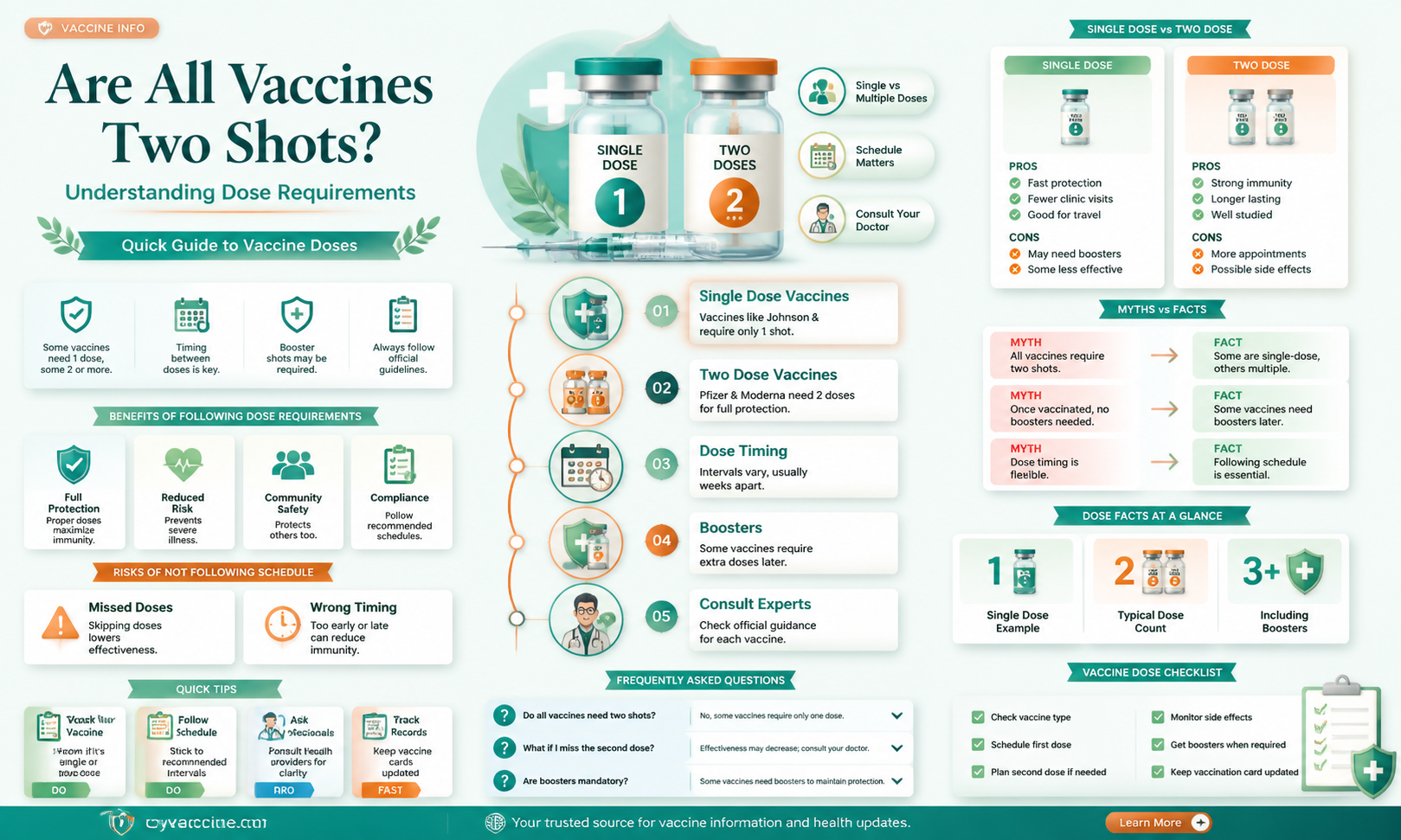
Not all vaccines require two shots; the number of doses needed varies depending on the type of vaccine and the disease it targets. Some vaccines, like the COVID-19 mRNA vaccines (Pfizer and Moderna), typically require two doses for full protection, while others, such as the Johnson & Johnson COVID-19 vaccine, are administered as a single shot. Similarly, childhood vaccines like MMR (measles, mumps, rubella) often require two doses, whereas the flu vaccine is usually given annually in one dose. Booster shots may also be recommended for certain vaccines to maintain immunity over time. The specific dosing schedule is determined by scientific research and public health guidelines to ensure optimal effectiveness and safety.
