As the COVID-19 vaccination rollout continues, the focus has shifted to determining who will be included in the next group to receive the vaccine. This decision is typically based on a combination of factors, including age, underlying health conditions, occupation, and community transmission rates. Health authorities and governments work together to prioritize individuals who are at the highest risk of severe illness or death from the virus, as well as those who play critical roles in maintaining essential services. The goal is to allocate vaccines in a fair and efficient manner, ensuring that the most vulnerable populations are protected while also working towards achieving herd immunity. As more vaccine doses become available, the eligibility criteria are gradually expanded to include additional groups, with the ultimate aim of offering vaccination to the entire population.
Explore related products


$16.89 $16.95




What You'll Learn
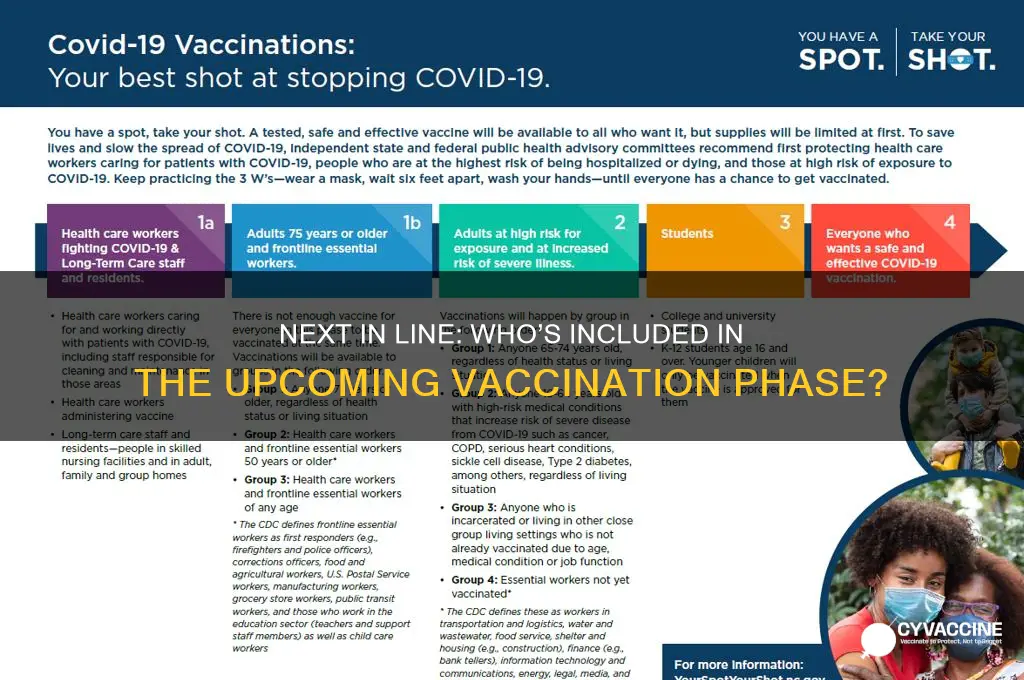
- Priority Groups: Essential workers, teachers, individuals with comorbidities, and those in high-risk environments
- Age-Based Rollout: Expanding eligibility to younger age groups as vaccine supply increases
- Geographic Distribution: Targeting areas with high transmission rates or limited healthcare access
- Occupation-Based Allocation: Including sectors like retail, transportation, and hospitality workers
- Community Outreach: Focusing on underserved populations and vaccine hesitancy hotspots
![]()
Priority Groups: Essential workers, teachers, individuals with comorbidities, and those in high-risk environments
Essential workers form the backbone of society, keeping critical services running during crises. From healthcare support staff to grocery store employees, their roles expose them to higher infection risks. Vaccinating this group minimizes disruptions to essential systems and protects those who cannot work remotely. For instance, a CDC study found that frontline workers accounted for 12% of COVID-19 cases in the U.S., despite comprising only 8% of the population. Prioritizing them ensures economic stability and public safety, with many countries allocating doses based on occupational risk assessments.
Teachers and school staff are another critical group, as their vaccination directly impacts educational continuity and student safety. A single unvaccinated teacher can lead to classroom closures, affecting dozens of students and their families. Evidence from the UK’s vaccination rollout shows that prioritizing educators reduced school outbreaks by 40%. Most guidelines recommend teachers receive the standard two-dose mRNA vaccine series, with boosters administered six months later. Schools can facilitate this by hosting on-site clinics during professional development days, streamlining access and encouraging uptake.
Individuals with comorbidities, such as diabetes, heart disease, or obesity, face significantly higher risks of severe illness. The WHO estimates that 68% of COVID-19 deaths globally occurred in those with pre-existing conditions. Vaccination protocols often prioritize this group based on age and condition severity, with some countries offering additional doses for immunocompromised individuals. For example, the FDA authorizes a third mRNA dose for those with moderate to severe immune deficiencies. Practical tips include scheduling vaccinations during stable health periods and consulting specialists to manage potential side effects.
High-risk environments, like prisons, homeless shelters, and meatpacking plants, are breeding grounds for outbreaks due to overcrowding and poor ventilation. In the U.S., prisons reported infection rates five times higher than the general population. Vaccinating these populations requires tailored strategies, such as mobile clinics and multilingual materials. Some facilities offer incentives, like reduced sentences or gift cards, to boost participation. A study in California found that vaccinating 80% of a prison population reduced case rates by 75%, demonstrating the impact of targeted interventions. Addressing these environments is crucial for equitable public health outcomes.
Best Vaccines for Pregnant Women in India: Expert Recommendations
You may want to see also
Explore related products






