After a bone marrow transplant, the guidelines for administering vaccines are typically established by a combination of international and national health organizations, such as the Centers for Disease Control and Prevention (CDC), the World Health Organization (WHO), and the European Society for Blood and Marrow Transplantation (EBMT). These organizations collaborate with expert panels, including immunologists, infectious disease specialists, and hematologists, to develop evidence-based recommendations tailored to the unique immunological challenges faced by transplant recipients. Additionally, individual healthcare institutions and transplant centers often adapt these guidelines to suit their patient populations, ensuring personalized care while adhering to broader standards. The goal is to optimize vaccine efficacy and safety, protecting patients from preventable infections during their recovery period.
| Characteristics | Values |
|---|---|
| Guideline-Setting Organizations | Centers for Disease Control and Prevention (CDC), Infectious Diseases Society of America (IDSA), European Conference on Infections in Leukaemia (ECIL), American Society of Transplantation and Cellular Therapy (ASTCT) |
| Primary Audience | Healthcare providers, hematologists, oncologists, transplant physicians |
| Focus | Immunization protocols for patients post-bone marrow transplant (BMT) |
| Key Recommendations | Timing of vaccinations, vaccine types (inactivated vs. live), dose schedules, booster requirements |
| Vaccine Types Addressed | Influenza, pneumococcal, hepatitis B, meningococcal, herpes zoster, COVID-19, etc. |
| Timing Post-Transplant | Typically starts 6-12 months after BMT, depending on immune recovery |
| Considerations | Immune status, graft-versus-host disease (GVHD), medication interactions |
| Updates Frequency | Regularly updated based on new research and vaccine developments |
| Global Variations | Guidelines may differ slightly between regions (e.g., U.S., Europe) |
| Evidence-Based | Recommendations are based on clinical trials and expert consensus |
| Patient-Specific Factors | Age, comorbidities, and individual immune response are considered |
| Collaboration | Multidisciplinary approach involving infectious disease specialists and transplant teams |
| Accessibility | Guidelines are publicly available through organizational websites and publications |
Explore related products






What You'll Learn
- Role of Transplant Team: Physicians and specialists directly involved in the transplant process establish initial vaccine protocols
- CDC Recommendations: Centers for Disease Control and Prevention provide general guidelines for post-transplant vaccinations
- ACIP Influence: Advisory Committee on Immunization Practices offers evidence-based advice for vaccine scheduling
- Institutional Policies: Hospitals and clinics may adapt guidelines based on patient-specific risks and resources
- Patient-Specific Plans: Individualized vaccine schedules are tailored by healthcare providers post-transplant
![]()
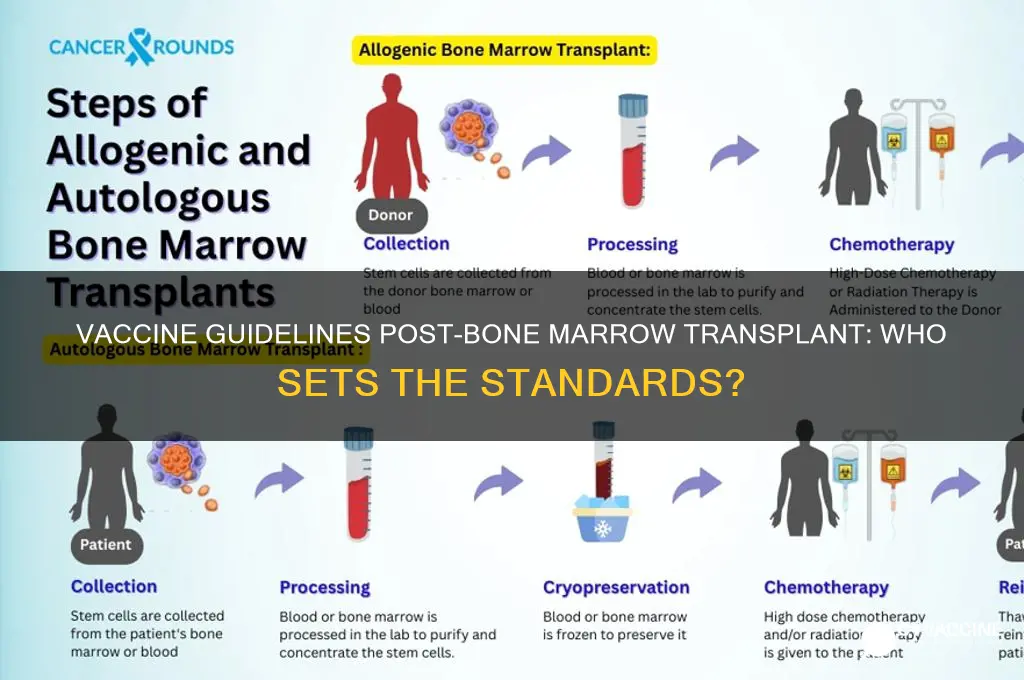
Role of Transplant Team: Physicians and specialists directly involved in the transplant process establish initial vaccine protocols
The transplant team, comprising hematologists, oncologists, infectious disease specialists, and immunologists, plays a pivotal role in establishing initial vaccine protocols for patients post-bone marrow transplant. These protocols are not one-size-fits-all; they are meticulously tailored to the patient’s immune reconstitution timeline, underlying conditions, and transplant type (autologous vs. allogeneic). For instance, allogeneic transplant recipients typically experience slower immune recovery, necessitating delayed vaccination schedules compared to autologous recipients. The team’s expertise ensures that vaccines are administered at optimal intervals to maximize efficacy without compromising the fragile immune system.
