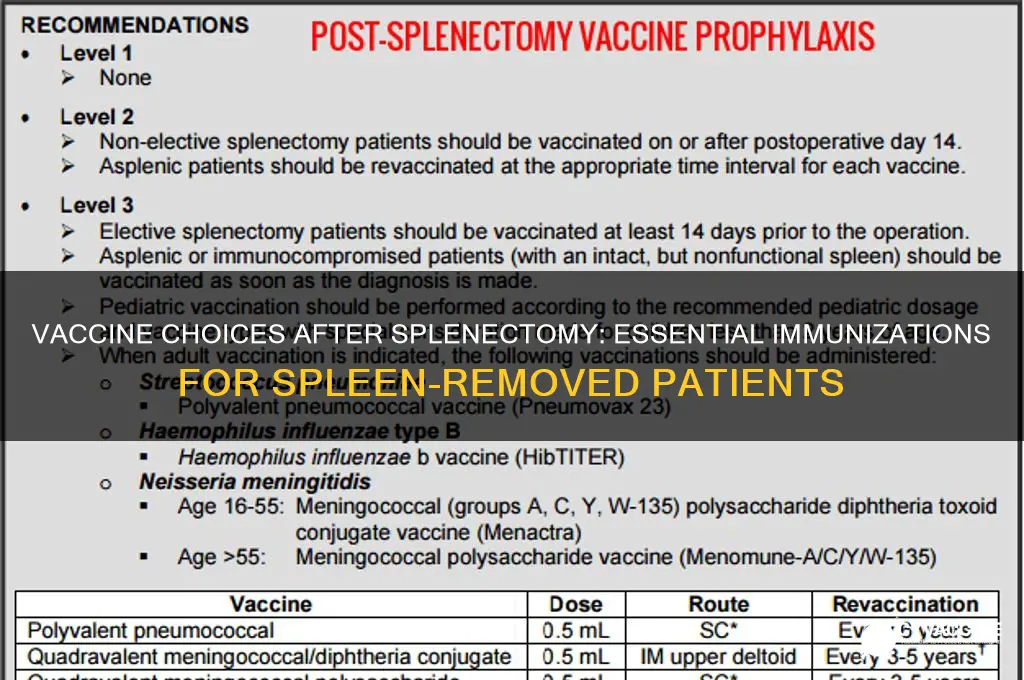
Patients who have had their spleen removed (splenectomy) are at increased risk for severe infections, particularly from encapsulated bacteria such as *Streptococcus pneumoniae*, *Haemophilus influenzae type b* (Hib), and *Neisseria meningitidis*. To protect against these infections, specific vaccinations are recommended. These typically include the pneumococcal conjugate vaccine (PCV13 or PCV15), followed by the pneumococcal polysaccharide vaccine (PPSV23), as well as the Hib and meningococcal vaccines. It is crucial for healthcare providers to ensure these vaccines are administered according to the latest guidelines, as they significantly reduce the risk of life-threatening infections in asplenic individuals. Consultation with an infectious disease specialist or immunologist may be beneficial to tailor the vaccination schedule to the patient’s specific needs.
| Characteristics | Values |
|---|---|
| Condition | Asplenia (absence of spleen function, either surgically removed or non-functional) |
| Increased Risk | Susceptibility to encapsulated bacterial infections (e.g., Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis) |
| Recommended Vaccines |
|
| Vaccination Schedule |
|
| Booster Doses |
|
| Additional Precautions |
|
| Guidelines Source | Centers for Disease Control and Prevention (CDC), World Health Organization (WHO), and local health authorities |
| Last Updated | As of 2023 (guidelines may vary by region; consult healthcare provider for latest recommendations) |
Explore related products






What You'll Learn
- Pneumococcal Vaccines: Essential for post-splenectomy patients to prevent serious infections like pneumonia and meningitis
- Meningococcal Vaccines: Protects against meningococcal disease, a life-threatening bacterial infection in asplenic individuals
- Haemophilus Influenzae Type B (Hib): Reduces risk of severe infections, including sepsis and meningitis
- Annual Flu Vaccine: Boosts immunity against influenza, which can lead to severe complications without a spleen
- COVID-19 Vaccine: Important for overall protection, as asplenic patients are at higher risk for severe illness
![]()
Pneumococcal Vaccines: Essential for post-splenectomy patients to prevent serious infections like pneumonia and meningitis
The spleen plays a critical role in filtering blood and fighting infections, particularly those caused by encapsulated bacteria like *Streptococcus pneumoniae*. When the spleen is removed—a procedure known as splenectomy—patients become significantly more susceptible to severe infections, including pneumonia, meningitis, and sepsis. Pneumococcal vaccines are not just recommended but essential for these individuals to mitigate this heightened risk. Without a functioning spleen, the body loses a key defense mechanism, making vaccination a vital preventive measure.
