The ambitious global effort to vaccinate the world against COVID-19, once hailed as a beacon of international cooperation, has faced significant setbacks, raising questions about its unraveling. Initially, the COVAX initiative and other global partnerships aimed to ensure equitable vaccine distribution, but disparities between wealthy and low-income nations quickly emerged. Hoarding by affluent countries, logistical challenges, vaccine hesitancy, and the rise of new variants undermined progress. Additionally, geopolitical tensions and pharmaceutical patent disputes further complicated efforts, leaving billions without access to life-saving doses. This unraveling highlights the fragility of global solidarity in the face of a pandemic and underscores the urgent need for systemic reforms to address inequities in healthcare access.
| Characteristics | Values |
|---|---|
| Global Vaccine Inequality | Wealthy nations hoarded vaccines, leaving low-income countries with limited access. |
| Supply Chain Challenges | Cold chain requirements, transportation issues, and manufacturing delays hindered distribution. |
| Hesitancy and Misinformation | Widespread vaccine hesitancy fueled by misinformation and conspiracy theories. |
| Political and Bureaucratic Hurdles | Nationalistic policies, export bans, and slow regulatory approvals disrupted global efforts. |
| COVAX Shortfalls | The COVAX initiative fell short of its targets due to funding gaps and vaccine shortages. |
| Variant Emergence | New variants like Delta and Omicron reduced vaccine efficacy and increased global urgency. |
| Economic Disparities | Low-income countries lacked resources to purchase, store, and administer vaccines. |
| Logistical Complexities | Challenges in reaching remote populations and ensuring equitable distribution within countries. |
| Pharmaceutical Prioritization | Vaccine manufacturers prioritized high-paying countries over global equitable distribution. |
| Global Coordination Failures | Lack of unified global leadership and cooperation among nations and organizations. |
Explore related products






What You'll Learn
![]()
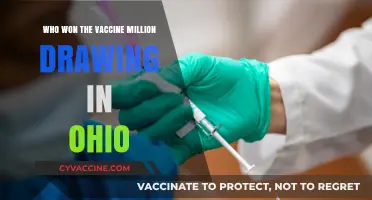
Global vaccine inequity and hoarding by wealthy nations
The COVID-19 pandemic exposed a stark reality: global vaccine distribution was never truly equitable. While wealthy nations stockpiled doses, often far exceeding their population needs, low-income countries struggled to secure even a fraction of the required vaccines. This hoarding by affluent nations wasn't merely a logistical oversight; it was a deliberate strategy driven by self-interest and a lack of global solidarity. For instance, by mid-2021, the United States had administered over 300 million doses, while many African countries had received fewer than 1 million doses combined. This disparity wasn’t just a moral failing—it prolonged the pandemic, allowing new variants like Delta and Omicron to emerge and spread globally.
Consider the mechanics of this inequity. Wealthy nations pre-purchased billions of doses through advance market commitments, effectively cornering the market. The COVAX initiative, designed to ensure equitable access, was underfunded and outmaneuvered. By the time COVAX began distributing vaccines in February 2021, the U.S. and EU had already secured enough doses to vaccinate their populations multiple times over. This hoarding wasn’t just about quantity; it was about control. Export bans, as seen in India and the EU, further exacerbated the crisis, leaving low-income nations at the mercy of trickle-down distribution.
The consequences of this inequity are measurable. A study by the International Chamber of Commerce estimated that vaccine inequity cost the global economy $2.3 trillion in 2021 alone. For every 10% increase in vaccination rates in low-income countries, global GDP could have risen by $153 billion. Yet, as of late 2021, only 3% of people in low-income countries had received a single dose, compared to over 60% in high-income countries. This wasn’t just a health crisis; it was an economic and humanitarian catastrophe fueled by policy choices.
