As the global vaccination rollout continues, the question of who qualifies for the next round of vaccines is a critical concern for public health officials and communities alike. Priority groups are typically determined based on factors such as age, underlying health conditions, occupation, and geographic location, with the goal of maximizing protection for those most vulnerable to severe illness and death from COVID-19. In many regions, initial phases have focused on healthcare workers, the elderly, and individuals with comorbidities, while subsequent rounds may expand to include essential workers, younger age groups, and the general population. However, the allocation process can vary significantly between countries, influenced by vaccine supply, distribution infrastructure, and local epidemiological data. As new variants emerge and vaccine efficacy is continually assessed, eligibility criteria may evolve, requiring ongoing communication and transparency to ensure equitable access and public trust in the vaccination program.
Explore related products






What You'll Learn
- Priority Groups: Elderly, healthcare workers, essential workers, and immunocompromised individuals are prioritized
- Age Eligibility: Specific age brackets determined by health authorities for vaccine rollout
- Health Conditions: Individuals with chronic illnesses or high-risk factors qualify early
- Occupation Criteria: Teachers, grocery workers, and first responders included in early phases
- Geographic Distribution: Vaccine availability based on regional population density and outbreak severity
![]()
Priority Groups: Elderly, healthcare workers, essential workers, and immunocompromised individuals are prioritized
The elderly, typically defined as individuals aged 65 and older, are consistently prioritized in vaccine distribution due to their heightened vulnerability to severe illness and mortality from infectious diseases. This group often faces age-related immune decline, known as immunosenescence, which reduces their ability to mount a robust response to vaccines. To address this, some vaccines, like the high-dose influenza vaccine (Fluzone High-Dose), contain four times the antigen of standard doses to enhance immunity. Practical tips for this group include scheduling vaccinations during quieter clinic hours to minimize stress and ensuring caregivers are informed about potential side effects, such as mild fever or soreness, which are normal and transient.
Healthcare workers form another critical priority group, not only because they face increased exposure to pathogens but also because their health directly impacts the continuity of medical services. This category includes doctors, nurses, pharmacists, and support staff like janitors and administrative personnel in healthcare settings. Vaccination protocols for this group often emphasize rapid deployment, with on-site clinics and mobile vaccination units to ensure minimal disruption to their work. For example, during the COVID-19 pandemic, healthcare workers were among the first to receive mRNA vaccines, with a recommended two-dose regimen spaced 3–4 weeks apart, followed by boosters every 6–12 months depending on variant circulation.
Essential workers, a broad category encompassing grocery store employees, teachers, public transit operators, and emergency responders, are prioritized to maintain societal functioning during outbreaks. Their roles require frequent public interaction, increasing their risk of infection and community spread. Vaccination strategies for this group often involve partnerships with employers to organize mass vaccination events or provide paid time off for appointments. For instance, some jurisdictions offered drive-through vaccination sites for transit workers, ensuring quick access without disrupting their schedules. A key consideration is tailoring communication to address vaccine hesitancy, emphasizing safety data and the collective benefit of herd immunity.
Immunocompromised individuals, including those with HIV, cancer patients undergoing chemotherapy, and organ transplant recipients, require special attention due to their suppressed immune systems. Standard vaccine doses may be less effective for this group, necessitating additional measures like extra doses or alternative formulations. For example, individuals with moderate to severe immunocompromise are advised to receive three primary doses of mRNA COVID-19 vaccines, followed by boosters at regular intervals. Clinicians should also consider serologic testing to assess antibody response post-vaccination and recommend additional precautions, such as masking and physical distancing, even after vaccination. Practical advice includes coordinating with specialists to time vaccinations optimally, such as scheduling doses between chemotherapy cycles when immune function is relatively higher.
Comparatively, while all priority groups share the goal of reducing severe outcomes, the rationale and approach differ. The elderly and immunocompromised benefit from enhanced vaccine formulations and additional doses, whereas healthcare and essential workers require rapid, accessible deployment to ensure societal stability. Each group’s vaccination strategy must balance individual protection with broader public health goals, highlighting the complexity of equitable vaccine distribution. By addressing these groups’ unique needs, public health systems can maximize the impact of vaccination campaigns and minimize disease burden across populations.
Washington Football Team's Vaccination Rate: How Many Players Are Vaccinated?
