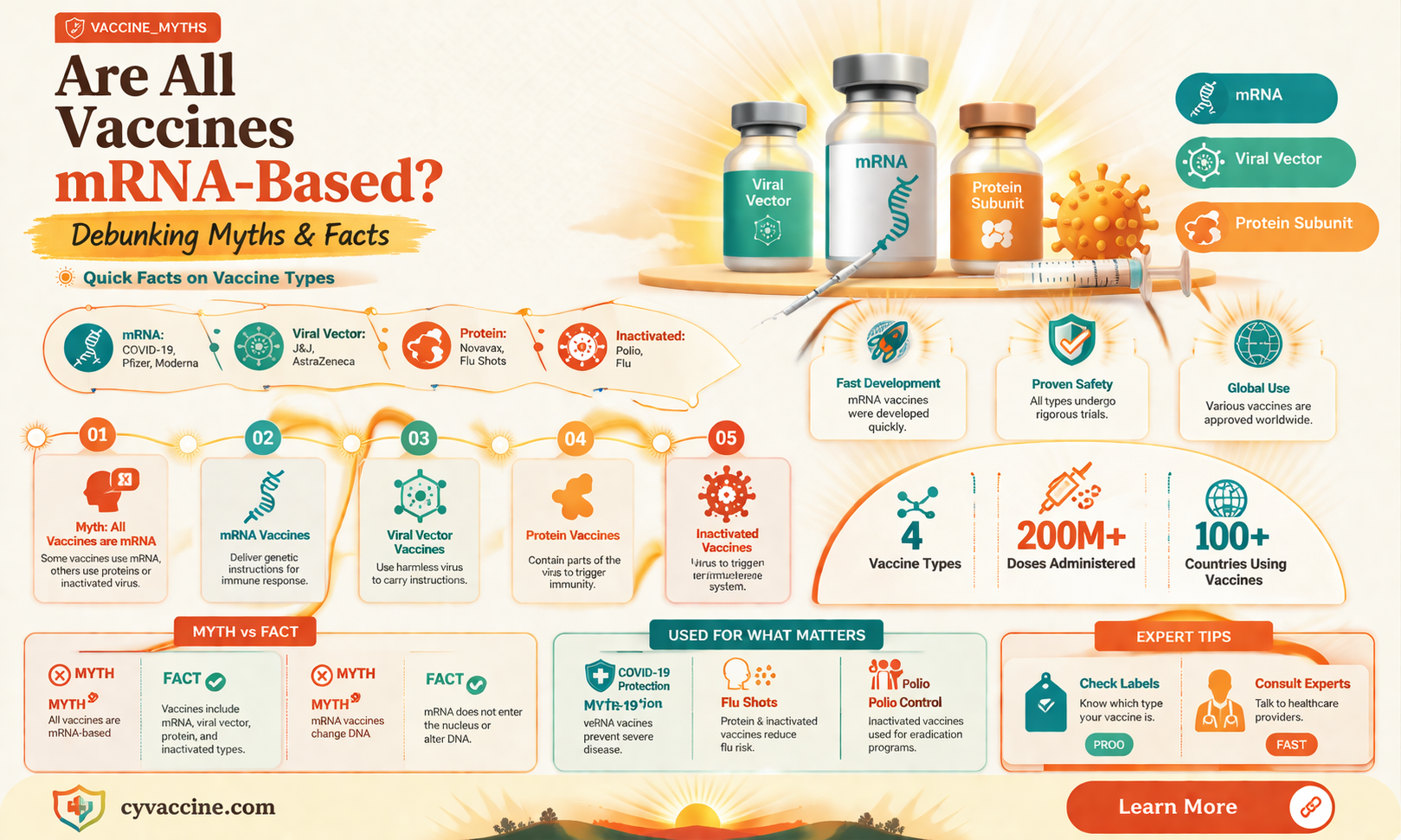
The question of whether all vaccines are made with mRNA is a common one, especially given the prominence of mRNA technology in recent COVID-19 vaccines. However, it’s important to clarify that not all vaccines utilize mRNA (messenger RNA). Vaccines are developed using various technologies, including inactivated or weakened viruses, viral vectors, protein subunits, and toxoids, among others. mRNA vaccines, such as those produced by Pfizer-BioNTech and Moderna, represent a relatively new approach that instructs cells to produce a harmless protein triggering an immune response. While mRNA vaccines have gained significant attention for their efficacy and rapid development, they are just one of several vaccine platforms, each designed to address specific diseases and immune responses. Understanding the diversity of vaccine technologies is crucial for appreciating how different vaccines work and their roles in global health.
| Characteristics | Values |
|---|---|
| Are all vaccines made with mRNA? | No |
| Types of vaccines that use mRNA technology | COVID-19 vaccines (e.g., Pfizer-BioNTech, Moderna) |
| Types of vaccines that do not use mRNA technology | Inactivated vaccines (e.g., Sinopharm, Sinovac), viral vector vaccines (e.g., AstraZeneca, Johnson & Johnson), protein subunit vaccines (e.g., Novavax), live attenuated vaccines (e.g., MMR), toxoid vaccines (e.g., Tetanus), conjugate vaccines (e.g., Pneumococcal), polysaccharide vaccines (e.g., Meningococcal) |
| mRNA vaccine mechanism | Delivers genetic material (mRNA) to cells, instructing them to produce a harmless piece of the virus (spike protein), triggering an immune response |
| Non-mRNA vaccine mechanisms | Introduce a weakened or inactivated form of the virus, viral proteins, or toxins to stimulate an immune response |
| Stability of mRNA vaccines | Requires ultra-cold storage for some (e.g., Pfizer-BioNTech), while others are more stable (e.g., Moderna) |
| Stability of non-mRNA vaccines | Generally more stable and easier to store and transport |
| Development time for mRNA vaccines | Faster development and production compared to traditional vaccines |
| Development time for non-mRNA vaccines | Longer development and production timelines |
| Examples of diseases targeted by mRNA vaccines | COVID-19, currently under research for influenza, Zika, and cancer |
| Examples of diseases targeted by non-mRNA vaccines | Influenza, measles, mumps, rubella, polio, tetanus, diphtheria, pertussis, hepatitis B, human papillomavirus (HPV), and many others |
| Regulatory approvals for mRNA vaccines | Pfizer-BioNTech and Moderna COVID-19 vaccines approved by WHO, FDA, EMA, and other regulatory bodies |
| Regulatory approvals for non-mRNA vaccines | Numerous vaccines approved by regulatory bodies worldwide for various diseases |
Explore related products



