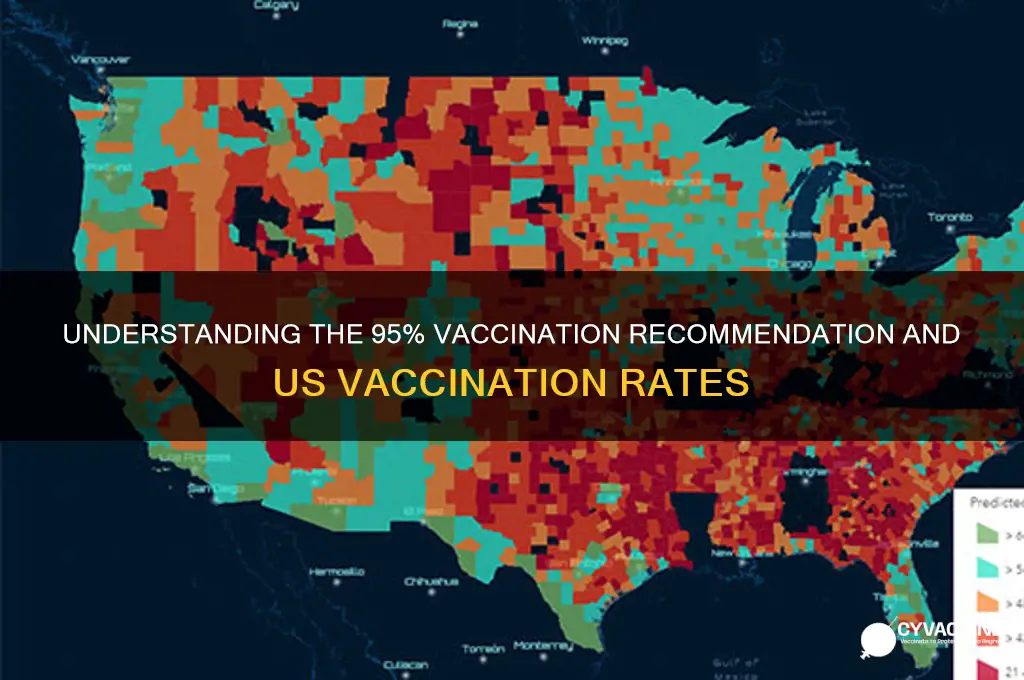
The recommendation for a 95% vaccination rate often refers to the concept of herd immunity, where a high percentage of the population needs to be vaccinated to effectively stop the spread of a disease. This figure is particularly relevant for highly contagious diseases like measles. However, the actual vaccination rates in the USA vary significantly by vaccine and demographic group. For instance, childhood vaccines such as MMR (measles, mumps, rubella) typically achieve coverage rates above 90% among school-aged children, thanks to school immunization requirements. In contrast, adult vaccination rates, such as for influenza or COVID-19, are generally lower, often ranging between 40% to 70%, depending on the vaccine and population subgroup. These disparities highlight the ongoing challenges in achieving widespread immunity and the importance of public health efforts to improve vaccination uptake across all age groups.
Explore related products