Pneumococcal vaccines come in two primary forms: pneumococcal conjugate vaccine (PCV13 or Prevnar 13) and pneumococcal polysaccharide vaccine (PPSV23 or Pneumovax 23). For post-splenectomy patients, both vaccines are typically administered in a sequential regimen. The CDC recommends starting with PCV13, followed by PPSV23 at least 8 weeks later. This combination provides broader protection against pneumococcal serotypes, covering both invasive diseases and pneumonia. For adults aged 19 and older who have undergone splenectomy, this two-dose series is standard, with a potential booster dose of PPSV23 after 5 years, depending on individual risk factors.
The timing of vaccination is crucial. Ideally, patients should receive their first dose of PCV13 at least 2 weeks before splenectomy, if possible. If vaccination occurs after surgery, it should be administered as soon as feasible, ideally within the first year post-splenectomy. Delayed vaccination still offers significant protection but may leave patients vulnerable during the interim period. Practical tips include scheduling vaccine appointments promptly after surgery, keeping a record of vaccination dates, and ensuring healthcare providers are aware of the patient’s splenectomy status to avoid missed opportunities for immunization.
While pneumococcal vaccines are highly effective, they are not 100% protective. Post-splenectomy patients must also adopt additional precautions, such as carrying a medical alert card, wearing a medical ID bracelet, and promptly seeking medical attention for fever or signs of infection. Antibiotic prophylaxis may be prescribed in some cases, but vaccination remains the cornerstone of prevention. By combining vaccination with these measures, patients can significantly reduce their risk of life-threatening infections and maintain a healthier, more secure lifestyle after splenectomy.
Understanding the National Vaccine Injury Compensation Act: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Meningococcal Vaccines: Protects against meningococcal disease, a life-threatening bacterial infection in asplenic individuals
The spleen plays a critical role in filtering blood and fighting infections, particularly those caused by encapsulated bacteria. When the spleen is removed—a condition known as asplenia—individuals become significantly more vulnerable to severe infections, including meningococcal disease. This life-threatening bacterial infection, caused by *Neisseria meningitidis*, can lead to meningitis or sepsis, with mortality rates as high as 10–15% even with prompt treatment. For asplenic patients, the risk of contracting meningococcal disease increases 300-fold compared to the general population, making vaccination not just advisable but essential.
Meningococcal vaccines are specifically designed to protect against the most common serogroups of *N. meningitidis*—A, B, C, W, and Y. For asplenic individuals, the Centers for Disease Control and Prevention (CDC) recommends a comprehensive vaccination strategy. This includes the meningococcal conjugate vaccine (MenACWY), which covers serogroups A, C, W, and Y, and the serogroup B meningococcal vaccine (MenB). MenACWY is typically administered as a two-dose series for asplenic patients, with the first dose given as soon as possible after splenectomy and the second dose 2 months later. Booster doses of MenACWY are recommended every 5 years to maintain immunity. For MenB, a two-dose series (e.g., Bexsero or Trumenba) is advised, with doses spaced 1–2 months apart, depending on the specific vaccine.
Age is a critical factor in determining the vaccination schedule. Children aged 2–10 years who are asplenic should receive a primary series of MenACWY, followed by boosters every 3 years. Adolescents and adults follow the standard 5-year booster schedule. For MenB, the vaccine is approved for individuals aged 10 years and older, with no current recommendation for routine boosters. It’s important to note that these vaccines are not interchangeable; both MenACWY and MenB are necessary to provide broad protection against meningococcal disease.
Practical tips for asplenic patients include carrying a medical alert card or wearing a bracelet indicating their condition, as this can expedite appropriate treatment in emergencies. Additionally, patients should be educated about the signs and symptoms of meningococcal disease, such as sudden fever, severe headache, neck stiffness, and a rash, and instructed to seek immediate medical attention if these occur. Antibiotic prophylaxis may also be prescribed by healthcare providers, but vaccination remains the cornerstone of prevention.
In summary, meningococcal vaccines are a critical intervention for asplenic individuals, offering protection against a disease that poses a disproportionately high risk to this population. By adhering to the recommended vaccination schedules and staying informed about potential risks, patients and healthcare providers can work together to mitigate the dangers of meningococcal disease in the absence of a functioning spleen.
