and efficacy. While ultra-cold storage vaccines push the boundaries of scientific innovation, they also demand advanced infrastructure. Vaccines stable at standard refrigeration, on the other hand, offer practicality and scalability, particularly in low-resource settings. By tailoring vaccine selection to storage capabilities, healthcare systems can maximize impact, ensuring that life-saving doses reach those who need them most.
CDC Vaccination Concerns: Exploring Alternatives and Informed Choices
You may want to see also
Frequently asked questions
No, vaccines are not all the same. They vary in composition based on the disease they target, the type of vaccine (e.g., mRNA, viral vector, inactivated virus), and the specific ingredients used to ensure safety and efficacy.
No, the level of protection varies depending on the vaccine, the individual’s immune response, and the disease being prevented. Some vaccines offer near-complete immunity, while others reduce severity or transmission risk.
No, side effects differ among vaccines. Common side effects like soreness, fatigue, or fever can vary in frequency and intensity based on the vaccine type and the person receiving it.
No, the number of doses needed varies. Some vaccines require a single dose, while others need multiple doses or boosters to provide full protection.
No, vaccines are developed using different technologies, such as mRNA (e.g., Pfizer, Moderna), viral vectors (e.g., Johnson & Johnson, AstraZeneca), inactivated viruses, or protein subunits, depending on the disease and desired immune response.