Explore related products






What You'll Learn
- Single-dose vaccines: Some vaccines require only one shot for full immunity
- Booster shots: Additional doses may be needed for prolonged protection
- Vaccine schedules: Timing between doses varies by vaccine type
- Mixed dosing: Combining different vaccines for optimal immunity
- Vaccine efficacy: Protection levels differ after one or two shots
![]()
Single-dose vaccines: Some vaccines require only one shot for full immunity
Not all vaccines follow the two-shot regimen that has become familiar in recent years. Single-dose vaccines, designed to confer full immunity with just one administration, play a critical role in public health strategies. For instance, the Johnson & Johnson COVID-19 vaccine is a notable example, offering robust protection against severe disease with a single 0.5 mL intramuscular injection for individuals aged 18 and older. This approach simplifies logistics, reduces healthcare burden, and improves compliance, particularly in populations with limited access to medical facilities or those hesitant to return for a second dose.
The efficacy of single-dose vaccines hinges on their formulation and the immune response they elicit. Unlike multi-dose vaccines, which build immunity gradually through repeated exposure to antigens, single-dose vaccines often incorporate adjuvants or higher antigen concentrations to stimulate a strong, lasting immune response immediately. For example, the yellow fever vaccine, a live-attenuated virus administered as a single 0.5 mL dose, provides lifelong immunity for most recipients after just one shot. This makes it a cornerstone of travel medicine and outbreak control in endemic regions.
Single-dose vaccines are particularly advantageous in emergency or resource-constrained settings. During disease outbreaks, such as Ebola, single-dose vaccines like the rVSV-ZEBOV vaccine have been deployed to rapidly protect at-risk populations. This vaccine, administered as a single 1 mL injection, achieved over 90% efficacy in clinical trials, demonstrating the power of this approach in crisis situations. Similarly, childhood immunization programs often include single-dose vaccines, such as the measles vaccine, which is typically given as a 0.5 mL dose to children around 12 months of age, ensuring widespread protection with minimal logistical complexity.
Practical considerations for single-dose vaccines include proper storage, administration technique, and patient education. Many single-dose vaccines, like the Johnson & Johnson COVID-19 vaccine, require refrigeration at 2°C to 8°C, while others, such as the yellow fever vaccine, must be stored in a freezer until reconstitution. Healthcare providers must ensure accurate dosing and injection site selection to maximize efficacy and minimize adverse effects. Patients should be informed about potential side effects, which are generally mild to moderate, and encouraged to monitor their health post-vaccination. For travelers receiving single-dose vaccines like yellow fever, carrying an International Certificate of Vaccination is essential for compliance with entry requirements in certain countries.
In conclusion, single-dose vaccines represent a vital tool in the immunization arsenal, offering efficient, effective protection against a range of diseases. Their simplicity and convenience make them ideal for diverse populations and scenarios, from routine childhood immunizations to emergency outbreak responses. Understanding their unique characteristics and proper administration ensures their optimal use, contributing to global health security and individual well-being.
FDA Research: Vaccinated vs. Unvaccinated Kids - What's the Truth?
You may want to see also
Explore related products






![]()
Booster shots: Additional doses may be needed for prolonged protection
Not all vaccines follow a strict two-shot regimen. While many, like the Pfizer-BioNTech and Moderna COVID-19 vaccines, initially require two doses spaced weeks apart, the concept of booster shots has become increasingly crucial for maintaining immunity. Booster shots are additional doses administered after the initial series to "boost" the immune response that may have waned over time. This is particularly relevant for vaccines targeting rapidly evolving viruses or those where immunity naturally declines.
For instance, the COVID-19 pandemic highlighted the need for boosters. Studies showed that while the initial two doses provided robust protection against severe illness and hospitalization, their effectiveness against infection and mild illness diminished over 6-12 months. This led health authorities to recommend booster shots, typically a single dose, for individuals aged 12 and older, with specific intervals varying depending on the initial vaccine received.
The necessity of boosters extends beyond COVID-19. Vaccines like the Tdap (Tetanus, Diphtheria, and Pertussis) require periodic boosters throughout life, typically every 10 years, to maintain immunity against these potentially serious diseases. Similarly, the shingles vaccine, Shingrix, involves a two-dose series followed by a booster shot after several years to ensure continued protection, especially in older adults who are more susceptible to shingles.
The timing and frequency of booster shots are carefully determined through scientific research and ongoing monitoring of vaccine effectiveness. Factors like the specific disease, the vaccine's mechanism of action, and individual risk factors all play a role in these recommendations. It's crucial to consult with healthcare professionals to understand the booster schedule appropriate for your specific needs and medical history.
While the idea of additional shots might seem inconvenient, booster doses are a vital tool in maintaining long-term immunity and protecting against preventable diseases. They represent a proactive approach to public health, ensuring that our bodies remain equipped to fight off pathogens effectively. Staying informed about recommended booster schedules and adhering to them is a responsible step towards safeguarding both individual and community health.