Consider the timing of vaccine administration, a critical factor influenced by the transplant team’s guidelines. For inactivated vaccines, such as the influenza vaccine, initiation often begins 6–12 months post-transplant, depending on the patient’s immune recovery. Live-attenuated vaccines, like the MMR (measles, mumps, rubella) vaccine, are generally deferred until at least 24 months post-transplant due to the risk of vaccine-strain infection in immunocompromised patients. The team may also recommend higher dosages or additional booster shots to compensate for suboptimal immune responses, particularly in older adults or those with comorbidities.
A comparative analysis highlights the transplant team’s role in balancing risks and benefits. For example, while the COVID-19 mRNA vaccines are recommended for all post-transplant patients, the team may advise a third primary dose for those with persistently low B-cell counts. This decision is informed by monitoring immune markers like CD19+ B-cell levels and serologic responses to prior vaccinations. In contrast, patients with graft-versus-host disease (GVHD) may require further delays or adjustments to avoid exacerbating inflammation. The team’s nuanced approach ensures that vaccination supports long-term health without interfering with transplant outcomes.
Practical tips from the transplant team include maintaining open communication with primary care providers to ensure vaccine records are up-to-date and coordinating with pharmacies to access specialized vaccines, such as high-dose influenza formulations. Patients are often advised to avoid public spaces during peak infection seasons and to carry a vaccination card detailing their transplant history. The team may also recommend prophylactic antibiotics or antiviral medications during vaccine-induced immune activation periods. By integrating these strategies, the transplant team empowers patients to navigate post-transplant life with confidence and safety.
Traveling to Korea? Vaccination Requirements You Need to Know
You may want to see also
Explore related products






![]()
CDC Recommendations: Centers for Disease Control and Prevention provide general guidelines for post-transplant vaccinations
The Centers for Disease Control and Prevention (CDC) play a pivotal role in shaping post-transplant vaccination protocols, offering a comprehensive framework that healthcare providers rely on to protect immunocompromised patients. These guidelines are not one-size-fits-all but are meticulously tailored to address the unique vulnerabilities of bone marrow transplant recipients. For instance, the CDC recommends restarting vaccinations 6 to 12 months after transplant, depending on the patient’s immune recovery and the type of transplant (autologous vs. allogeneic). This phased approach ensures that vaccines are administered when the immune system is most likely to respond effectively, balancing safety and efficacy.
One critical aspect of the CDC’s recommendations is the prioritization of specific vaccines. Inactivated vaccines, such as the influenza vaccine and the Tdap (tetanus, diphtheria, and pertussis) vaccine, are typically administered first, as they pose minimal risk to immunocompromised individuals. Live attenuated vaccines, like the MMR (measles, mumps, rubella) and varicella vaccines, are deferred until the immune system has sufficiently recovered, often 2 years post-transplant. Notably, the CDC advises against administering live vaccines to patients on immunosuppressive therapy, as they may trigger severe infections. Dosage adjustments are also recommended; for example, pneumococcal vaccines (PCV15 and PPSV23) are given sequentially, with a minimum interval of 8 weeks between doses, to maximize protection against pneumonia.
The CDC’s guidelines also emphasize the importance of serologic testing to assess immune responses to vaccinations. For instance, hepatitis B surface antibody titers should be checked 1–2 months after the final dose of the hepatitis B vaccine series. If titers are inadequate, additional doses or alternative strategies, such as high-dose regimens, may be considered. This personalized approach ensures that patients receive the maximum benefit from vaccinations despite their compromised immune systems.