What You'll Learn
- WHO's 95% Vaccination Recommendation: Global health target for herd immunity against infectious diseases
- Actual U.S. Vaccination Rates: Current coverage varies by vaccine type and demographic group
- COVID-19 Vaccination in USA: High uptake but disparities persist in certain communities
- Childhood Immunization Rates: Most vaccines meet WHO targets, exceptions like flu and HPV
- Vaccine Hesitancy Impact: Misinformation and access barriers lower U.S. vaccination compliance
![]()
WHO's 95% Vaccination Recommendation: Global health target for herd immunity against infectious diseases
The World Health Organization (WHO) has set a bold target: achieving 95% vaccination coverage to establish herd immunity against infectious diseases. This recommendation is not arbitrary; it’s rooted in epidemiological models that show this threshold is critical to interrupting disease transmission. For highly contagious diseases like measles, which has a basic reproduction number (R0) of 12-18, even a small drop below 95% coverage can lead to outbreaks. For instance, a 5% gap in measles vaccination can result in a 50% increase in susceptible individuals, undermining decades of progress. This target is a global health imperative, but its success hinges on local implementation and equitable access to vaccines.
Achieving 95% vaccination coverage requires more than just vaccine availability; it demands strategic planning and community engagement. WHO outlines a three-pronged approach: strengthening health systems, addressing vaccine hesitancy, and ensuring equitable distribution. For example, in low-income countries, cold chain logistics are critical for vaccine viability, while in high-income nations like the U.S., combating misinformation is paramount. The U.S. CDC reports that only 91% of children receive the measles-mumps-rubella (MMR) vaccine by age 2, falling short of the 95% target. Bridging this gap involves tailored interventions, such as school-based vaccination drives and culturally sensitive communication campaigns.
Comparatively, countries like Portugal and Rwanda have achieved over 95% vaccination rates for key diseases through universal healthcare systems and robust public health infrastructure. Portugal’s success with HPV vaccination (95% coverage in adolescents) highlights the role of school-based programs and parental education. Rwanda’s 93% measles vaccination rate, despite resource constraints, demonstrates the power of community health workers and mobile clinics. These examples underscore that the 95% target is attainable but requires political will, sustained funding, and localized strategies.
A critical challenge to the 95% goal is vaccine hesitancy, fueled by misinformation and historical mistrust. WHO recommends a behavioral science approach, emphasizing empathy over confrontation. For instance, addressing parental concerns about vaccine safety involves transparent communication about side effects (e.g., mild fever post-MMR vaccination in 5-15% of cases) and long-term benefits. In the U.S., where 20% of parents express vaccine skepticism, platforms like VaxChat connect families with healthcare providers for personalized guidance. Pairing data with storytelling—such as sharing outbreak stories from under-vaccinated communities—can humanize the urgency of herd immunity.
Finally, the 95% recommendation is not a one-size-fits-all solution; it must adapt to disease-specific contexts. For polio, where the oral vaccine’s effectiveness varies by strain, WHO advocates a combination of routine immunization and supplementary campaigns. For COVID-19, the target shifts based on vaccine efficacy and viral mutations, with boosters recalibrated for at-risk groups (e.g., elderly, immunocompromised). Practical tips for policymakers include mapping vaccine deserts, leveraging digital health records for real-time monitoring, and incentivizing healthcare providers to reach underserved populations. The 95% target is ambitious but achievable—if we treat it as a shared responsibility, not just a statistic.
Los Angeles Daily Vaccine Rollout: Tracking Shots Administered Each Day
You may want to see also
Explore related products

$11.93 $21.99





![]()
Actual U.S. Vaccination Rates: Current coverage varies by vaccine type and demographic group
The World Health Organization (WHO) often recommends vaccination coverage of at least 95% to achieve herd immunity for highly contagious diseases like measles. In the U.S., actual vaccination rates fall short of this benchmark, varying significantly by vaccine type and demographic group. For instance, childhood vaccines such as MMR (measles, mumps, rubella) achieve coverage around 90% nationally, but this drops to 60-70% in some communities, leaving pockets of vulnerability. Adult vaccines, like the annual flu shot, hover around 50% coverage, with disparities widening by age, race, and socioeconomic status. Understanding these variations is critical to addressing gaps and strengthening public health defenses.
Consider the COVID-19 vaccine rollout, a recent case study in demographic disparities. As of late 2023, approximately 68% of the U.S. population has completed the primary series, but booster uptake is uneven: only 20% of adults have received the updated bivalent booster. Age plays a stark role, with 85% of seniors aged 65+ completing the primary series compared to 55% of adults aged 18-29. Racial gaps persist, too: while 72% of Asian Americans are fully vaccinated, only 58% of Black Americans and 63% of Hispanic Americans have reached this milestone. These differences highlight the need for targeted outreach, culturally sensitive messaging, and equitable access to vaccination sites.
To bridge these gaps, public health strategies must be tailored to specific populations. For children, school-based vaccination programs and reminder systems have proven effective, but exemptions for non-medical reasons undermine progress. Adults require workplace incentives, mobile clinics, and clear communication about vaccine safety and efficacy. For example, the CDC recommends a shingles vaccine (Shingrix) for adults over 50, yet only 35% have received both required doses. Practical tips include scheduling the second dose at the time of the first and using pharmacy-based services for convenience.
Comparing U.S. vaccination rates to global benchmarks reveals both strengths and weaknesses. While the U.S. leads in COVID-19 vaccine development and initial distribution, it lags behind countries like Portugal (90% fully vaccinated) and Singapore (85% boosted). Routine childhood vaccines in the U.S. surpass rates in many low-income nations but fall short of WHO’s 95% target. This comparison underscores the importance of sustained investment in vaccine infrastructure, public trust, and global collaboration.
In conclusion, the U.S. vaccination landscape is a patchwork of successes and challenges, shaped by vaccine type, demographics, and systemic factors. Achieving WHO-recommended coverage requires more than medical solutions—it demands addressing hesitancy, improving access, and fostering community engagement. By learning from disparities and leveraging proven strategies, the U.S. can move closer to protecting all populations against preventable diseases.
Polio Vaccine and Fetal Tissue: Separating Fact from Fiction
You may want to see also
Explore related products