London's Vaccination Rules: What Travelers Need to Know
You may want to see also
Explore related products






![]()
Vaccine schedules: Timing between doses varies by vaccine type
Not all vaccines follow a uniform two-dose regimen. The timing and number of doses required for optimal immunity vary significantly depending on the vaccine type, the disease it targets, and the recipient's age and health status. For instance, the COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) typically require two doses administered 3–4 weeks apart for individuals aged 12 and older, while the Johnson & Johnson viral vector vaccine is a single-dose regimen. In contrast, the HPV vaccine (Gardasil 9) follows a two- or three-dose schedule depending on the recipient’s age at the initial vaccination: those under 15 need two doses 6–12 months apart, while those 15 and older require three doses over 6 months. This variability underscores the importance of understanding vaccine-specific schedules to ensure maximum protection.
The rationale behind these differing schedules lies in the vaccines' mechanisms and the immune response they elicit. For example, the hepatitis B vaccine often requires three doses over 6 months to establish long-term immunity, particularly in infants and young children. Similarly, the shingles vaccine (Shingrix) demands two doses 2–6 months apart to effectively protect older adults, whose immune systems may be less responsive. In some cases, booster doses are necessary to maintain immunity, such as with the Tdap vaccine (tetanus, diphtheria, and pertussis), which requires a booster every 10 years. These schedules are meticulously designed based on clinical trial data to balance efficacy, safety, and practicality.
Age is a critical factor in determining vaccine schedules. Pediatric vaccines, such as those for measles, mumps, and rubella (MMR), are typically administered in two doses: the first at 12–15 months and the second at 4–6 years. This timing aligns with the maturation of the immune system and the waning of maternal antibodies. In contrast, adult vaccines often have longer intervals between doses to accommodate slower immune responses. For travelers, accelerated schedules may be recommended for vaccines like hepatitis A, which can be given in two doses 6–12 months apart, but an initial dose can provide short-term protection if travel is imminent.
Practical considerations also influence vaccine schedules. For example, the influenza vaccine is administered annually due to the virus's rapid mutation and the waning of immunity over time. On the other hand, the rabies vaccine is given in a series of four doses over 14 days in the event of exposure, a schedule designed to rapidly neutralize the virus before it causes disease. Adhering to these schedules is crucial, as deviations can compromise immunity. If a dose is missed, healthcare providers often follow catch-up schedules, which may involve restarting the series or adjusting intervals based on the specific vaccine.
In summary, vaccine schedules are not one-size-fits-all. They are tailored to the unique characteristics of each vaccine, the target population, and the disease being prevented. Understanding these variations is essential for both healthcare providers and recipients to ensure timely and effective immunization. Always consult vaccine-specific guidelines or a healthcare professional to confirm the appropriate schedule, as deviations can reduce protection. By respecting these schedules, individuals can maximize the benefits of vaccination and contribute to public health.
MSC Cruise: Vaccination Requirements and Protocols
You may want to see also
Explore related products






![]()
Mixed dosing: Combining different vaccines for optimal immunity
Not all vaccines follow the traditional two-shot regimen, and this variability has sparked interest in mixed dosing—a strategy where different vaccines are combined to enhance immune response. For instance, the COVID-19 pandemic introduced heterologous prime-boost schedules, such as receiving AstraZeneca’s viral vector vaccine as the first dose and Pfizer’s mRNA vaccine as the second. Studies show this approach can elicit higher antibody levels and broader immune memory compared to homologous dosing (same vaccine twice). This isn’t limited to COVID-19; countries like Canada and the UK have adopted mixed schedules for other vaccines, such as HPV, where a lower dose of Cervarix (adjuvanted) followed by Gardasil (non-adjuvanted) provides robust protection with fewer doses.
The science behind mixed dosing lies in leveraging the strengths of different vaccine platforms. Viral vector vaccines excel at stimulating T-cell responses, while mRNA vaccines produce high levels of neutralizing antibodies. Combining these can create a more comprehensive immune profile. For example, a study in *The Lancet* found that a mixed COVID-19 regimen increased antibody titers by up to 200% compared to two doses of AstraZeneca alone. However, this approach requires careful consideration of timing and dosage. For adults aged 18–65, a 4-week interval between doses is optimal for mixed COVID-19 vaccines, balancing immune response and minimizing side effects like fatigue or fever.
