The question of who is paying for COVID-19 vaccines in the United States is a critical aspect of the nation’s public health response to the pandemic. While the federal government, through initiatives like the Coronavirus Aid, Relief, and Economic Security (CARES) Act and the American Rescue Plan, has allocated billions of dollars to fund vaccine development, procurement, and distribution, the financial burden is shared across multiple entities. State and local governments play a role in administering vaccines, often using federal grants to cover operational costs. Additionally, private insurers and government programs like Medicare and Medicaid cover vaccination expenses for their beneficiaries, ensuring that individuals face no out-of-pocket costs. This collaborative funding model reflects a concerted effort to make vaccines widely accessible and to mitigate the economic impact of the pandemic on both individuals and the healthcare system.
| Characteristics | Values |
|---|---|
| Funding Source | Federal Government |
| Program | COVID-19 Vaccination Program |
| Cost Coverage | Free for all individuals, regardless of insurance status |
| Legislation | Coronavirus Aid, Relief, and Economic Security (CARES) Act, Coronavirus Response and Relief Supplemental Appropriations Act, American Rescue Plan Act |
| Total Funding (as of 2023) | Over $18 billion allocated for vaccine procurement and distribution |
| Vaccine Providers | Pharmacies, healthcare providers, state/local health departments, community health centers, and other qualified entities |
| Reimbursement | Providers are reimbursed by the federal government for administering vaccines |
| Insurance Requirements | No cost-sharing (e.g., copays, deductibles) for patients |
| Uninsured Individuals | Covered by the Health Resources and Services Administration (HRSA) COVID-19 Uninsured Program |
| State Role | States manage distribution and administration, but funding is primarily federal |
| Private Sector Involvement | Vaccine manufacturers are paid by the federal government for doses purchased |
| Ongoing Support | Continued federal funding for booster shots, pediatric vaccines, and future variants |
Explore related products






What You'll Learn
![]()
Federal funding sources for vaccines
The U.S. federal government has played a pivotal role in funding COVID-19 vaccines, ensuring widespread accessibility without direct cost to individuals. Through initiatives like Operation Warp Speed, launched in 2020, the government allocated over $10 billion to accelerate vaccine development and manufacturing. This funding enabled companies like Pfizer, Moderna, and Johnson & Johnson to produce vaccines at an unprecedented pace. Notably, the government purchased hundreds of millions of doses upfront, guaranteeing availability and removing financial barriers for recipients. This strategy not only expedited vaccine distribution but also mitigated risks for manufacturers, fostering rapid innovation.
Beyond development, federal funding has covered vaccination administration costs, particularly for uninsured individuals and those with limited coverage. The Provider Relief Fund, part of the CARES Act, allocated billions to healthcare providers administering vaccines, ensuring they were reimbursed for their services. Additionally, the Centers for Disease Control and Prevention (CDC) partnered with state and local health departments to establish community vaccination sites, mobile clinics, and outreach programs. These efforts were critical in reaching underserved populations, including rural areas and communities of color, where vaccine hesitancy and access issues were most pronounced.
A lesser-known federal funding source is the Vaccines for Children (VFC) program, which, while primarily focused on pediatric immunizations, has been adapted to support COVID-19 vaccine distribution for eligible children. This program ensures that children from low-income families receive vaccines at no cost, with the federal government purchasing doses and distributing them to providers. For COVID-19, this framework was expanded to include adolescents aged 12 and older, following FDA approval for Pfizer’s vaccine in this age group. Providers participating in the VFC program are reimbursed for administrative costs, further reducing financial burdens on families and healthcare systems.
Federal funding has also supported ongoing research and monitoring of vaccine safety and efficacy. The CDC’s Immunization Safety Office and the FDA’s post-authorization safety surveillance systems rely on federal dollars to track adverse events and ensure public confidence in vaccines. For instance, the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) are federally funded tools that monitor real-world vaccine outcomes. These systems were instrumental in identifying rare side effects, such as myocarditis in young males post-vaccination, allowing for swift public health responses and updated guidelines.
In summary, federal funding sources for vaccines in the U.S. encompass development, distribution, administration, and safety monitoring. By investing billions in these areas, the government has not only facilitated the creation of life-saving vaccines but also ensured equitable access and public trust. Practical tips for individuals include verifying eligibility for no-cost vaccines through local health departments or community clinics and staying informed about booster recommendations via CDC guidelines. This comprehensive federal approach underscores the critical role of public investment in safeguarding public health.
Shingrix Vaccine: Cold Sore Relief?
