The emergence of the Indian variant, also known as Delta, has raised concerns about vaccine efficacy and the best protection against this highly transmissible strain. As countries grapple with its rapid spread, understanding which vaccine offers the most robust defense is crucial. Studies indicate that while no vaccine provides complete immunity, those like Pfizer-BioNTech and Moderna, based on mRNA technology, have shown higher effectiveness in preventing symptomatic infection and severe outcomes compared to viral vector vaccines like AstraZeneca and Covaxin. However, the availability and distribution of these vaccines vary globally, making it essential to consider local contexts and public health strategies in determining the best vaccine for combating the Indian variant.
Explore related products

$3.59 $24.95





What You'll Learn
![]()
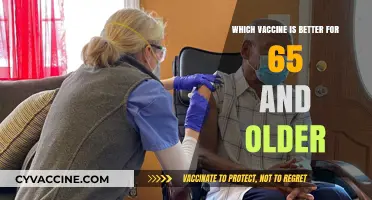
Vaccine Efficacy Against Indian Variant
The Indian variant, now known as the Delta variant, has raised concerns about vaccine efficacy, prompting a closer examination of how different vaccines perform against this highly transmissible strain. Data from various studies and real-world scenarios provide insights into which vaccines offer the strongest protection. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines have demonstrated high efficacy against the Delta variant, with studies showing around 88% effectiveness after two doses in preventing symptomatic infection. This is slightly lower than their efficacy against the original strain but still robust, particularly in preventing severe illness and hospitalization.
In contrast, the AstraZeneca vaccine, widely used in India and other countries, has shown slightly lower efficacy against the Delta variant, with effectiveness ranging from 60% to 67% after two doses. However, it remains highly effective in preventing severe disease and hospitalization, which is a critical measure of vaccine success. A key takeaway is that while no vaccine provides 100% protection, completing the full dosage regimen significantly enhances immunity. For AstraZeneca, ensuring a 12-week gap between doses has been shown to improve efficacy, particularly against variants.
Another important consideration is the role of booster doses in maintaining protection. Emerging data suggest that a third dose of mRNA vaccines can restore efficacy to over 90% against the Delta variant, even among older adults or those with comorbidities. This underscores the importance of booster strategies, especially in regions with high Delta variant circulation. For individuals who received vaccines like Sinovac or Sinopharm, which have lower efficacy against Delta, heterologous boosting (using a different vaccine type for the booster) has shown promising results in enhancing immunity.
Practical tips for maximizing vaccine efficacy include adhering strictly to dosing schedules, avoiding misinformation about vaccine safety, and continuing to follow public health measures like masking and social distancing, especially in crowded settings. Additionally, individuals should stay informed about local vaccination campaigns and booster availability. For those in regions with limited access to mRNA vaccines, prioritizing full vaccination with available options remains crucial, as even partial protection is better than none.
In conclusion, while the Delta variant poses challenges, vaccines remain a powerful tool in the fight against COVID-19. The choice of vaccine may depend on availability and individual health considerations, but the overarching message is clear: getting vaccinated and staying up-to-date with recommended doses is the most effective way to protect against severe illness and contribute to community immunity.
Planet Fitness Membership: Vaccinated or Not?
You may want to see also
Explore related products