To address this, a multi-pronged approach is essential. First, wealthy nations must stop hoarding doses and redirect excess supplies to COVAX or directly to low-income countries. Second, pharmaceutical companies should waive intellectual property rights temporarily, enabling local production in underserved regions. Third, global leaders must prioritize funding for vaccine delivery infrastructure in low-income countries, where cold chain logistics and healthcare worker shortages remain significant barriers. Finally, a global vaccine equity treaty could prevent such disparities in future pandemics, ensuring that self-interest never again trumps collective survival.
The lesson is clear: global health is not a zero-sum game. Hoarding vaccines may provide short-term security for wealthy nations, but it undermines long-term global stability. The unraveled grand plan to vaccinate the world wasn’t just a failure of logistics—it was a failure of empathy and foresight. Until we address the systemic inequities that allowed this to happen, the world will remain vulnerable to the next pandemic.
Australia's Hepatitis B Vaccine: A Historical Introduction and Impact
You may want to see also
Explore related products






![]()
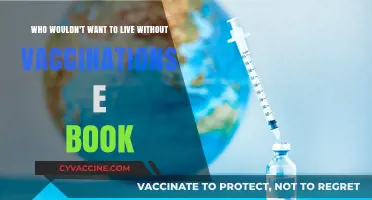
Supply chain disruptions and production challenges
The global vaccine rollout faced an unprecedented challenge: a complex dance of supply and demand, where every misstep had consequences. One of the critical issues was the fragility of the supply chain, a vast network of manufacturers, distributors, and healthcare providers, all of which had to work in harmony. A single disruption could cause a ripple effect, delaying vaccine delivery and endangering lives. For instance, the COVID-19 vaccine supply chain required precise temperature control, with some vaccines needing ultra-cold storage as low as -70°C. This meant specialized equipment and training, a significant hurdle for many countries, especially in warmer regions or those with limited infrastructure.
Consider the journey of a vaccine dose. It begins with production, where manufacturers face the daunting task of scaling up to meet global demand. The process is intricate, involving multiple stages, from cultivating the virus or bacteria to formulating and filling vials, each step requiring specific expertise and resources. For instance, the mRNA vaccines, a groundbreaking technology, demanded a new level of precision in manufacturing, with companies like Pfizer and Moderna having to rapidly expand their production capabilities. Any bottleneck in this process, be it a shortage of raw materials or specialized equipment, could halt production, causing delays in vaccine availability.
Now, imagine the logistics of distributing these vaccines. It's a race against time and temperature. Each vaccine has a limited shelf life, and the clock starts ticking from the moment it leaves the production facility. The distribution network must be efficient, ensuring vaccines reach their destinations swiftly. This is where the supply chain's vulnerability becomes apparent. Delays in transportation, customs clearance, or last-mile delivery can render vaccines ineffective. For instance, a shipment held up at a border due to paperwork could mean thousands of doses wasted, a devastating setback for a country awaiting its allocation.
To address these challenges, a multi-faceted approach is necessary. Firstly, diversifying production sites can reduce the risk of disruptions. Encouraging local manufacturing, especially in regions with limited access, ensures a more stable supply. Secondly, investing in cold chain infrastructure is vital. This includes providing training and equipment to maintain the integrity of vaccines during transport and storage. Governments and organizations should collaborate to streamline customs and regulatory processes, ensuring swift vaccine clearance. Lastly, real-time tracking systems can monitor vaccine shipments, allowing for quick intervention if issues arise. By strengthening these links in the supply chain, we can ensure a more resilient and efficient global vaccine distribution network.
In the grand scheme of global vaccination, supply chain management is a critical yet often overlooked aspect. It requires meticulous planning, international cooperation, and innovative solutions. By learning from the challenges faced during the COVID-19 vaccine rollout, we can improve our preparedness for future health crises, ensuring that the next grand plan to vaccinate the world is not only ambitious but also logistically sound. This involves not just producing vaccines but also delivering them effectively, a complex task that demands our attention and resources.