You may want to see also
Explore related products






![]()
State and local contributions to vaccine costs
State and local governments play a pivotal role in ensuring vaccine accessibility, often stepping in to cover costs that federal programs don’t fully address. For instance, while the federal government funds vaccines for uninsured adults through the Provider Relief Fund, states like California and New York have allocated additional budgets to cover administrative costs, such as staffing vaccination sites and outreach programs. These contributions are critical in bridging gaps, especially in underserved communities where federal funding alone may fall short. Without such state-level support, vaccination rates could stagnate, leaving vulnerable populations at risk.
Consider the logistics: administering a single dose of the Pfizer or Moderna vaccine involves more than just the vial’s cost, which ranges from $15 to $20. States often fund the storage of mRNA vaccines at ultra-cold temperatures (-70°C for Pfizer), a requirement that smaller clinics cannot always meet without financial aid. Local health departments also cover transportation costs for mobile vaccination units, ensuring rural areas aren’t left behind. For example, Texas deployed over 50 mobile teams in 2021, funded entirely by state allocations, to reach residents in remote counties. These efforts highlight how state contributions extend beyond direct vaccine purchases to include infrastructure and accessibility.
A persuasive argument emerges when examining the return on investment for state and local vaccine funding. By preventing outbreaks, states reduce the economic burden of hospitalizations, which can cost upwards of $20,000 per COVID-19 patient. For instance, Michigan’s $50 million investment in vaccine distribution in 2021 likely averted thousands of hospitalizations, saving the state an estimated $200 million in healthcare costs. This proactive approach not only protects public health but also stabilizes local economies by keeping businesses open and workers healthy. Critics of such spending overlook the long-term savings and societal benefits.
Comparatively, states with higher contributions to vaccine costs tend to have more equitable distribution rates. In Illinois, where the state allocated $10 million for community-based vaccination programs, minority vaccination rates increased by 15% within six months. Contrast this with states that relied solely on federal funding, where disparities persisted. This data underscores the importance of localized efforts in tailoring solutions to specific community needs. States that invest in culturally competent outreach, such as multilingual materials or partnerships with trusted community leaders, see faster and more inclusive vaccine uptake.
Finally, a practical tip for local governments: leverage federal programs like the Vaccines for Children (VFC) program, which provides free vaccines to eligible children, but supplement them with state-funded initiatives targeting hesitant populations. For example, offering small incentives like $25 gift cards or free transportation to vaccination sites can significantly boost participation. States can also collaborate with pharmacies and schools to host on-site clinics, reducing barriers to access. By combining federal resources with targeted local strategies, states can maximize their impact and ensure no one is left behind in the vaccination effort.
Adult Chickenpox Vaccination: Benefits, Risks, and Wise Considerations
You may want to see also
Explore related products






![]()
Role of private insurance in vaccine payments
Private insurance plays a pivotal role in the U.S. vaccine payment landscape, serving as a critical intermediary between healthcare providers and patients. Under the Affordable Care Act (ACA), most private insurance plans are required to cover recommended vaccines without cost-sharing, meaning patients typically pay nothing out-of-pocket for FDA-approved vaccines administered by in-network providers. This includes routine immunizations like the annual flu shot, childhood vaccines (e.g., MMR, DTaP), and newer vaccines such as the COVID-19 series. For adults aged 65 and older, private insurance often covers additional vaccines like shingles (Shingrix) and pneumococcal shots, though dosage schedules may vary based on health status.
However, the system is not without its complexities. Private insurers negotiate reimbursement rates with vaccine manufacturers and providers, which can influence the availability of certain vaccines within their networks. For instance, while the COVID-19 vaccine was free to all Americans during the public health emergency, private insurers now handle payment for booster doses, with coverage dependent on FDA and CDC recommendations. This shift underscores the insurer’s role in balancing public health needs with financial sustainability. Patients should verify coverage details, as some plans may exclude specific vaccines or require prior authorization for certain age groups or high-dose formulations.
A comparative analysis reveals that private insurance coverage for vaccines contrasts sharply with the underinsured or uninsured population, who rely on programs like the Vaccine for Children (VFC) or community health centers. For insured individuals, the process is streamlined: providers bill insurers directly, and patients receive vaccines at no cost during preventive care visits. Yet, gaps exist. Travel vaccines (e.g., yellow fever) or off-label uses of vaccines are often excluded from coverage, leaving patients to pay out-of-pocket. This highlights the need for clearer policy guidelines and expanded coverage criteria.