![]()
Age-Based Rollout: Expanding eligibility to younger age groups as vaccine supply increases
As vaccine supply ramps up, the logical next step in many immunization campaigns is to expand eligibility to younger age groups. This age-based rollout strategy prioritizes broader community protection by targeting populations previously deemed lower risk but now crucial for achieving herd immunity.
Consider a phased approach, starting with adolescents aged 12–15, followed by younger children as safety data becomes available. For instance, the Pfizer-BioNTech vaccine received emergency use authorization for 12–15-year-olds after trials demonstrated 100% efficacy in this group, with a two-dose regimen of 30 µg each, identical to adult dosing. This expansion not only protects younger individuals but also reduces transmission in schools and households.
However, implementation requires careful planning. Schools can serve as vaccination sites, but parental consent must be streamlined through digital forms or on-site authorization. Communication campaigns should address vaccine hesitancy among parents, emphasizing the vaccine’s safety profile and the role of younger populations in sustaining outbreaks.
A comparative analysis shows that countries like Canada and Israel, which prioritized age-based rollouts, saw faster declines in community transmission. By contrast, regions that delayed younger age group eligibility struggled with prolonged outbreaks. The takeaway is clear: as supply increases, age-based expansion is not just equitable but strategically essential for ending the pandemic.
Vaccinated vs. Unvaccinated: Who Fared Better?
You may want to see also
Explore related products






![]()
Geographic Distribution: Targeting areas with high transmission rates or limited healthcare access
In regions where COVID-19 transmission rates soar, vaccination strategies must pivot to prioritize geographic hotspots. Data from the CDC highlights that areas with dense populations, such as urban centers or crowded housing communities, often experience higher infection rates due to close contact. For instance, a neighborhood in Miami-Dade County saw a 25% positivity rate during a recent surge, compared to the national average of 10%. Targeting these zones with mobile vaccination units or pop-up clinics can rapidly curb spread, especially in groups like essential workers or those aged 16–40, who may face barriers to accessing fixed vaccination sites.
Limited healthcare access compounds the challenge in rural or underserved areas, where transmission can silently escalate. In Appalachia, for example, residents often travel over 50 miles to reach the nearest vaccination center, leading to lower uptake rates. Deploying single-dose vaccines like Johnson & Johnson in these regions offers a practical solution, as it eliminates the need for follow-up appointments. Pairing this with community health workers who provide door-to-door education and scheduling assistance can bridge the gap, ensuring even the most isolated populations receive protection.
A comparative analysis of urban and rural vaccination campaigns reveals the importance of tailored approaches. In New York City, mass vaccination sites effectively reached millions, but in rural Montana, smaller, localized efforts proved more successful. For instance, Montana’s partnership with local pharmacies and schools increased vaccination rates by 15% in just three months. This underscores the need to adapt strategies based on geographic realities, leveraging existing infrastructure and community trust to maximize impact.
Persuasively, targeting high-transmission areas isn’t just a public health strategy—it’s an economic imperative. Uncontrolled outbreaks in densely populated regions can disrupt supply chains, strain healthcare systems, and prolong lockdowns. By prioritizing these areas, policymakers can prevent broader societal and economic fallout. For example, vaccinating 70% of the population in a high-transmission county could reduce hospitalizations by up to 80%, freeing up resources for other critical needs. This approach not only saves lives but also accelerates recovery.
Practically, implementing a geographically focused vaccination plan requires coordination and flexibility. Start by mapping transmission hotspots using real-time data from health departments. Next, allocate resources like vaccines, personnel, and transportation to these areas, ensuring doses are stored and administered correctly (e.g., Pfizer requires ultra-cold storage, while Moderna offers more flexibility). Finally, engage local leaders to address hesitancy and ensure messaging resonates culturally. By combining data-driven targeting with community-centered execution, this strategy can effectively reach those most at risk, regardless of where they live.
Understanding Live Vaccines: How They Work and Why They Matter
You may want to see also
Explore related products