HBO Max Vaccination Special Release Date: What to Expect
You may want to see also
Explore related products






![]()
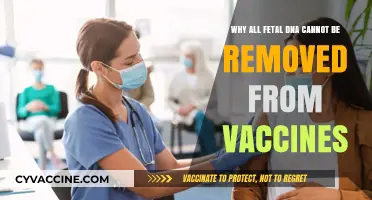
Vaccine hesitancy and misinformation campaigns
Vaccine hesitancy, once a fringe concern, has become a global obstacle, amplified by misinformation campaigns that exploit fear and uncertainty. Consider the COVID-19 pandemic: despite the rapid development of safe and effective vaccines, vaccination rates plateaued in many regions. In the U.S., for instance, only 69% of the eligible population was fully vaccinated by late 2023, far below the 90% threshold needed for herd immunity. This gap wasn’t due to supply shortages but to a complex interplay of distrust, confusion, and deliberate disinformation. Misinformation campaigns, often spread via social media, targeted vulnerable populations with false claims about vaccine safety, efficacy, and motives, creating a breeding ground for hesitancy.
To understand the mechanics of these campaigns, examine their tactics. Misinformation often leverages emotional triggers—fear, anger, or skepticism—to bypass critical thinking. For example, false claims that COVID-19 vaccines alter DNA or contain microchips went viral, despite scientific evidence to the contrary. Such narratives are particularly effective when they align with existing beliefs, such as distrust of pharmaceutical companies or government institutions. Social media algorithms exacerbate the problem by prioritizing engagement over accuracy, ensuring that sensationalist content reaches wider audiences. A study by the *Journal of Experimental Psychology* found that repeated exposure to misinformation, even when later corrected, can leave a lasting impression, making it harder to reverse false beliefs.
Addressing vaccine hesitancy requires a multi-pronged approach. First, public health messaging must be clear, consistent, and tailored to specific audiences. For instance, messaging aimed at parents might focus on protecting children, while campaigns targeting younger adults could emphasize community responsibility. Second, healthcare providers play a critical role as trusted sources of information. A survey by the Kaiser Family Foundation revealed that 80% of unvaccinated individuals would consider the vaccine if recommended by their doctor. Third, platforms like Facebook and Twitter must take greater responsibility for curbing misinformation. While some have implemented fact-checking tools, enforcement remains inconsistent, allowing false narratives to persist.
Practical steps can also empower individuals to combat misinformation. Encourage fact-checking using reliable sources like the WHO or CDC, and teach media literacy to identify red flags in online content (e.g., lack of credible citations, sensationalist language). For parents, discussing vaccines with pediatricians and sharing personal experiences can help build confidence. Policymakers should invest in community-based initiatives that engage local leaders, as these efforts often resonate more than top-down campaigns. Finally, transparency in vaccine development and distribution is essential. For example, publishing trial data and explaining side effects openly can counteract conspiracy theories.
The takeaway is clear: vaccine hesitancy and misinformation are not insurmountable, but they require proactive, strategic responses. By understanding the root causes and employing evidence-based solutions, societies can rebuild trust and protect public health. The lessons from COVID-19 serve as a stark reminder that vaccines are only as effective as the willingness to take them—and that willingness depends on defeating the misinformation that undermines it.
Smallpox Vaccine: The Age Children Received Their First Dose
You may want to see also
![]()
Political interference and bureaucratic delays
Political interference has been a silent saboteur in the global vaccination effort, often overshadowing logistical challenges. Consider the case of COVAX, the WHO-backed initiative designed to equitably distribute vaccines. When wealthier nations like the U.S. and EU prioritized bilateral deals with manufacturers, they effectively bypassed COVAX, leaving low-income countries at the mercy of delayed shipments. For instance, by mid-2021, African nations had received only 2% of global vaccine doses, despite housing 17% of the world’s population. This wasn’t merely a failure of supply chains but a direct consequence of political maneuvering, where self-interest trumped global solidarity.