$3.59 $24.95





![]()
COVID-19 Vaccination in USA: High uptake but disparities persist in certain communities
The COVID-19 vaccination campaign in the United States has been a monumental effort, with over 670 million doses administered as of October 2023. This high uptake has significantly contributed to reducing severe illness, hospitalizations, and deaths. The Centers for Disease Control and Prevention (CDC) reports that approximately 80% of the eligible population (ages 5 and older) has received at least one dose, and 68% are fully vaccinated. These numbers reflect a robust response to the pandemic, aligning with the World Health Organization’s (WHO) recommendation of achieving at least 70% vaccination coverage to control the spread of the virus. However, the national averages mask persistent disparities in vaccination rates across certain communities, highlighting the need for targeted interventions.
Analyzing the data reveals that vaccination rates vary widely by demographic factors such as race, ethnicity, geographic location, and socioeconomic status. For instance, while 73% of Asian Americans and 62% of White Americans are fully vaccinated, only 56% of Hispanic and 52% of Black Americans have completed their primary series. Rural areas also lag behind urban centers, with vaccination rates in some rural counties as low as 40%. These disparities are often driven by systemic barriers, including limited access to healthcare facilities, vaccine hesitancy fueled by misinformation, and historical mistrust of medical institutions among marginalized communities. Addressing these gaps requires culturally sensitive outreach, mobile vaccination clinics, and community-led initiatives to build trust and improve accessibility.
From a practical standpoint, closing the vaccination gap involves tailored strategies. For example, offering vaccines at local churches, schools, and workplaces can increase convenience for underserved populations. Translating vaccine information into multiple languages and using trusted community leaders as messengers can combat misinformation. Additionally, addressing logistical challenges, such as providing transportation to vaccination sites or offering flexible appointment times, can remove barriers for those with limited mobility or rigid work schedules. The CDC’s “Vaccines for Children” program and similar initiatives can serve as models for ensuring equitable access, particularly for low-income families.
Comparatively, the U.S. vaccination rates are higher than many countries but still fall short of the 95% coverage often cited as necessary for herd immunity against highly contagious variants like Delta and Omicron. While the WHO’s 70% target is a critical milestone, achieving higher coverage remains essential to minimize the emergence of new variants and protect vulnerable populations. The U.S. experience underscores that even in a resource-rich nation, equitable vaccine distribution and uptake are complex challenges that demand sustained effort and innovation.
In conclusion, while the U.S. has made significant strides in COVID-19 vaccination, disparities in uptake persist and threaten to undermine progress. By focusing on targeted, community-driven solutions, policymakers and healthcare providers can bridge these gaps and move closer to comprehensive protection. The lessons learned from this campaign will be invaluable for future public health initiatives, emphasizing the importance of inclusivity, trust, and adaptability in achieving widespread immunization.
Parental Concerns: How Many Believe Vaccines Pose Harm to Children?
You may want to see also
Explore related products






![]()
Childhood Immunization Rates: Most vaccines meet WHO targets, exceptions like flu and HPV
The World Health Organization (WHO) recommends a 95% vaccination rate for many childhood immunizations to achieve herd immunity, a critical threshold for preventing outbreaks. In the United States, most childhood vaccines meet or exceed this target, a testament to decades of public health efforts. Diseases like measles, mumps, and rubella, once common, are now rare thanks to high vaccination rates. For instance, the MMR vaccine, typically administered in two doses starting at 12 months, boasts a coverage rate of over 90% among kindergarteners, effectively controlling these diseases.
However, not all vaccines fare equally well. Influenza (flu) and Human Papillomavirus (HPV) vaccines fall short of WHO targets, with significant implications for public health. Flu vaccination rates among children aged 6 months to 17 years hover around 60%, far below the 95% goal. This gap leaves communities vulnerable to seasonal outbreaks, particularly among young children and those with underlying health conditions. Parents often underestimate the severity of flu in children, but it can lead to hospitalization and even death. To improve uptake, healthcare providers should emphasize the annual nature of the flu vaccine and its safety profile, dispelling myths about its effectiveness.
HPV vaccination rates are equally concerning, with only about 54% of adolescents completing the recommended two-dose series by age 17. This vaccine prevents cancers caused by HPV, including cervical, throat, and anal cancers. Misconceptions about the vaccine’s necessity or safety persist, despite its proven track record. Pediatricians can play a pivotal role by framing HPV vaccination as a cancer prevention tool rather than solely a sexually transmitted infection prevention measure. Starting the series at age 9–12, as recommended, can also normalize it as a routine part of adolescent care.
Closing these gaps requires targeted strategies. For flu, schools and clinics could offer on-site vaccination clinics, reducing barriers to access. For HPV, provider training in effective communication techniques and state-level policies, such as school entry requirements, could boost rates. Parents should also be educated on the long-term benefits of these vaccines, emphasizing their role in preventing serious diseases. While most childhood immunizations meet WHO targets, addressing disparities in flu and HPV vaccination is crucial for comprehensive public health protection.
CDC-Recommended Vaccines: Protecting Newborns from Day One
You may want to see also
Explore related products






