The World Health Organization (WHO) has published a position paper on Haemophilus influenzae type b (Hib) conjugate vaccines, emphasizing their critical role in preventing Hib-related diseases, such as meningitis, pneumonia, and epiglottitis, which disproportionately affect young children in low- and middle-income countries. The paper highlights the significant reduction in Hib disease burden following the introduction of Hib vaccines into national immunization programs, underscoring their safety, efficacy, and cost-effectiveness. WHO recommends the inclusion of Hib conjugate vaccines in routine infant immunization schedules, advocating for sustained global efforts to improve vaccine access and coverage to further decrease morbidity and mortality associated with Hib infections. This position paper serves as a vital resource for policymakers, healthcare providers, and stakeholders working to strengthen immunization programs and protect vulnerable populations from this preventable disease.
Explore related products






What You'll Learn
![]()
Vaccine efficacy in preventing Hib diseases
Haemophilus influenzae type b (Hib) conjugate vaccines have demonstrated remarkable efficacy in preventing invasive Hib diseases, which include conditions such as meningitis, pneumonia, and epiglottitis. Clinical trials and post-introduction studies consistently show that these vaccines provide robust protection, particularly in young children who are most vulnerable to Hib infections. For instance, a meta-analysis of randomized controlled trials found that Hib conjugate vaccines were 95–100% effective in preventing invasive Hib diseases in infants and young children when administered as part of a primary series. This high efficacy underscores the critical role of these vaccines in reducing the global burden of Hib-related morbidity and mortality.
The timing and dosage of Hib conjugate vaccines are crucial for maximizing their protective effects. The World Health Organization (WHO) recommends a primary series of two or three doses, depending on the specific vaccine formulation, starting as early as 6 weeks of age. A booster dose is often administered between 12 and 15 months to enhance long-term immunity. For example, the *PRP-T* (a Hib conjugate vaccine) is typically given in a 3-dose schedule at 2, 4, and 6 months, followed by a booster at 12–15 months. Adhering to this schedule ensures optimal immune response and sustained protection against Hib diseases throughout childhood.
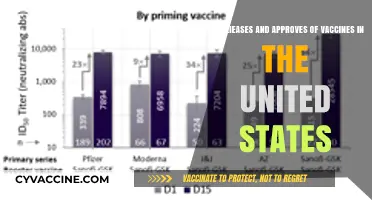
Comparative studies highlight the superiority of Hib conjugate vaccines over earlier polysaccharide vaccines, which were less immunogenic and ineffective in children under 2 years of age. Conjugate vaccines, by linking Hib polysaccharides to carrier proteins, elicit a T-cell-dependent immune response, enabling infants to develop robust and lasting immunity. This innovation has been pivotal in reducing Hib disease incidence by over 90% in countries with high vaccination coverage. For example, the United States, which introduced Hib conjugate vaccines in the early 1990s, saw a dramatic decline in Hib meningitis cases from approximately 20,000 annually to fewer than 50 cases per year.
Despite their proven efficacy, challenges remain in ensuring equitable access to Hib conjugate vaccines globally. In low-income countries, where the burden of Hib diseases is highest, vaccine coverage is often suboptimal due to logistical barriers, limited healthcare infrastructure, and funding constraints. Strengthening immunization programs, improving cold chain management, and advocating for sustainable financing are essential steps to bridge this gap. Practical tips for healthcare providers include educating caregivers about the importance of completing the full vaccine series, monitoring for rare adverse reactions (such as mild fever or local pain), and integrating Hib vaccination with other routine immunizations to maximize efficiency.
In conclusion, the efficacy of Hib conjugate vaccines in preventing invasive diseases is well-established, making them a cornerstone of childhood immunization programs. By adhering to recommended schedules, addressing global disparities in access, and leveraging lessons from successful implementations, the international community can further reduce the burden of Hib diseases and save countless lives.