Bureaucratic delays, on the other hand, operate like invisible handcuffs, slowing progress at every turn. Take India’s Serum Institute, the world’s largest vaccine manufacturer, which faced export bans due to domestic political pressures. These restrictions, though temporary, halted millions of doses destined for COVAX. Similarly, regulatory approvals in some countries took months longer than in others, not due to scientific scrutiny but procedural inefficiencies. For example, the AstraZeneca vaccine, approved in the UK in December 2020, didn’t receive the green light in Brazil until January 2021 and in South Africa until February, despite identical clinical data. Such delays cost lives, particularly in regions with surging cases.
The interplay between politics and bureaucracy is perhaps most evident in vaccine diplomacy. China and Russia leveraged their vaccines as geopolitical tools, offering doses to countries in exchange for political favors. While this increased access in some regions, it also created dependency and fragmented global efforts. For instance, Serbia received doses of both Sputnik V and Sinopharm, but its neighbors in the EU were bound by stricter procurement rules, leading to uneven distribution within the same geographic area. This politicization of vaccines not only delayed global coverage but also deepened existing inequalities.
To mitigate these issues, a two-pronged approach is essential. First, establish independent oversight bodies to insulate vaccine distribution from political whims. Second, streamline regulatory processes without compromising safety. For example, adopting a "rolling review" system, where data is assessed as it becomes available, could shave weeks off approval timelines. Additionally, high-income countries must honor their dose-sharing commitments—not as charitable acts, but as strategic investments in global health security. Without addressing these political and bureaucratic bottlenecks, even the most ambitious vaccination plans will remain unraveled, leaving the world vulnerable to future pandemics.
Unveiling the 1970s Vaccination Formulas: Ingredients and Their Evolution
You may want to see also
![]()
Funding gaps and donor fatigue in global efforts
The COVID-19 pandemic exposed a harsh reality: global health initiatives are only as strong as their weakest link. The ambitious goal of vaccinating the world against this virus faced a critical hurdle: funding gaps and donor fatigue. While initial pledges poured in, the sustained financial commitment required to reach every corner of the globe simply wasn't there.
Imagine a relay race where the baton is passed from one runner to the next. In this case, the baton represents funding, and the runners are donor countries and organizations. The race to vaccinate the world stumbled when some runners, exhausted by the prolonged effort and facing their own domestic challenges, slowed their pace. This "donor fatigue" left crucial gaps in the funding needed to procure vaccines, distribute them equitably, and ensure their administration in hard-to-reach areas.
Consider the COVAX facility, a global initiative aimed at equitable vaccine distribution. It faced a staggering $2 billion shortfall in 2021, hindering its ability to secure doses for low-income countries. This meant that while wealthy nations were administering booster shots, many vulnerable populations remained unprotected, leaving the door open for new variants to emerge and prolonging the pandemic for everyone.
The consequences of these funding gaps are stark. Lower vaccination rates in developing countries not only endanger local populations but also create breeding grounds for new variants that can spread globally, undermining the progress made elsewhere. It's a stark reminder that global health is interconnected – a vulnerability in one region becomes a threat to all.
To break this cycle, we need a paradigm shift. Sustainable funding mechanisms, beyond reliance on sporadic donations, are crucial. This could involve exploring innovative financing models like vaccine bonds or leveraging existing global health funds more effectively. Additionally, fostering greater collaboration between governments, private sector entities, and philanthropic organizations is essential to pool resources and expertise. The world cannot afford to let donor fatigue derail future global health initiatives. The cost of inaction is simply too high.
Vaccines vs. Immunization: Understanding the Key Differences and Benefits
You may want to see also
Frequently asked questions
The primary goal was to ensure equitable access to COVID-19 vaccines worldwide to curb the pandemic, prevent new variants, and protect vulnerable populations. It was deemed crucial to achieve herd immunity and stabilize global health and economies.
The plan unraveled due to vaccine hoarding by wealthy nations, logistical challenges in low-income countries, vaccine hesitancy, and insufficient funding and coordination among international organizations.
New variants like Delta and Omicron reduced vaccine efficacy, increased breakthrough infections, and necessitated booster shots, straining global supply and complicating distribution efforts, especially in under-vaccinated regions.