To navigate this system effectively, patients should take proactive steps. First, review your insurance plan’s vaccine coverage annually, as formularies and networks may change. Second, ensure your provider is in-network to avoid unexpected costs. Third, keep a record of vaccinations, as some insurers require documentation for reimbursement or to avoid duplicate doses. For families, confirm that pediatricians participate in the VFC program as a backup if insurance coverage is inadequate. Finally, advocate for policy reforms that standardize vaccine coverage across all insurers, ensuring equitable access regardless of plan type.
In conclusion, private insurance is a cornerstone of vaccine payment in the U.S., offering broad coverage but requiring vigilance from patients and providers. By understanding its mechanisms and limitations, individuals can maximize benefits while pushing for systemic improvements to close coverage gaps.
From Lab to Injection: The Comprehensive Stages of Vaccine Creation
You may want to see also
Explore related products






![]()
Out-of-pocket costs for uninsured individuals
Uninsured individuals in the U.S. face a unique challenge when it comes to vaccine costs, as they lack the safety net of insurance coverage to offset expenses. Unlike insured patients, who typically pay little to nothing for recommended vaccines, the uninsured must navigate a patchwork of pricing structures, assistance programs, and out-of-pocket costs that vary widely by location, vaccine type, and provider. For example, a single dose of the Pfizer-BioNTech COVID-19 vaccine can cost up to $50 at some pharmacies, while the shingles vaccine (Shingrix) may run as high as $200 per dose, with two doses required for full immunization.
To minimize out-of-pocket costs, uninsured individuals should first explore federally funded programs like the Vaccines for Children (VFC) program, which provides free vaccines to eligible children, or the Bridge Access Program for COVID-19 vaccines, which offers no-cost options through participating pharmacies. Additionally, community health centers often provide vaccines at reduced rates based on income. For adults, manufacturer assistance programs, such as GSK’s Vaccines Access Program, may offer discounts or free doses for vaccines like Shingrix or Tdap. Proactively researching these options can significantly reduce financial burden.
A comparative analysis reveals that while some vaccines, like the annual flu shot, are often available for $0–$50 at retail pharmacies, others, such as the HPV vaccine (Gardasil 9), can cost upwards of $250 per dose, with a three-dose series totaling $750. This disparity highlights the importance of prioritizing vaccines based on risk factors and age recommendations. For instance, uninsured young adults should consider the HPV vaccine a high priority due to its role in preventing cancers, while older adults might focus on shingles and pneumonia vaccines (Pneumovax 23 or Prevnar 20) to avoid costly complications.
Persuasively, uninsured individuals must also be aware of hidden costs, such as administration fees, which can add $15–$25 per vaccine dose. To counter this, consider bundling vaccines during a single visit to reduce overall fees. For example, getting a Tdap and flu shot together can save both time and money. Furthermore, negotiating prices directly with providers or pharmacies can sometimes yield discounts, especially when paying in cash upfront. Practical tips include asking for the cash price, which is often lower than the billed rate, and inquiring about sliding-scale fees at local clinics.
In conclusion, while out-of-pocket costs for vaccines can be daunting for uninsured individuals, strategic planning and resource utilization can mitigate expenses. By leveraging federal programs, manufacturer assistance, and cost-saving strategies, the uninsured can access essential vaccines without incurring overwhelming financial strain. Prioritizing vaccines based on age and health risks, coupled with proactive research, ensures protection without breaking the bank.
Vaccinated US Flights: Is Testing No Longer a Requirement?