$23.58 $32.99

$18.99 $18.99


What You'll Learn
- Traditional vs. mRNA Vaccines: Comparing conventional vaccine technologies with newer mRNA-based approaches in development and efficacy
- mRNA Vaccine Examples: Highlighting specific vaccines like Pfizer-BioNTech and Moderna that use mRNA technology
- Non-mRNA Vaccines: Discussing vaccines made with inactivated viruses, proteins, or viral vectors, not mRNA
- mRNA Vaccine Safety: Addressing safety profiles, side effects, and long-term studies of mRNA vaccines
- Future of mRNA Vaccines: Exploring potential applications of mRNA technology beyond COVID-19, like cancer or flu vaccines
![]()
Traditional vs. mRNA Vaccines: Comparing conventional vaccine technologies with newer mRNA-based approaches in development and efficacy
Not all vaccines are made with mRNA technology; in fact, the majority of vaccines used today rely on traditional methods that have been refined over decades. Conventional vaccines typically use weakened or inactivated pathogens, parts of pathogens (like proteins or sugars), or toxoids to stimulate an immune response. For example, the flu vaccine contains inactivated influenza viruses, while the tetanus vaccine uses a toxoid to neutralize the harmful effects of the toxin produced by the bacteria. These vaccines have proven effective in preventing diseases like measles, mumps, polio, and hepatitis B, often requiring multiple doses to build and maintain immunity. For instance, the MMR vaccine (measles, mumps, rubella) is administered in two doses, typically at 12–15 months and 4–6 years of age, to ensure robust protection.
In contrast, mRNA vaccines represent a newer approach that leverages genetic material to instruct cells to produce a specific protein, triggering an immune response. The COVID-19 vaccines developed by Pfizer-BioNTech and Moderna are prime examples of this technology. Unlike traditional vaccines, mRNA vaccines do not contain live or inactivated pathogens, reducing the risk of adverse reactions. They also offer faster development timelines, as seen during the pandemic, where mRNA vaccines were authorized for emergency use within a year of the virus’s identification. However, mRNA vaccines often require ultra-cold storage (e.g., -70°C for Pfizer’s vaccine) and may necessitate multiple doses, such as the two-dose primary series for COVID-19, followed by boosters to maintain efficacy against evolving variants.
One key advantage of mRNA technology is its adaptability. Because it relies on delivering genetic instructions, mRNA vaccines can be rapidly redesigned to target new pathogens or variants. For instance, updated COVID-19 boosters were developed within months to address the Omicron variant. Traditional vaccines, on the other hand, often require more time-consuming processes, such as culturing viruses or bacteria, which can delay responses to emerging threats. However, mRNA vaccines are not without challenges; their novelty means long-term efficacy and safety data are still being collected, and their higher production costs can limit accessibility in low-resource settings.
Efficacy comparisons between traditional and mRNA vaccines highlight both strengths and limitations. Traditional vaccines have a well-established track record, with some, like the smallpox vaccine, achieving global eradication of the disease. mRNA vaccines, while newer, have demonstrated remarkable efficacy in clinical trials, with Pfizer’s COVID-19 vaccine showing 95% effectiveness against symptomatic infection in initial studies. However, real-world effectiveness can vary due to factors like waning immunity and viral mutations. For example, COVID-19 mRNA vaccines remain highly effective against severe disease and hospitalization but offer reduced protection against infection over time, necessitating boosters.
Practical considerations also differentiate these approaches. Traditional vaccines are generally more stable and easier to distribute, making them suitable for widespread immunization campaigns, such as those for polio or measles. mRNA vaccines, despite their logistical challenges, offer a promising platform for addressing diseases where traditional methods have fallen short, such as HIV or malaria. For individuals, understanding these differences can inform vaccine choices, particularly for those with specific health concerns or living in areas with limited access to advanced storage facilities. As mRNA technology continues to evolve, it may complement, rather than replace, traditional vaccines, providing a diverse toolkit to combat infectious diseases globally.
RTS,S Vaccine: Unique Features Compared to Traditional Vaccines
You may want to see also
Explore related products