You may want to see also
Explore related products






![]()
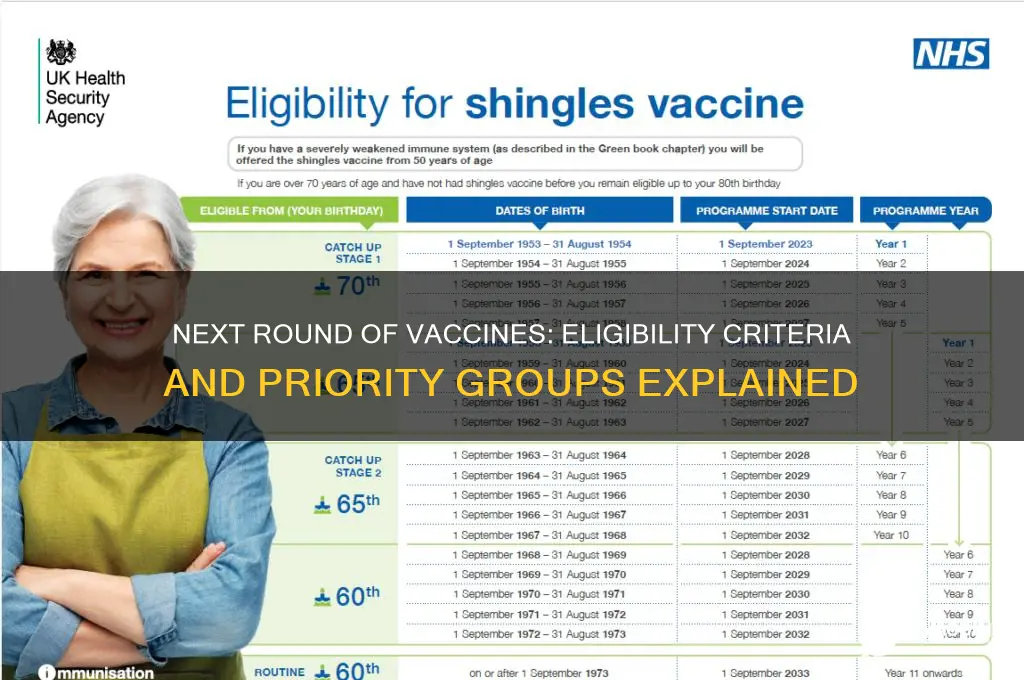
Age Eligibility: Specific age brackets determined by health authorities for vaccine rollout
Health authorities often prioritize age groups based on vulnerability and societal impact when rolling out vaccines. For instance, during the COVID-19 pandemic, many countries started with individuals aged 65 and older, as this demographic faced higher risks of severe illness and death. This phased approach ensures that limited vaccine supplies are allocated efficiently, protecting those most at risk first. Understanding these age brackets is crucial for individuals to know when they or their loved ones qualify for vaccination.
Determining age eligibility involves a balance between medical data and logistical feasibility. For example, children under 12 were among the last to receive COVID-19 vaccines due to the need for additional safety studies and lower dosage formulations. In contrast, adolescents aged 12–17 were approved for vaccination sooner, but with specific guidelines, such as receiving the Pfizer-BioNTech vaccine, which was the first to be authorized for this age group. Parents and caregivers must stay informed about these distinctions to ensure timely vaccination for eligible family members.
Practical tips can help navigate age-based vaccine rollouts. First, monitor official health department websites or sign up for alerts to receive updates on eligibility expansions. Second, prepare necessary documentation, such as proof of age or residency, when scheduling appointments. For younger age groups, like teenagers, ensure caregivers are aware of any required parental consent forms. Lastly, be patient but proactive; eligibility criteria can change rapidly as vaccine supplies increase and new data emerges.
Comparing age eligibility across different vaccines highlights the importance of tailored approaches. For instance, the flu vaccine is typically recommended for all individuals aged 6 months and older, with no upper age limit, whereas COVID-19 vaccines had stricter age brackets initially. Such differences underscore the need for public awareness campaigns that clarify which vaccines are appropriate for specific age groups. This clarity helps prevent confusion and ensures widespread protection across all eligible populations.
In conclusion, age eligibility is a cornerstone of vaccine rollout strategies, designed to maximize impact and protect the most vulnerable. By staying informed, preparing necessary documentation, and understanding the nuances of different vaccines, individuals can navigate these phased rollouts effectively. Health authorities must continue to communicate these age brackets clearly to build trust and ensure equitable access to life-saving vaccines.