![]()
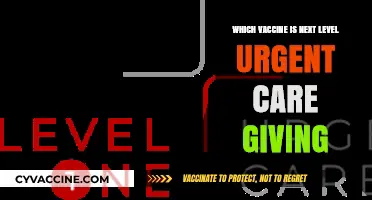
Pfizer vs. AstraZeneca Comparison
The Indian variant, now known as Delta, has raised critical questions about vaccine efficacy. Among the frontrunners, Pfizer and AstraZeneca dominate discussions, but their differences in technology, dosage, and real-world performance demand scrutiny. Pfizer’s mRNA platform delivers genetic instructions via lipid nanoparticles, requiring ultra-cold storage and a two-dose regimen (30 µg each, 21 days apart). AstraZeneca, a viral vector vaccine, uses a modified adenovirus to transport spike protein DNA, stored in standard refrigeration and administered in two doses (0.5 mL each, 4–12 weeks apart). These foundational distinctions set the stage for their comparative analysis against Delta.
Efficacy Against Delta: The Numbers Speak
Studies reveal Pfizer’s slight edge in neutralizing Delta. A Public Health England analysis showed Pfizer’s efficacy at 88% against symptomatic disease after two doses, compared to AstraZeneca’s 67%. However, both vaccines demonstrated over 90% effectiveness in preventing hospitalization, underscoring their shared strength in averting severe outcomes. Notably, Pfizer’s efficacy post-first dose is lower (36%), while AstraZeneca’s is 30%, emphasizing the critical need for completing both doses. For those in high-transmission areas, Pfizer’s faster immune ramp-up (21-day interval) may offer earlier protection, whereas AstraZeneca’s flexibility in dosing intervals caters to logistical challenges in resource-constrained settings.
Practical Considerations: Age, Access, and Side Effects
Pfizer is authorized for individuals aged 12 and above, making it a family-friendly option, while AstraZeneca is typically recommended for adults over 18 (or 30–40 in some countries due to rare blood clot risks). Side effects differ: Pfizer recipients often report fatigue, fever, and injection-site pain after the second dose, whereas AstraZeneca is linked to flu-like symptoms and, rarely, thrombosis with thrombocytopenia syndrome (TTS). For younger populations or those with clotting concerns, Pfizer may be preferable, but AstraZeneca’s accessibility in low-income regions makes it a cornerstone of global equity efforts.
Boosters and Variants: A Dynamic Landscape
The Delta variant’s mutations spotlight the need for boosters. Pfizer’s third-dose trials show a 5-fold increase in antibodies, and some countries now recommend boosters for vulnerable groups. AstraZeneca’s booster data is less conclusive, though heterologous boosting (mixing with mRNA vaccines) has shown promise in enhancing immunity. For travelers or those in outbreak zones, Pfizer’s higher initial efficacy might tip the scale, but AstraZeneca’s durability remains competitive, particularly in preventing severe disease.
Takeaway: Context Dictates Choice
The "best" vaccine hinges on context. Pfizer excels in rapid, high-efficacy protection, ideal for urban populations or younger demographics. AstraZeneca’s logistical simplicity and cost-effectiveness make it indispensable for mass immunization campaigns. Ultimately, the best vaccine is the one available—both significantly reduce Delta’s impact, and hesitancy poses a greater risk than minor efficacy differences. Consult local health guidelines, prioritize timely vaccination, and remember: any vaccine is a step toward collective immunity.
Maryland's Mass Vaccination Sites: Locations and Essential Information
You may want to see also
Explore related products