![]()
mRNA Vaccine Examples: Highlighting specific vaccines like Pfizer-BioNTech and Moderna that use mRNA technology
Not all vaccines are made with mRNA technology, but those that are have revolutionized the field of immunology, particularly in response to the COVID-19 pandemic. Among the most prominent examples are the Pfizer-BioNTech and Moderna vaccines, both of which utilize mRNA to elicit an immune response. These vaccines work by delivering genetic material that instructs cells to produce a harmless piece of the virus’s spike protein, triggering the body to build immunity. Unlike traditional vaccines, which use weakened or inactivated viruses, mRNA vaccines do not alter human DNA and are rapidly degradable once their task is complete.
The Pfizer-BioNTech COVID-19 vaccine, authorized for emergency use in December 2020, is administered in a two-dose series, typically 21 days apart. For individuals aged 12 and older, each dose contains 30 micrograms of mRNA. In children aged 5–11, the dosage is reduced to 10 micrograms per shot, reflecting differences in immune response and safety considerations. A booster dose is recommended for those aged 12 and older, particularly for enhanced protection against variants. Practical tips include scheduling doses well in advance and monitoring for common side effects like fatigue, headache, and injection site pain, which are typically mild and short-lived.
Moderna’s mRNA-1273 vaccine follows a similar mechanism but with some key differences. It is administered in two doses, 28 days apart, with each dose containing 100 micrograms of mRNA for individuals aged 18 and older. A half-dose (50 micrograms) booster is recommended for continued immunity. Moderna’s vaccine has been particularly noted for its efficacy in preventing severe disease, even against emerging variants. For those with compromised immune systems, an additional third primary dose may be advised before considering a booster. Side effects are comparable to Pfizer’s vaccine but may be slightly more pronounced due to the higher mRNA content.
Comparing the two, Pfizer-BioNTech’s vaccine is more widely used globally, partly due to its earlier approval and broader age range (down to age 5). Moderna’s vaccine, while equally effective, is often prioritized for adults and has been a key player in booster campaigns. Both vaccines have demonstrated remarkable success in reducing hospitalizations and deaths, underscoring the power of mRNA technology. Their rapid development and deployment highlight the flexibility and scalability of this platform, which is now being explored for other diseases like influenza and HIV.
In practical terms, choosing between Pfizer-BioNTech and Moderna often depends on availability, age eligibility, and individual health considerations. For parents, Pfizer’s lower dosage for children offers a tailored approach, while Moderna’s higher efficacy in adults may sway decisions for older populations. Regardless of choice, both vaccines exemplify the transformative potential of mRNA technology in modern medicine, offering a glimpse into a future where vaccines can be developed and adapted with unprecedented speed and precision.
Typhoid Vaccine: Understanding the Post-Vaccination Waiting Period
You may want to see also
Explore related products