You may want to see also
Explore related products






![]()
International and NGO support for U.S. vaccines
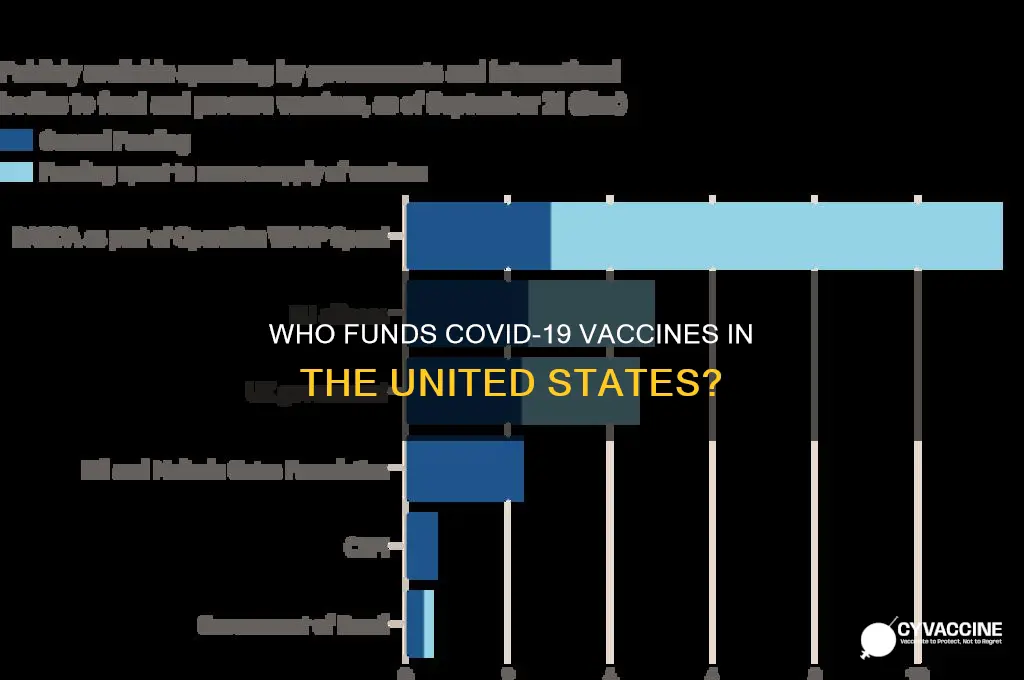
The U.S. vaccine rollout, while primarily funded domestically, has received significant international and NGO support, particularly in addressing inequities and reaching underserved populations. Organizations like Gavi, the Vaccine Alliance, have played a pivotal role by ensuring global vaccine access, indirectly benefiting the U.S. through reduced global transmission risks. For instance, Gavi’s COVAX initiative, though focused on low-income countries, has contributed to stabilizing the global supply chain, which has had ripple effects on U.S. vaccine availability. Additionally, NGOs like the Bill & Melinda Gates Foundation have provided funding and logistical support to enhance vaccine distribution in marginalized U.S. communities, ensuring that doses reach those most at risk.
One notable example of international collaboration is the partnership between the U.S. and Canada, where Canada donated excess vaccine doses to the U.S. during critical shortages in early 2021. This act of solidarity not only addressed immediate U.S. needs but also highlighted the interconnectedness of global health efforts. Similarly, the European Union’s temporary export waivers for vaccines produced within its borders allowed millions of doses to reach the U.S., accelerating its vaccination campaign. These examples underscore how international cooperation has been instrumental in supplementing U.S. vaccine funding and distribution.
NGOs have also been critical in addressing vaccine hesitancy and ensuring equitable access within the U.S. Organizations like the American Red Cross and the NAACP have partnered with federal and state governments to host vaccine clinics in underserved areas, particularly in communities of color. For instance, the NAACP’s partnership with Pfizer and BioNTech included targeted outreach campaigns and mobile clinics, resulting in over 500,000 vaccine doses administered in high-risk neighborhoods. Such efforts demonstrate how NGOs bridge gaps in federal and state programs, ensuring that no population is left behind.
Practical tips for leveraging international and NGO support include identifying local organizations with established community trust, such as faith-based groups or cultural associations, to facilitate vaccine distribution. For instance, partnering with the Hispanic Federation has proven effective in reaching Spanish-speaking populations, offering bilingual resources and culturally sensitive messaging. Additionally, tracking global vaccine surplus programs, like those managed by UNICEF, can provide opportunities for the U.S. to access additional doses during shortages. Finally, advocating for continued international collaboration through platforms like the World Health Organization ensures sustained support for global and domestic vaccine efforts.
In conclusion, while the U.S. government bears the primary financial responsibility for vaccines, international and NGO support has been indispensable in enhancing distribution, addressing inequities, and fostering global solidarity. These partnerships not only strengthen the U.S. response but also contribute to a more equitable global recovery. By recognizing and amplifying these efforts, the U.S. can build a more resilient public health infrastructure, both at home and abroad.
Vaccine-Associated Sarcomas: Which Species Faces the Highest Risk?
You may want to see also
Frequently asked questions
The federal government, through the Coronavirus Aid, Relief, and Economic Security (CARES) Act and other funding measures, has covered the cost of COVID-19 vaccines for all individuals in the U.S., regardless of insurance status.
No, COVID-19 vaccines are free for everyone in the U.S., including those without health insurance, as the cost is covered by the federal government.
No, healthcare providers and states are not responsible for paying for the vaccines. The federal government reimburses providers for administering the vaccines and covers the cost of the vaccine doses themselves.
While the federal government has covered the cost during the public health emergency, there is potential for COVID-19 vaccines to transition to the private market in the future. At that point, insurance companies may be billed, but individuals would still not incur out-of-pocket costs for the vaccine itself.