Vaccination Requirements for Aspiring Marine Recruits
You may want to see also
Explore related products






![]()
Health Conditions: Individuals with chronic illnesses or high-risk factors qualify early
Chronic illnesses and high-risk health factors significantly elevate vulnerability to severe outcomes from vaccine-preventable diseases. Conditions like diabetes, heart disease, chronic lung disease, and immunocompromised states—whether from cancer treatment, organ transplants, or HIV—place individuals at heightened risk. For instance, diabetics are three times more likely to experience severe complications from influenza, while those with chronic lung conditions face increased hospitalization rates from respiratory infections. Recognizing this, vaccine allocation strategies prioritize these groups to mitigate risks and reduce strain on healthcare systems.
Prioritizing individuals with chronic illnesses requires clear guidelines and practical implementation. For example, the CDC recommends that adults with asthma, COPD, or cystic fibrosis receive annual influenza vaccines and prioritize COVID-19 boosters. Similarly, those with heart conditions or stroke history should follow accelerated vaccine schedules, often receiving doses 4–6 weeks earlier than the general population. Practical tips include scheduling appointments during stable health periods, ensuring caregivers are also vaccinated, and carrying a medical ID card detailing conditions and vaccine status for emergency reference.
A comparative analysis reveals disparities in how countries address this priority group. While the U.S. and U.K. explicitly list chronic conditions in their vaccine rollout phases, some low-income nations struggle to identify and reach these individuals due to fragmented healthcare systems. For instance, India’s CoWIN platform allows self-declaration of comorbidities but relies on individuals to upload medical certificates, creating barriers for those without digital access. In contrast, Israel’s centralized health system proactively contacted high-risk patients, achieving 90% vaccination rates among eligible chronically ill citizens within three months.
Persuading policymakers to maintain this priority requires emphasizing cost-effectiveness and equity. Studies show that vaccinating high-risk individuals reduces hospitalizations by up to 60%, saving healthcare costs and freeing resources for other critical needs. Moreover, early access to vaccines for this group aligns with ethical frameworks prioritizing those with the least ability to withstand infection. Advocacy efforts should highlight success stories, such as how Canada’s targeted approach to immunocompromised patients lowered ICU admissions by 40% during the Omicron wave, reinforcing the lifesaving impact of such policies.
Vaccine Injuries: Anger Issues in Children
You may want to see also
Explore related products






![]()
Occupation Criteria: Teachers, grocery workers, and first responders included in early phases
As vaccination efforts expand, occupation-based criteria are becoming a critical factor in determining who qualifies for the next round of vaccines. Teachers, grocery workers, and first responders are among the essential workers now included in early phases of vaccine distribution. This prioritization reflects their heightened exposure to COVID-19 and their role in maintaining societal function. For instance, teachers interact daily with students in crowded classrooms, while grocery workers face constant contact with the public, often in enclosed spaces. First responders, including police officers, firefighters, and EMTs, are at immediate risk due to their emergency duties. Recognizing these risks, health authorities have categorized these professions as high-priority, ensuring they receive vaccines sooner to protect both themselves and the communities they serve.
From a logistical standpoint, vaccinating these occupational groups requires careful planning. Teachers, for example, are often grouped by school district or union affiliation, making it easier to coordinate mass vaccination events. Grocery workers, employed by large chains or smaller stores, may require partnerships with employers to schedule vaccinations during off-peak hours. First responders, already part of structured organizations, can be vaccinated through their departments, often in dedicated clinics. Practical tips include ensuring these workers have access to flexible scheduling to accommodate potential side effects, such as fatigue or mild fever after receiving doses like the Pfizer-BioNTech or Moderna vaccines, which require two shots spaced 3–4 weeks apart. Clear communication about eligibility and registration processes is also essential to avoid confusion and ensure equitable access.
The inclusion of these occupations in early phases is not just a public health decision but also a societal one. By protecting teachers, schools can remain open, minimizing disruptions to education and allowing parents to return to work. Vaccinating grocery workers ensures the stability of food supply chains, a critical service during the pandemic. First responders, vaccinated and healthy, can continue to provide life-saving services without fear of becoming vectors for the virus. This approach aligns with the Centers for Disease Control and Prevention (CDC) guidelines, which emphasize reducing morbidity and mortality while preserving societal function. It also addresses ethical concerns by prioritizing those who face unavoidable risks due to their jobs, rather than those who can mitigate exposure through remote work or other means.