$9.99



$63.74 $84.99


![]()
Non-mRNA Vaccines: Discussing vaccines made with inactivated viruses, proteins, or viral vectors, not mRNA
Not all vaccines rely on mRNA technology, and understanding the diverse landscape of vaccine development is crucial for informed decision-making. While mRNA vaccines have gained prominence, particularly with COVID-19, traditional methods like inactivated viruses, protein subunits, and viral vectors remain foundational in global health. These non-mRNA vaccines have been safeguarding populations for decades, each with unique mechanisms and applications.
Inactivated virus vaccines, such as the polio (IPV) and hepatitis A vaccines, use viruses rendered non-infectious through chemical or physical processes. This approach triggers an immune response without the risk of the disease itself. For instance, the IPV is administered in a series of four doses starting at 2 months of age, offering robust protection against poliomyelitis. The simplicity and safety of inactivated vaccines make them ideal for widespread use, especially in pediatric populations.
Protein subunit vaccines, like the shingles (Shingrix) and HPV (Gardasil) vaccines, contain specific pieces of a virus—often its surface proteins—to stimulate immunity. Shingrix, for example, uses a recombinant glycoprotein E combined with an adjuvant to enhance the immune response. It is recommended for adults over 50 in a two-dose series, spaced 2–6 months apart. This targeted approach minimizes side effects while providing strong, long-lasting protection.
Viral vector vaccines, exemplified by Johnson & Johnson’s COVID-19 vaccine and the Ebola vaccine (Ervebo), employ a harmless virus to deliver genetic material encoding a pathogen’s antigen. Ervebo, a single-dose vaccine approved for individuals over 18, uses a vesicular stomatitis virus to express an Ebola protein, inducing immunity without exposing recipients to the disease. While viral vector vaccines can provoke robust responses, they may be less suitable for individuals with specific allergies or immune conditions.
Each non-mRNA vaccine type offers distinct advantages, from the stability of inactivated vaccines to the precision of protein subunits and the versatility of viral vectors. Their continued development ensures a multifaceted defense against infectious diseases, catering to diverse needs and contexts. Understanding these alternatives empowers individuals to appreciate the breadth of vaccine science beyond mRNA innovations.
Is Baby's Silence After Vaccinations Normal? Understanding Post-Shot Quietness
You may want to see also
Explore related products

$124.73 $129




![]()
mRNA Vaccine Safety: Addressing safety profiles, side effects, and long-term studies of mRNA vaccines
Not all vaccines are made with mRNA technology; traditional vaccines use weakened or inactivated viruses, viral proteins, or toxins to elicit an immune response. mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna for COVID-19, represent a newer approach that instructs cells to produce a harmless protein triggering an immune response. This distinction is crucial for understanding safety profiles, as mRNA vaccines do not interact with DNA or alter genetic material, addressing a common misconception.
Safety profiles of mRNA vaccines are rigorously evaluated through clinical trials involving tens of thousands of participants across diverse age groups, including adolescents (ages 12 and up) and adults. For instance, the Pfizer-BioNTech COVID-19 vaccine was tested in over 43,000 individuals, while Moderna’s trial included 30,000 participants. These studies consistently demonstrated high efficacy rates (94-95%) and a favorable safety profile, with side effects typically mild to moderate. Common reactions include pain at the injection site, fatigue, headache, and muscle pain, usually resolving within a few days. Severe allergic reactions are rare, occurring in approximately 2-5 cases per million doses, emphasizing the importance of post-vaccination monitoring for 15-30 minutes, especially in individuals with a history of anaphylaxis.
Long-term studies are ongoing, but current data provide reassurance. mRNA degrades quickly in the body, typically within days, and does not persist long-term. Post-authorization surveillance systems, such as the CDC’s Vaccine Adverse Event Reporting System (VAERS) and Vaccine Safety Datalink (VSD), continuously monitor for rare or delayed adverse events. For example, myocarditis (heart inflammation) has been observed primarily in adolescent males and young adults following the second dose of mRNA COVID-19 vaccines, with incidence rates of 10.7 to 67 cases per 100,000 doses. However, most cases are mild and resolve with rest and anti-inflammatory medications, underscoring the importance of weighing risks against the benefits of protection against severe COVID-19.
Practical tips for managing side effects include applying a cool, clean, wet washcloth over the injection site, using over-the-counter pain relievers (e.g., acetaminophen or ibuprofen), and staying hydrated. Avoid strenuous activity for 24 hours if experiencing significant discomfort. For individuals concerned about long-term safety, it’s helpful to understand that mRNA technology has been studied for decades, with applications in cancer research and infectious diseases prior to COVID-19. While no medical intervention is without risk, the robust safety data and ongoing monitoring of mRNA vaccines provide a strong foundation for public trust.
In conclusion, mRNA vaccines represent a groundbreaking advancement in immunization, with safety profiles supported by extensive clinical trials and real-world data. While side effects are generally mild and short-lived, ongoing long-term studies and surveillance systems ensure continuous evaluation. By addressing misconceptions and providing practical guidance, individuals can make informed decisions about vaccination, balancing potential risks with the proven benefits of protection against serious illness.
Easily Display Your Vaccine Status on Your Smartphone: A Guide
You may want to see also
Explore related products