Practical implementation of these guidelines requires close collaboration between transplant teams, infectious disease specialists, and primary care providers. Patients should be educated about the importance of adhering to the vaccination schedule and the potential risks of vaccine-preventable diseases. For example, influenza vaccination is particularly critical for transplant recipients, as they are at higher risk of severe complications from the flu. The CDC also recommends that household contacts receive all age-appropriate vaccines, including the annual flu shot, to create a protective cocoon around the vulnerable patient.
In summary, the CDC’s recommendations serve as a cornerstone for post-transplant vaccination strategies, offering evidence-based, patient-centered guidance. By following these protocols, healthcare providers can significantly reduce the risk of vaccine-preventable diseases in bone marrow transplant recipients, improving long-term outcomes and quality of life. However, adherence to these guidelines requires vigilance, coordination, and a deep understanding of the patient’s unique immunologic status.
DNA Vaccines: How They Train Your Body to Fight Future Diseases
You may want to see also
Explore related products





![]()
ACIP Influence: Advisory Committee on Immunization Practices offers evidence-based advice for vaccine scheduling
The Advisory Committee on Immunization Practices (ACIP) plays a pivotal role in shaping vaccine guidelines, particularly for vulnerable populations like bone marrow transplant recipients. This committee, comprising medical and public health experts, meticulously reviews scientific evidence to provide recommendations that ensure optimal immune protection. For instance, ACIP advises that transplant recipients receive specific vaccines at precise intervals post-transplant, considering the immune system’s gradual recovery. Their evidence-based approach ensures that guidelines are both safe and effective, minimizing risks like infection or graft rejection.
One critical aspect of ACIP’s influence is its detailed vaccine scheduling for bone marrow transplant patients. For example, inactivated vaccines such as the influenza vaccine are typically administered 6–12 months post-transplant, while live vaccines like MMR (measles, mumps, rubella) are deferred until at least 24 months post-transplant due to the risk of vaccine-strain infection. ACIP also emphasizes the importance of serologic testing to assess immune response, ensuring that additional doses are given if needed. This tailored approach reflects ACIP’s commitment to balancing immune reconstitution with patient safety.
ACIP’s recommendations are not static; they evolve with emerging research and clinical data. For instance, recent studies on COVID-19 vaccines in immunocompromised populations have prompted ACIP to recommend additional doses and shorter dosing intervals for transplant recipients. This adaptability ensures that guidelines remain current and responsive to new challenges. Healthcare providers rely on ACIP’s updates to make informed decisions, particularly in complex cases where standard protocols may not apply.
Practical implementation of ACIP’s guidelines requires collaboration between transplant teams, infectious disease specialists, and primary care providers. Patients must be educated about the importance of adhering to the vaccine schedule, as well as potential side effects and signs of infection. For example, caregivers should monitor for fever or unusual symptoms after vaccination, especially with live vaccines. ACIP’s evidence-based advice not only informs clinical practice but also empowers patients to take an active role in their post-transplant care.
In summary, ACIP’s influence on vaccine scheduling for bone marrow transplant recipients is both profound and practical. By offering evidence-based recommendations, the committee ensures that patients receive timely, safe, and effective immunizations tailored to their unique needs. Healthcare providers and patients alike benefit from ACIP’s rigorous approach, which bridges the gap between scientific research and clinical application, ultimately improving outcomes for this vulnerable population.
Understanding Vaccine Development: A Step-by-Step Guide to Combating Viruses
You may want to see also
Explore related products





![]()
Institutional Policies: Hospitals and clinics may adapt guidelines based on patient-specific risks and resources
Hospitals and clinics often tailor vaccine guidelines for bone marrow transplant recipients based on individual patient risks and available resources. For instance, a 45-year-old patient with a history of graft-versus-host disease (GvHD) may receive a reduced dose of the influenza vaccine (e.g., half the standard dose) to minimize immune system strain, while a younger, otherwise healthy recipient might follow standard dosing protocols. This customization reflects the delicate balance between protecting patients from vaccine-preventable diseases and avoiding complications in their fragile post-transplant state.
Institutional policies frequently incorporate flexibility to address resource limitations. A rural clinic with limited access to specialized vaccines, such as the pneumococcal conjugate vaccine (PCV13), might prioritize high-risk patients (e.g., those with neutropenia) for vaccination, delaying administration for lower-risk individuals. Similarly, facilities with constrained staffing may extend the interval between vaccine doses, provided this approach aligns with patient safety and recovery timelines. These adaptations ensure that guidelines remain practical without compromising care quality.