Empowering Young Lives: The Essential Role of Vaccines Before School
You may want to see also
Explore related products






![]()
Target populations for immunization programs
The World Health Organization (WHO) emphasizes that the primary target population for Haemophilus influenzae type b (Hib) conjugate vaccines is infants, as they are at the highest risk of invasive Hib disease. The immunization schedule typically begins at 6 weeks of age, with a primary series of 2 or 3 doses administered 4 to 8 weeks apart, depending on the specific vaccine formulation. For example, the *PRP-T* (ActHIB) and *PRP-OMP* (PedvaxHIB) vaccines require a 2-dose series, while *HbOC* (Hiberix) and *PRP-D* (Comvax) follow a 3-dose regimen. A booster dose is recommended at 12–15 months of age to ensure long-term immunity, particularly in regions with persistent Hib circulation.
In settings with high disease burden or delayed access to healthcare, catch-up vaccination for older children is crucial. The WHO recommends a single dose of Hib vaccine for children aged 12–59 months in countries where routine infant immunization has been introduced but coverage remains suboptimal. However, for children aged 5 years and older, Hib vaccination is generally not recommended unless they have specific risk factors, such as asplenia or immunocompromising conditions. This targeted approach ensures that resources are allocated efficiently to populations most vulnerable to Hib-related morbidity and mortality.
A comparative analysis of immunization strategies reveals that countries with high routine coverage in infants have successfully reduced Hib disease incidence across all age groups, a phenomenon known as herd immunity. For instance, the United States and the United Kingdom experienced a >90% decline in Hib cases following the introduction of Hib conjugate vaccines in the 1990s. In contrast, low- and middle-income countries with inconsistent vaccine supply or low coverage continue to report significant Hib-related hospitalizations and deaths, underscoring the importance of strengthening immunization programs in these regions.
Practical implementation of Hib vaccination programs requires careful consideration of local epidemiology, healthcare infrastructure, and vaccine affordability. For example, in areas with limited cold chain capacity, the use of thermostable Hib vaccines could improve accessibility. Additionally, integrating Hib vaccination with other routine immunizations, such as diphtheria-tetanus-pertussis (DTP) or pneumococcal conjugate vaccines, can enhance coverage and reduce logistical challenges. Health workers should also be trained to educate caregivers about the importance of completing the full vaccine series and adhering to the recommended schedule.
Finally, monitoring and evaluation are essential to assess the impact of Hib immunization programs. Surveillance systems should track both vaccine coverage and disease incidence to identify gaps and guide policy adjustments. For instance, serotype replacement or vaccine failures should prompt investigations into potential causes, such as waning immunity or genetic changes in Hib strains. By focusing on evidence-based strategies and continuous improvement, public health officials can maximize the benefits of Hib conjugate vaccines for target populations worldwide.
Discovering France's COVID-19 Vaccine: Name, Development, and Global Impact
You may want to see also
Explore related products






![]()
Dosage and administration guidelines
The World Health Organization's position paper on Haemophilus influenzae type b (Hib) conjugate vaccines emphasizes the critical role of proper dosage and administration to ensure optimal protection against Hib diseases, particularly in infants and young children. The recommended dosage regimen varies by vaccine product and age group, reflecting the need for tailored approaches to immunization. For instance, most Hib conjugate vaccines are administered in a 2- or 3-dose primary series, typically starting at 6 weeks of age, with doses given at least 4 weeks apart. A booster dose is often recommended between 12 and 15 months of age to enhance long-term immunity. This structured schedule ensures that children develop robust protection during their most vulnerable period.
One key consideration in dosage and administration is the vaccine's formulation and its compatibility with other vaccines. Hib conjugate vaccines are frequently combined with other antigens, such as diphtheria, tetanus, pertussis, and hepatitis B, in a single injection to simplify immunization programs. When administering combination vaccines, healthcare providers must adhere to the specific dosage instructions for each component to avoid underdosing or overdosing. For example, a combination vaccine like DTP-HepB-Hib may require a 3-dose primary series followed by a booster, while a standalone Hib vaccine might follow a different schedule. This flexibility allows for integration into existing national immunization programs while maintaining efficacy.