![]()
Future of mRNA Vaccines: Exploring potential applications of mRNA technology beyond COVID-19, like cancer or flu vaccines
MRNA technology, first widely recognized through its use in COVID-19 vaccines, is not the basis for all vaccines—traditional methods like inactivated viruses (e.g., flu shots) and viral vectors (e.g., Ebola vaccines) remain prevalent. However, mRNA’s rapid development and high efficacy during the pandemic have spotlighted its transformative potential. Beyond COVID-19, researchers are exploring mRNA’s adaptability for other diseases, including cancer, influenza, and even genetic disorders. This shift could redefine vaccine development, offering faster, more targeted solutions for complex health challenges.
Consider cancer vaccines, where mRNA’s ability to encode tumor-specific antigens presents a groundbreaking opportunity. Clinical trials are underway for personalized mRNA vaccines tailored to an individual’s cancer mutations. For example, Moderna’s mRNA-4157, in combination with Merck’s Keytruda, has shown promising results in melanoma patients, reducing recurrence risk by 44% in Phase 2 trials. Unlike traditional cancer treatments, these vaccines stimulate the immune system to recognize and attack cancer cells with minimal side effects. Dosage typically involves a priming injection followed by booster shots, administered over several weeks, with monitoring for immune response.
Influenza, a perennial global health challenge, is another prime candidate for mRNA innovation. Seasonal flu vaccines, often developed using egg-based methods, struggle to match rapidly evolving strains. mRNA vaccines, however, can be designed and manufactured within weeks, offering a more agile response. Pfizer and BioNTech are developing an mRNA flu vaccine targeting four influenza strains, with Phase 3 trials expected to conclude in 2024. If successful, this could mean annual flu shots with higher efficacy rates, particularly for vulnerable populations like the elderly and immunocompromised.
Yet, challenges remain. mRNA vaccines require ultra-cold storage, limiting accessibility in low-resource settings. Stability issues and high production costs also hinder scalability. To address these, researchers are exploring thermostable formulations and decentralized manufacturing. For instance, self-amplifying mRNA (saRNA) platforms, which use smaller doses to achieve the same immune response, could reduce costs and logistical barriers. Practical tips for healthcare providers include ensuring proper storage conditions and educating patients about the vaccine’s mechanism to build trust.
The future of mRNA technology extends beyond infectious diseases and cancer. Researchers are investigating its potential in treating genetic disorders like cystic fibrosis by delivering mRNA encoding functional proteins to replace defective ones. While still in early stages, preclinical studies show promise. For instance, a single dose of mRNA encoding CFTR protein restored lung function in mouse models. If translated to humans, this could revolutionize treatment for genetic diseases, offering a one-time or periodic intervention instead of lifelong medication.
In summary, mRNA technology’s versatility positions it as a cornerstone of future medicine. From cancer to flu and genetic disorders, its applications are vast and transformative. While technical and logistical hurdles persist, ongoing advancements in stability, delivery, and manufacturing could unlock its full potential. As research progresses, mRNA vaccines may not replace all traditional methods but will undoubtedly expand the toolkit for combating a wide array of diseases.
Should You Get a Typhoid Vaccine When Sick? Expert Advice
You may want to see also
Frequently asked questions
No, not all vaccines are made with mRNA. mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna for COVID-19, are a relatively new technology. Traditional vaccines use weakened or inactivated viruses, viral proteins, or other methods to trigger an immune response.
Vaccines that are not made with mRNA include inactivated vaccines (e.g., polio, hepatitis A), live-attenuated vaccines (e.g., measles, mumps, rubella), protein subunit vaccines (e.g., shingles, HPV), and viral vector vaccines (e.g., Johnson & Johnson COVID-19 vaccine, Ebola vaccine).
mRNA vaccines are gaining popularity due to their rapid development capabilities, high efficacy, and ability to be easily adapted for new variants or diseases. However, traditional vaccine technologies remain widely used and effective, offering proven safety and immunity for many diseases.