![]()
Occupation-Based Allocation: Including sectors like retail, transportation, and hospitality workers
Essential workers in sectors like retail, transportation, and hospitality form the backbone of daily life, yet their exposure to COVID-19 remains disproportionately high. Unlike remote workers, these individuals interact with dozens, if not hundreds, of people daily in enclosed spaces like stores, buses, and restaurants. This constant contact elevates their risk of infection, making them prime candidates for early vaccination. For instance, a CDC study found that frontline retail workers were five times more likely to test positive for COVID-19 compared to the general population. Prioritizing these workers not only protects them but also reduces community transmission, as they often serve as unwitting vectors due to their frequent public interactions.
Implementing occupation-based allocation requires a phased approach, balancing supply constraints with urgent need. Phase 1 could include high-contact roles like grocery store cashiers, bus drivers, and hotel staff, who often lack the luxury of social distancing. Phase 2 might expand to include warehouse workers, delivery personnel, and restaurant employees, whose roles are equally critical but may involve slightly less direct interaction. Employers can facilitate this process by providing on-site vaccination clinics during shifts, ensuring minimal disruption to operations. For example, Walmart and Uber partnered with local health departments to vaccinate employees at their workplaces, streamlining access and boosting participation rates.
Critics argue that occupation-based allocation could exacerbate inequities if not paired with geographic and demographic considerations. For instance, in low-income neighborhoods, where essential workers are often people of color, vaccine hesitancy and access barriers persist. To address this, allocation strategies must incorporate targeted outreach, such as multilingual information campaigns and mobile vaccination units. Additionally, offering incentives like paid time off for vaccination and recovery can encourage participation among workers who cannot afford unpaid leave. A pilot program in Chicago, which combined workplace clinics with community health worker outreach, saw a 30% increase in vaccination rates among essential workers in underserved areas.
The long-term benefits of prioritizing these sectors extend beyond public health. By safeguarding essential workers, societies can maintain economic stability and prevent supply chain disruptions. For example, a single outbreak among transportation workers could halt deliveries, causing ripple effects across industries. Moreover, protecting these workers fosters trust in public health initiatives, as it demonstrates a commitment to those who keep communities functioning. As vaccine supply increases, occupation-based allocation should remain a cornerstone of distribution strategies, ensuring that those who risk their health for others receive the protection they deserve.
Losing Your Mexican Vaccination Record: Consequences and Solutions Explained
You may want to see also
Explore related products






![]()
Community Outreach: Focusing on underserved populations and vaccine hesitancy hotspots
Underserved communities often face systemic barriers to healthcare, making them both high-risk and hard to reach during vaccination campaigns. These populations—rural residents, low-income families, racial and ethnic minorities, and those with limited English proficiency—are disproportionately affected by vaccine hesitancy, driven by historical mistrust, misinformation, and logistical challenges. For instance, a 2021 CDC study found that Black and Hispanic adults were less likely to receive COVID-19 vaccines due to concerns about side effects and mistrust of the medical system. Addressing these disparities requires tailored outreach strategies that acknowledge and dismantle these barriers.
Effective community outreach begins with understanding the unique needs and concerns of these populations. For example, in rural areas, transportation and internet access are significant hurdles. Mobile clinics offering walk-in appointments and on-site vaccination can bridge this gap. In urban hotspots, partnering with local churches, community centers, or trusted leaders can increase vaccine acceptance. A successful model is the *door-to-door* approach used in Brazil, where health workers visited homes to educate and vaccinate residents, achieving a 90% coverage rate in underserved neighborhoods. This method builds trust by meeting people where they are, both physically and culturally.
Language and cultural barriers further complicate outreach efforts. Translating materials into multiple languages is essential, but it’s not enough. Messages must be culturally relevant and delivered by trusted messengers. For instance, in Somali communities in Minnesota, local imams were enlisted to dispel myths about vaccines and encourage uptake. Similarly, in Hispanic communities, *promotoras* (community health workers) played a pivotal role in addressing fears and providing accurate information. These strategies highlight the importance of leveraging existing community structures to foster trust and engagement.
Vaccine hesitancy hotspots often stem from misinformation, which spreads rapidly in underserved areas with limited access to reliable sources. Combating this requires proactive, fact-based communication. Town hall meetings, social media campaigns, and local radio programs can be effective tools. For example, in India, WhatsApp groups were used to disseminate accurate vaccine information in regional languages, countering false narratives. Additionally, offering incentives like grocery vouchers or free health screenings can motivate hesitant individuals. However, these efforts must be paired with empathy and patience, acknowledging the valid reasons behind hesitancy without dismissing concerns.
Finally, sustainable outreach demands collaboration between governments, healthcare providers, and community organizations. Data-driven approaches, such as mapping hesitancy hotspots and tracking vaccination rates, can help allocate resources efficiently. For instance, in the U.S., the HRSA’s *Vaccine Equity Initiative* provided funding to community health centers to target underserved populations, resulting in millions of vaccinations in high-risk areas. By combining grassroots efforts with systemic support, we can ensure that no community is left behind in the next phase of vaccination campaigns.
Vaccination Requirements for Public School Attendance Explained
You may want to see also
Frequently asked questions
The next group typically includes essential workers, such as teachers, grocery store employees, and public transit workers, followed by individuals with underlying health conditions that increase their risk of severe illness.
The next group is determined based on factors like risk of exposure, risk of severe illness, and the goal of reducing community spread, with guidelines often provided by health authorities like the CDC or WHO.
Eligibility for the next group depends on vaccine supply and distribution plans, with timelines varying by region. Local health departments or government websites typically announce specific dates.