Comparatively, occupation-based criteria differ from age-based or health-condition criteria in their focus on societal role rather than individual vulnerability. While older adults and those with comorbidities remain top priorities due to their higher risk of severe illness, essential workers are prioritized for their collective impact on community health and infrastructure. This dual approach ensures that vaccines serve both individual and communal goals. For example, a 30-year-old teacher might receive the vaccine before a 50-year-old remote worker, even though the latter falls into a higher-risk age category. This strategy underscores the interconnectedness of public health and economic stability, making occupation-based criteria a cornerstone of phased vaccine distribution.
Understanding the Rarity of Child Deaths from Vaccine Injuries
You may want to see also
Explore related products


![]()
Geographic Distribution: Vaccine availability based on regional population density and outbreak severity
In regions with high population density, vaccine distribution strategies must prioritize rapid deployment to prevent exponential spread. Urban centers, where individuals live and work in close proximity, become hotspots for transmission. For instance, a city with a population density of 10,000 people per square mile may require a phased rollout, starting with essential workers and those over 65, followed by younger age groups. This approach ensures that the most vulnerable are protected first while gradually building herd immunity. Practical tips include setting up mobile vaccination units in densely populated neighborhoods and extending clinic hours to accommodate working populations.
Contrastingly, rural areas with lower population density face unique challenges, such as limited healthcare infrastructure and longer travel distances. In these regions, outbreak severity often dictates vaccine allocation. For example, a rural county experiencing a sudden surge in cases might receive a higher proportion of doses per capita compared to a neighboring county with fewer cases. To address accessibility, rural distribution plans should include partnerships with local pharmacies, community centers, and even door-to-door vaccination drives for the elderly or immobile. A single-dose vaccine like Johnson & Johnson’s may be prioritized in these areas to simplify logistics and ensure broader coverage.
Analyzing outbreak severity alongside population density reveals a dynamic allocation model. For instance, a moderately dense suburban area with a rapidly escalating outbreak should receive expedited vaccine shipments, even if nearby urban centers have higher absolute case numbers. This approach requires real-time data monitoring and flexible supply chains. Health authorities can use predictive modeling to anticipate hotspots, ensuring vaccines are pre-positioned where they’re most needed. A key takeaway is that geographic distribution isn’t just about population size—it’s about understanding the interplay between density and outbreak dynamics to maximize impact.
Persuasively, policymakers must resist the urge to allocate vaccines solely based on population size or political pressure. Instead, they should adopt a data-driven approach that considers both density and outbreak severity. For example, a region with a population of 500,000 but a 20% positivity rate should receive priority over a region of 1 million with a 2% rate. This strategy not only saves lives but also prevents overwhelmed healthcare systems. By communicating this rationale transparently, public trust can be maintained, even if certain areas receive vaccines earlier than others. Practical steps include publishing allocation criteria and regularly updating the public on distribution progress.
Descriptively, imagine a map where vaccine distribution is visualized as a series of concentric circles, with the most densely populated and severely affected areas at the center. Outer rings represent regions with lower density or milder outbreaks, receiving vaccines in subsequent phases. This model ensures that resources are allocated efficiently, creating a ripple effect of protection. For instance, a 10-mile radius around a major outbreak zone might receive 50% of available doses in the first phase, while surrounding areas receive 30% and 20% in phases two and three, respectively. Such a visual framework can guide both policymakers and the public in understanding the logic behind geographic distribution.
Fever After 2-Month Vaccines: Timing, Causes, and What to Expect
You may want to see also
Frequently asked questions
Eligibility for the next round of vaccines typically depends on local health guidelines, but it often includes individuals in priority groups such as healthcare workers, the elderly, those with underlying health conditions, and essential workers.
Eligibility for children depends on vaccine approvals for specific age groups. Once a vaccine is approved for children, they may qualify based on age and local health recommendations.
In many cases, the next round of vaccines may include booster shots for those who have already received their initial doses. However, some programs may also target unvaccinated individuals, depending on supply and demand.
Check with your local health department, healthcare provider, or government websites for updates on eligibility criteria and registration processes.
Yes, individuals with pre-existing conditions are often prioritized due to their higher risk of severe illness. Consult your healthcare provider or local guidelines for specific eligibility details.