Implementing mixed dosing isn’t without challenges. Regulatory bodies must approve specific combinations, and healthcare providers need clear guidelines. For instance, the World Health Organization (WHO) recommends mixed dosing for COVID-19 only when the same vaccine is unavailable. Practical tips include ensuring patients receive accurate documentation of their vaccine type and date, as this affects booster eligibility. Additionally, pregnant individuals or those with compromised immunity should consult a healthcare provider, as mixed dosing may require adjustments based on individual health status.
Comparatively, mixed dosing offers a flexible solution in resource-constrained settings. During vaccine shortages, combining available vaccines can maintain immunization coverage. For example, in low-income countries, a single dose of Johnson & Johnson followed by a dose of Pfizer has been used to accelerate vaccination campaigns. This adaptability highlights the potential of mixed dosing beyond emergency scenarios, such as optimizing flu vaccine regimens for elderly populations, who often respond poorly to standard doses.
In conclusion, mixed dosing represents a strategic shift in vaccination, moving beyond the one-size-fits-all approach. By combining vaccines, we can tailor immune responses to specific populations or diseases. While research is ongoing, early evidence suggests this method could enhance efficacy, reduce side effects, and improve accessibility. As vaccine technology evolves, mixed dosing may become a cornerstone of immunization strategies, offering a nuanced way to achieve optimal immunity.
Verify Your Vaccine Record with NADRA in Pakistan: A Guide
You may want to see also
Explore related products






![]()
Vaccine efficacy: Protection levels differ after one or two shots
Not all vaccines require two shots, but for those that do, the difference in protection levels between one and two doses can be significant. This is particularly evident in mRNA vaccines like Pfizer-BioNTech and Moderna, where the second dose acts as a booster, significantly enhancing immune response. Studies show that after the first dose, Pfizer’s vaccine offers approximately 52% efficacy against symptomatic COVID-19, while the second dose elevates this to around 95%. Moderna’s first dose provides roughly 80% protection, with the second dose pushing it to over 94%. These numbers underscore the critical role of completing the full vaccine series for optimal immunity.
The timing between doses also plays a crucial role in vaccine efficacy. For Pfizer, the recommended interval is 3 to 4 weeks, while Moderna allows for a longer gap of 4 to 6 weeks. Deviating from these schedules can impact the immune response, as the second dose relies on the priming effect of the first. For instance, delaying the second dose beyond the recommended timeframe may reduce the initial spike in antibodies, though it doesn’t negate the overall benefit. However, adhering to the prescribed schedule ensures the highest level of protection, particularly against emerging variants.
Age and health status further influence how individuals respond to one or two doses. Younger, healthier populations often mount a robust immune response after a single dose, while older adults or immunocompromised individuals may require the full series to achieve comparable protection. For example, data from Israel’s vaccination campaign revealed that while one dose provided substantial protection for younger adults, those over 65 needed both doses to significantly reduce hospitalizations and severe illness. This highlights the importance of tailored vaccination strategies based on demographic and health factors.
Practical considerations also come into play when deciding between one or two doses. In resource-limited settings or during vaccine shortages, prioritizing a single dose for a larger population can provide immediate, albeit partial, protection. However, this approach must be balanced against the long-term benefits of full vaccination. For individuals, ensuring access to the second dose is essential, as partial immunity may lead to complacency and increased risk of infection. Scheduling reminders, transportation assistance, and clear communication about the importance of the second dose can help improve compliance and maximize vaccine efficacy.
In conclusion, while not all vaccines require two shots, those that do demonstrate a clear disparity in protection levels between one and two doses. Completing the full series is vital for achieving optimal immunity, particularly in the context of mRNA vaccines. Factors like dosing intervals, age, and health status further shape the effectiveness of vaccination, emphasizing the need for personalized and strategic approaches. By understanding these nuances, individuals and healthcare systems can make informed decisions to ensure the broadest and most effective protection against infectious diseases.
J&J Vaccine Shortage: Reasons Behind the Scarcity Explained
You may want to see also
Frequently asked questions
No, not all vaccines require two shots. Some vaccines are administered as a single dose, while others may require multiple doses depending on the type of vaccine and the disease it prevents.
Some vaccines require two shots to build a stronger and longer-lasting immune response. The first shot primes the immune system, and the second shot boosts immunity to provide better protection against the disease.
It depends on the vaccine. Some vaccines, like the Johnson & Johnson COVID-19 vaccine, provide full protection with a single dose. Others, like the Pfizer and Moderna COVID-19 vaccines, require two doses for optimal protection.
Missing the second shot may reduce the vaccine’s effectiveness. It’s important to follow the recommended schedule, but if you miss a dose, consult your healthcare provider to determine the best course of action.
Yes, some vaccines require multiple doses beyond two shots. For example, the HPV vaccine is often given in a series of two or three doses, depending on the age of the recipient. Always follow the specific guidelines for the vaccine you’re receiving.