The End of Live Polio Vaccines: A Historical Shift
You may want to see also
Explore related products






![]()
Haemophilus Influenzae Type B (Hib): Reduces risk of severe infections, including sepsis and meningitis
The removal of the spleen, a procedure known as splenectomy, significantly increases a patient's susceptibility to severe bacterial infections. This is because the spleen plays a crucial role in filtering blood and identifying encapsulated bacteria, such as *Haemophilus influenzae type b* (Hib). Without a functioning spleen, these bacteria can proliferate unchecked, leading to life-threatening conditions like sepsis and meningitis. Vaccination against Hib becomes a critical preventive measure for these patients.
From an analytical perspective, the Hib vaccine is particularly vital for asplenic individuals due to the bacterium's capsule, which allows it to evade the immune system. The vaccine works by inducing antibodies against this polysaccharide capsule, effectively neutralizing the bacteria before they can cause infection. Studies show that Hib vaccination reduces the risk of invasive Hib disease by over 95% in immunocompetent individuals, and while data specific to asplenic patients is limited, the protective effect is expected to be similarly substantial. This makes the Hib vaccine a cornerstone in post-splenectomy immunization protocols.
Instructively, the Hib vaccine is typically administered as part of a combination vaccine, such as DTaP-Hib-IPV (diphtheria, tetanus, pertussis, Hib, and polio) for children, or as a standalone dose for adults. For asplenic patients, the CDC recommends a single dose of Hib vaccine if they have not been previously vaccinated. If the patient has received Hib vaccination before splenectomy, a booster dose is advised. It’s important to note that the vaccine is generally well-tolerated, with mild side effects like soreness at the injection site being the most common.
Persuasively, the consequences of skipping the Hib vaccine for asplenic patients cannot be overstated. Without this protection, the risk of invasive Hib disease increases 50- to 200-fold compared to the general population. Sepsis and meningitis, both potential complications, carry high mortality rates and long-term disabilities, especially in adults. Given the vaccine’s proven efficacy and safety profile, it is a small but critical step in safeguarding the health of splenectomized individuals.
Comparatively, while other vaccines like pneumococcal and meningococcal are also essential for asplenic patients, the Hib vaccine stands out due to its specificity in targeting a bacterium that is particularly adept at exploiting the absence of splenic function. Unlike pneumococcal vaccines, which cover multiple serotypes, the Hib vaccine is monovalent, simplifying its administration and ensuring robust immunity against a single, high-risk pathogen. This focused approach makes it an indispensable component of post-splenectomy care.
Practically, healthcare providers should ensure that asplenic patients receive the Hib vaccine as soon as possible after splenectomy, ideally within two weeks, to minimize the window of vulnerability. Patients should also be educated about the importance of carrying a wallet card or medical alert indicating their asplenic status, as this can prompt timely antibiotic treatment in case of infection. Additionally, maintaining up-to-date vaccination records and scheduling regular check-ups can help monitor immunity and address any gaps in protection. By prioritizing Hib vaccination, clinicians can significantly reduce the risk of severe infections in this vulnerable population.
Post-Vaccination Baby Bathing: Safe Practices and Timing for Parents
You may want to see also
Explore related products






![]()
Annual Flu Vaccine: Boosts immunity against influenza, which can lead to severe complications without a spleen
Individuals who have had their spleen removed, a procedure known as splenectomy, face heightened risks from certain infections, including influenza. The spleen plays a critical role in filtering blood and fighting pathogens, so its absence weakens the immune system’s ability to respond to encapsulated bacteria and viruses like the flu. Annual flu vaccination becomes a cornerstone of preventive care for these patients, significantly reducing their risk of severe complications such as pneumonia, sepsis, or hospitalization. Without this protection, influenza can progress rapidly and unpredictably in asplenic individuals, making vaccination not just advisable but essential.
The annual flu vaccine is specifically designed to target the most prevalent influenza strains each season, providing tailored immunity. For patients without a spleen, this vaccine acts as a critical shield, compensating for their reduced ability to combat infections. It’s important to note that the flu vaccine does not guarantee complete immunity but substantially lowers the likelihood of infection and severe outcomes. Adults and children over six months old who have undergone splenectomy should receive the inactivated influenza vaccine (IIV), as live attenuated vaccines (like the nasal spray) are contraindicated due to their immunocompromised state. Timing is key—aim to get vaccinated by the end of October, as flu activity typically peaks between December and February.