![]()
Vaccine Hesitancy Impact: Misinformation and access barriers lower U.S. vaccination compliance
The World Health Organization (WHO) recommends a 95% vaccination rate to achieve herd immunity for highly contagious diseases like measles, yet the actual vaccination coverage in the U.S. falls short, particularly for vaccines such as the MMR (measles, mumps, rubella). For instance, as of 2023, only about 92% of U.S. children aged 19–35 months have received one dose of the MMR vaccine, leaving a gap that allows outbreaks to occur. This disparity highlights the critical impact of vaccine hesitancy, driven by misinformation and access barriers, on public health compliance.
Misinformation spreads like a virus, eroding trust in vaccines through social media, conspiracy theories, and unverified sources. A 2022 study found that 64% of U.S. adults encountered COVID-19 vaccine misinformation online, with 37% reporting it made them less likely to get vaccinated. For example, false claims linking vaccines to autism or infertility persist despite overwhelming scientific evidence to the contrary. This distrust isn’t limited to new vaccines; it affects routine immunizations like the flu shot, where only 50% of U.S. adults were vaccinated in the 2022–2023 season. Combatting misinformation requires clear, accessible communication from healthcare providers and public health campaigns that address concerns directly.
Access barriers further compound vaccine hesitancy, disproportionately affecting underserved communities. Rural areas often lack nearby vaccination sites, while urban areas may face long wait times or limited appointment availability. For instance, only 68% of rural Americans live within a 10-mile radius of a pharmacy offering vaccines, compared to 94% of urban residents. Additionally, uninsured individuals or those with high out-of-pocket costs are less likely to seek vaccination. Practical solutions include mobile clinics, extended clinic hours, and eliminating cost barriers through programs like the Vaccines for Children (VFC) program, which provides free vaccines to eligible children up to age 18.
The interplay of misinformation and access barriers creates a vicious cycle: distrust reduces demand, and reduced demand limits investment in accessible services. For example, during the COVID-19 pandemic, counties with higher vaccine hesitancy saw slower rollout of vaccination sites, exacerbating inequities. Breaking this cycle requires a dual approach: addressing misinformation through education and improving access through policy and infrastructure. Schools, workplaces, and community centers can serve as vaccination hubs, while digital tools like text reminders and online scheduling can streamline access.
Ultimately, closing the gap between WHO recommendations and U.S. vaccination rates demands a targeted strategy. For parents, verifying vaccine information through trusted sources like the CDC or WHO is crucial. For policymakers, investing in equitable access and incentivizing vaccination through workplace programs or school requirements can drive compliance. By tackling misinformation and access barriers head-on, the U.S. can move closer to the 95% threshold needed for herd immunity, protecting both individuals and communities from preventable diseases.
Late for Your Vaccine Appointment? What to Expect and Do Next
You may want to see also
Frequently asked questions
The 95% vaccination target is often recommended by public health organizations, such as the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC), to achieve herd immunity for highly contagious diseases like measles.
As of recent data, the actual vaccination rate in the USA varies by vaccine and demographic group. For example, COVID-19 vaccination rates fluctuate, but as of late 2023, approximately 68-70% of the eligible U.S. population had received at least one dose, though this falls short of the 95% target for herd immunity against highly contagious variants.
The CDC recommends several vaccines for the general population, including COVID-19, influenza (flu), measles, mumps, rubella (MMR), tetanus, diphtheria, pertussis (Tdap), human papillomavirus (HPV), and others, depending on age, health status, and risk factors.