A persuasive argument for tailored policies lies in their ability to improve patient outcomes. For example, a hospital might implement a tiered vaccination schedule based on immune reconstitution milestones. Patients with CD4+ T-cell counts above 200 cells/μL could receive live-attenuated vaccines (e.g., MMR) earlier than those with lower counts, reducing the risk of vaccine-related complications. Such strategies demonstrate how institutional policies can optimize vaccine efficacy while safeguarding vulnerable populations.
Comparatively, rigid adherence to generalized guidelines may overlook unique patient circumstances. A 60-year-old recipient with comorbidities like diabetes or chronic lung disease faces higher risks from infections, necessitating accelerated vaccination timelines. Conversely, a pediatric patient might require delayed vaccination due to immature immune system development. By embracing adaptability, institutions ensure that guidelines serve as a framework rather than a straitjacket, fostering better-individualized care.
In practice, hospitals often collaborate with multidisciplinary teams to refine policies. Pharmacists, infectious disease specialists, and transplant physicians jointly assess factors like graft source (autologous vs. allogeneic), immunosuppressive therapy regimens, and patient lifestyle. For instance, a patient returning to work in a healthcare setting might receive priority for COVID-19 booster doses. This collaborative approach ensures that institutional policies remain dynamic, evidence-based, and patient-centered.
Shingrix Vaccine Allergic Reaction: Recognizing Symptoms and Seeking Help
You may want to see also
Explore related products






![]()
Patient-Specific Plans: Individualized vaccine schedules are tailored by healthcare providers post-transplant
After a bone marrow transplant, the immune system is essentially reset, leaving patients vulnerable to infections. This critical period demands a meticulous approach to vaccination, one that goes beyond a one-size-fits-all model. Enter patient-specific plans, where healthcare providers meticulously tailor vaccine schedules to individual needs. This personalized strategy considers factors like the patient's age, underlying health conditions, the type of transplant, and the intensity of the conditioning regimen. For instance, a 60-year-old with a history of diabetes and a myeloablative transplant will have a vastly different vaccine timeline compared to a 25-year-old with a reduced-intensity transplant.
Healthcare providers, often infectious disease specialists or transplant physicians, act as architects of these individualized plans. They leverage guidelines from organizations like the Centers for Disease Control and Prevention (CDC) and the European Conference on Infections in Leukaemia (ECIL), but these serve as frameworks, not rigid rules. The provider's expertise lies in interpreting these guidelines within the unique context of each patient. This might involve adjusting vaccine dosages – a child might receive a lower dose of the MMR vaccine compared to an adult – or spacing out vaccines to avoid overwhelming the recovering immune system.
A key challenge in crafting these plans is the delicate balance between protecting the patient and avoiding potential harm. Live-attenuated vaccines, like the varicella vaccine, are generally avoided in the early post-transplant period due to the risk of vaccine-strain infection. Instead, inactivated vaccines, such as the pneumococcal conjugate vaccine (PCV13), are prioritized. The timing of these vaccinations is crucial; starting too early might result in inadequate immune response, while delaying too long leaves the patient susceptible. Typically, inactivated vaccines are initiated 6-12 months post-transplant, with live vaccines introduced later, often after 2 years.
Regular monitoring of immune function through blood tests is essential to guide these decisions. If antibody levels remain low, booster doses may be necessary. This iterative process requires close collaboration between the patient, their caregiver, and the healthcare team.
Patient-specific vaccine plans are not static; they evolve as the patient's immune system recovers and new medical developments emerge. This dynamic approach ensures optimal protection against preventable diseases, minimizing the risk of complications and promoting long-term health after a bone marrow transplant.
How to Participate in a Vaccine Trial: A Step-by-Step Guide
You may want to see also
Frequently asked questions
The guidelines for vaccines after a bone marrow transplant are typically set by medical organizations such as the Centers for Disease Control and Prevention (CDC), the European Conference on Infections in Leukaemia (ECIL), and the American Society of Transplantation and Cellular Therapy (ASTCT).
No, vaccine guidelines can vary by region and country. While international organizations like the World Health Organization (WHO) provide overarching recommendations, local health authorities and transplant centers often adapt these guidelines to fit specific healthcare systems and patient populations.
Vaccine guidelines are regularly reviewed and updated based on new research, emerging infections, and changes in vaccine technology. Updates can occur annually or as needed, with major revisions often published by leading medical organizations and transplant societies.