Comparatively, the flu vaccine stands out as one of the most accessible and effective measures for asplenic patients, especially when paired with other precautions like pneumococcal and meningococcal vaccinations. Unlike antibiotics or antiviral medications, which are reactive treatments, the flu vaccine is proactive, priming the immune system to recognize and neutralize the virus before it causes harm. However, it’s not a one-size-fits-all solution. Patients should consult their healthcare provider to ensure the vaccine aligns with their medical history and current health status. For instance, those with egg allergies can safely receive most flu vaccines, but severe allergic reactions require specialized formulations.
Practical tips can enhance the effectiveness of the flu vaccine for asplenic individuals. First, stay informed about local flu activity through resources like the CDC or WHO to gauge when vaccination is most urgent. Second, maintain a healthy lifestyle—adequate sleep, hydration, and nutrition—to support overall immune function. Third, carry a medical alert card or wear a bracelet indicating your asplenic status, as this ensures prompt treatment if flu-like symptoms arise. Finally, keep a record of your vaccination dates and share them with all healthcare providers to ensure continuity of care. By integrating the annual flu vaccine into a broader health strategy, asplenic patients can significantly mitigate the risks associated with influenza.
Understanding Religious Exemption Criteria for Vaccination Requirements
You may want to see also
Explore related products






![]()
COVID-19 Vaccine: Important for overall protection, as asplenic patients are at higher risk for severe illness
Individuals who have had their spleen removed, a condition known as asplenia, face a heightened vulnerability to infections due to the spleen’s critical role in filtering blood and fighting pathogens. This immunocompromised state significantly increases the risk of severe illness from COVID-19, making vaccination not just advisable but essential. The COVID-19 vaccine acts as a vital shield, bolstering the immune system’s ability to recognize and combat the virus, thereby reducing the likelihood of hospitalization or death in asplenic patients.
Analyzing the vaccine options, mRNA vaccines (Pfizer-BioNTech and Moderna) are generally recommended for asplenic individuals due to their high efficacy and robust immune response. These vaccines have been shown to produce strong neutralizing antibodies, which are crucial for preventing severe COVID-19 outcomes. For asplenic patients, the standard dosing schedule applies: two primary doses followed by a booster, with an additional booster recommended for those over 50 or with severe immunocompromise. It’s important to note that the timing of boosters may vary based on individual health status, so consulting a healthcare provider is essential.
A comparative look at other vaccine types reveals that while viral vector vaccines (Johnson & Johnson) are effective, they may elicit a slightly weaker immune response in immunocompromised individuals. However, they remain a viable option if mRNA vaccines are unavailable or contraindicated. Novavax, a protein subunit vaccine, is another alternative, particularly for those with mRNA vaccine hesitancy or allergies. Regardless of the vaccine chosen, the goal is to achieve the highest possible level of protection, as asplenic patients are less likely to mount a full immune response compared to the general population.
Practical tips for asplenic patients include scheduling vaccinations during periods of good health to maximize immune response and ensuring all recommended doses are completed. Additionally, these individuals should continue adhering to preventive measures like masking and social distancing, especially in high-risk settings. Regular communication with a healthcare provider is crucial to tailor the vaccination strategy to individual needs, including potential adjustments for comorbidities or other immunizations like pneumococcal or meningococcal vaccines, which are also critical for asplenic patients.
In conclusion, the COVID-19 vaccine is a cornerstone of protection for asplenic patients, who are at heightened risk for severe illness. By prioritizing mRNA vaccines, adhering to dosing schedules, and maintaining open dialogue with healthcare providers, these individuals can significantly reduce their vulnerability to COVID-19. This proactive approach not only safeguards personal health but also contributes to broader community immunity, underscoring the vaccine’s importance in this unique population.
Understanding Medical Exemptions: How Many Skip Vaccines for Health Reasons?
You may want to see also
Frequently asked questions
Patients who have had their spleen removed (splenectomy) should receive the pneumococcal conjugate vaccine (PCV13), followed by the pneumococcal polysaccharide vaccine (PPSV23), to protect against Streptococcus pneumoniae infections.
Yes, in addition to pneumococcal vaccines, patients without a spleen should receive the meningococcal conjugate vaccine (MenACWY) and the Haemophilus influenzae type b (Hib) vaccine to prevent serious bacterial infections.
After the initial series, a booster dose of PPSV23 is recommended 5 years after the first dose. However, specific timing may vary, so consult a healthcare provider for personalized advice.
Yes, annual influenza vaccination is strongly recommended for splenectomy patients, as they are at higher risk of complications from the flu, which can increase susceptibility to secondary bacterial infections.
Yes, the COVID-19 vaccine is recommended for splenectomy patients, as they are at increased risk of severe illness from COVID-19. They should follow the standard vaccination schedule, including boosters as advised.