Age-specific guidelines are another critical aspect of Hib vaccine administration. In infants, the immune response to Hib conjugate vaccines is highly effective, with seroprotection rates exceeding 95% after the primary series. However, in older children and adults, particularly those with underlying conditions like asplenia or HIV, the dosage and need for vaccination may differ. For example, individuals with compromised immune systems may require additional doses or higher antigen content to achieve adequate immunity. Healthcare providers must assess each patient's risk factors and medical history to determine the most appropriate vaccination strategy.
Practical tips for administration include ensuring proper storage and handling of vaccines to maintain potency. Hib conjugate vaccines should be stored at 2°C to 8°C and protected from light. Before administration, the vaccine should be inspected for discoloration or particulate matter, and the correct dosage should be drawn into a sterile syringe. Injection technique is also important; the vaccine should be administered intramuscularly, typically into the vastus lateralis muscle in infants and young children, to minimize pain and adverse reactions. Proper documentation of the vaccine type, dose, and administration date is essential for tracking immunization status and planning future doses.
In conclusion, adherence to dosage and administration guidelines is paramount for the success of Hib conjugate vaccination programs. By following age-specific schedules, using appropriate combinations, and ensuring correct technique, healthcare providers can maximize the vaccine's impact in preventing Hib-related diseases. These guidelines not only protect individual recipients but also contribute to herd immunity, reducing the overall burden of Hib infections in communities. As immunization programs evolve, ongoing training and updates for healthcare workers remain essential to maintain high standards of vaccine delivery.
Post-Vaccine Intimacy: Is It Safe to Have Sex After Your Shot?
You may want to see also
Explore related products






![]()
Safety and adverse event monitoring
The WHO's position paper on Haemophilus influenzae type b (Hib) conjugate vaccines underscores the importance of robust safety and adverse event monitoring systems to ensure public trust and vaccine efficacy. Post-licensure surveillance is critical, as clinical trials, while comprehensive, may not capture rare or long-term adverse events. For instance, the paper highlights that Hib vaccines have been administered to millions of infants globally, with systemic adverse events such as fever and local reactions (e.g., redness, swelling) being the most commonly reported. These reactions are typically mild and resolve within 48 hours, aligning with the vaccine’s safety profile. However, the rarity of severe events like anaphylaxis necessitates ongoing vigilance through active monitoring systems.
To effectively monitor adverse events, the WHO recommends a multi-tiered approach. Passive surveillance systems, where healthcare providers report suspected adverse events, are foundational but rely on voluntary participation and may underreport. Active surveillance, such as the use of sentinel sites or population-based studies, provides more comprehensive data. For example, the Global Advisory Committee on Vaccine Safety (GACVS) has reviewed data from countries like the Gambia and Chile, where Hib vaccines were introduced in the 1990s, confirming their safety and identifying no significant long-term risks. Implementing such systems in low-resource settings, however, requires capacity-building and standardized reporting tools to ensure data reliability.
A key challenge in adverse event monitoring is distinguishing vaccine-related events from coincidental illnesses, particularly in infants who receive multiple vaccines simultaneously. The WHO emphasizes the use of standardized case definitions and causality assessment tools to improve accuracy. For instance, fever within 24 hours of vaccination is common but rarely a cause for concern unless accompanied by other symptoms. Healthcare providers should educate caregivers about expected reactions and when to seek medical attention, such as persistent crying, lethargy, or high fever (>40°C). Clear communication reduces anxiety and enhances trust in vaccination programs.
Practical tips for healthcare providers include documenting vaccination details (date, dose, manufacturer) and encouraging caregivers to report any unusual symptoms promptly. National immunization programs should integrate adverse event monitoring into routine activities, ensuring timely reporting to regional or global databases like the Vaccine Adverse Event Reporting System (VAERS). For Hib conjugate vaccines, specific attention should be given to monitoring in high-risk groups, such as preterm infants or those with underlying conditions, as their immune responses may differ. Regular reviews of safety data by regulatory bodies and the WHO ensure that any emerging concerns are addressed swiftly, maintaining the vaccine’s proven track record of safety.
In conclusion, safety and adverse event monitoring for Hib conjugate vaccines require a proactive, structured approach that combines passive and active surveillance, standardized reporting, and clear communication. By prioritizing these measures, public health systems can continue to deliver Hib vaccines with confidence, protecting millions of children from this once-devastating disease while minimizing risks and maintaining transparency.
The Smallpox Vaccine: Why It Leaves a Unique Scar
You may want to see also
Explore related products






![]()
Global implementation and impact assessment
The global rollout of Haemophilus influenzae type b (Hib) conjugate vaccines has been a cornerstone of public health efforts to combat childhood morbidity and mortality. Since the World Health Organization (WHO) first recommended Hib vaccination in 1998, over 190 countries have introduced the vaccine into their national immunization programs. This widespread adoption underscores the vaccine’s efficacy in preventing Hib-related diseases, such as meningitis and pneumonia, which disproportionately affect children under five. However, implementation disparities persist, particularly in low-income regions where vaccine access and infrastructure challenges remain significant barriers.
A critical aspect of global implementation is the integration of Hib vaccines into routine immunization schedules. WHO guidelines recommend a primary series of two or three doses, depending on the vaccine formulation, starting at 6 weeks of age, followed by a booster dose at 12–15 months. For example, the *PRP-T* (ActHIB) and *HbOC* (HibTITER) vaccines typically require three doses, while *PRP-OMP* (PedvaxHIB) is administered in two doses. In settings with high Hib disease burden, early initiation of vaccination is crucial, as infants are most vulnerable during the first year of life. Practical tips for healthcare providers include ensuring cold chain maintenance to preserve vaccine potency and using prefilled syringes to minimize wastage and administration errors.
Impact assessments reveal a dramatic reduction in Hib-related diseases in countries with high vaccination coverage. For instance, studies in the Gambia and Chile demonstrated a 90% decline in Hib meningitis cases within three years of vaccine introduction. However, measuring impact in low-resource settings is complicated by limited disease surveillance systems. WHO emphasizes the importance of strengthening surveillance networks to accurately track Hib disease incidence and vaccine effectiveness. Comparative analyses show that countries with robust surveillance systems, such as Bangladesh and Kenya, have been more successful in demonstrating the vaccine’s impact and advocating for sustained funding.
Despite successes, challenges in global implementation persist. Vaccine affordability remains a hurdle, though initiatives like Gavi, the Vaccine Alliance, have subsidized Hib vaccines for eligible countries. Another issue is public hesitancy, driven by misinformation or lack of awareness about Hib disease severity. Persuasive communication strategies, such as community engagement campaigns and healthcare worker training, are essential to address these concerns. For example, in India, a nationwide campaign highlighting the life-threatening risks of Hib meningitis significantly improved vaccine uptake in rural areas.
In conclusion, the global implementation of Hib conjugate vaccines has transformed child health outcomes, but equitable access and sustained impact require continued effort. Policymakers must prioritize strengthening health systems, ensuring vaccine affordability, and fostering public trust. By learning from successful models and addressing persistent gaps, the global community can further reduce the burden of Hib disease and move closer to the WHO’s vision of universal immunization coverage.
Armpit Pain After Pneumonia Vaccine: Normal or Cause for Concern?
You may want to see also
Frequently asked questions
The WHO strongly recommends the inclusion of Hib conjugate vaccines in routine childhood immunization programs globally to prevent Hib-related diseases, such as meningitis and pneumonia.
The WHO recommends starting Hib vaccination as early as 6 weeks of age, with a primary series of 2 or 3 doses, depending on the vaccine formulation, followed by a booster dose in the second year of life.
Yes, Hib conjugate vaccines are considered safe and well-tolerated. Common side effects are mild and include pain at the injection site, fever, and irritability.
Yes, the WHO recommends Hib vaccination in all countries, regardless of disease burden, due to the vaccine's effectiveness in preventing severe Hib-related diseases and its cost-effectiveness.
Yes, Hib conjugate vaccines can be safely co-administered with other routine childhood vaccines, such as DTP (diphtheria, tetanus, pertussis), hepatitis B, and pneumococcal conjugate vaccines.