![]()
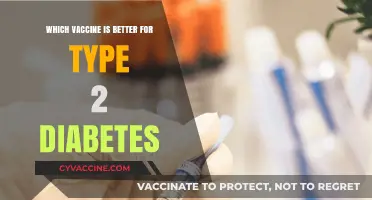
Covaxin’s Role in Variant Protection
As the Indian variant (B.1.617) emerged, global attention turned to vaccine efficacy against this strain. Among the vaccines developed and deployed in India, Covaxin, produced by Bharat Biotech in collaboration with the Indian Council of Medical Research (ICMR) and the National Institute of Virology (NIV), has been a focal point. Covaxin’s unique inactivated virus technology positions it as a strong candidate for variant protection, but its role extends beyond its mechanism. Early studies indicate that Covaxin elicits a broad immune response, including neutralizing antibodies and T-cell immunity, which may offer resilience against mutations in the Indian variant. This dual-action immunity is critical, as variants often evade antibody-based defenses but remain susceptible to T-cell attacks.
To understand Covaxin’s role, consider its dosage and administration. The vaccine is administered in two doses, 4–6 weeks apart, with a full immune response typically achieved 2 weeks after the second dose. For adults aged 18 and above, this regimen has shown efficacy against symptomatic COVID-19, including cases caused by the Indian variant. Practical tips for recipients include scheduling the second dose promptly to ensure optimal immunity and monitoring for mild side effects like fever or injection site pain, which are normal indicators of immune activation.
Comparatively, Covaxin’s inactivated virus platform differs from mRNA vaccines like Pfizer or Moderna, which target the spike protein specifically. While mRNA vaccines have shown reduced neutralizing antibody activity against some variants, Covaxin’s whole-virus approach exposes the immune system to multiple viral components, potentially offering broader protection. A study published in *The Lancet* highlighted that Covaxin recipients developed antibodies capable of neutralizing the B.1.617 variant, though at slightly lower levels than against the original strain. This suggests partial but meaningful protection, especially against severe disease and hospitalization.
Persuasively, Covaxin’s role in variant protection is further strengthened by its accessibility and storage advantages. Unlike mRNA vaccines requiring ultra-cold storage, Covaxin can be stored at 2–8°C, making it more feasible for distribution in resource-limited settings. This logistical edge ensures wider coverage, a critical factor in combating variants that thrive in under-vaccinated populations. For policymakers and healthcare providers, prioritizing Covaxin in regions with high variant prevalence could mitigate outbreak severity and reduce the emergence of new mutations.
In conclusion, Covaxin’s inactivated virus technology, combined with its ability to induce both antibody and T-cell responses, positions it as a valuable tool against the Indian variant. While no vaccine offers complete protection against all variants, Covaxin’s broad immune activation and practical advantages make it a strategic choice in the fight against evolving strains. Recipients should adhere to the recommended dosage schedule and remain vigilant about emerging data, as ongoing research will further refine our understanding of its efficacy in real-world scenarios.
Understanding mRNA Vaccine Half-Life: Duration, Immunity, and Efficacy Explained
You may want to see also
Explore related products






![]()
Booster Shots for Enhanced Immunity
The Indian variant, now known as the Delta variant, has raised concerns about vaccine efficacy and the need for enhanced immunity. As this variant continues to spread globally, the role of booster shots in maintaining robust protection has become a critical discussion point. Booster shots, essentially additional doses of a vaccine, are designed to remind the immune system of a previous infection or vaccination, thereby strengthening its response to the virus. This is particularly relevant for the Delta variant, which has shown a higher transmissibility rate and potential immune evasion capabilities.
From an analytical perspective, the effectiveness of booster shots lies in their ability to increase neutralizing antibodies and memory cells. Studies have shown that a third dose of mRNA vaccines, such as Pfizer-BioNTech or Moderna, can significantly boost antibody levels, particularly in individuals aged 65 and older or those with compromised immune systems. For instance, a Pfizer booster shot administered 6 months after the second dose has been found to increase antibody titers by 5 to 10 times, offering enhanced protection against symptomatic infection, including the Delta variant. This data underscores the importance of timing and dosage in maximizing the benefits of booster shots.
Instructively, the administration of booster shots varies by vaccine type and population. For mRNA vaccines, the recommended interval between the second dose and the booster is typically 6 months, while for viral vector vaccines like AstraZeneca, the interval may be shorter, around 3 months, depending on local health guidelines. It’s crucial for individuals to consult healthcare providers to determine eligibility, especially for those with underlying health conditions or weakened immune systems. Practical tips include scheduling the booster during a time when one can rest afterward, staying hydrated, and monitoring for common side effects like fatigue or mild fever, which generally subside within 48 hours.
Persuasively, the case for booster shots extends beyond individual protection to community immunity. As the Delta variant continues to circulate, achieving high vaccination rates, including boosters, is essential to reduce transmission and prevent the emergence of new variants. Countries like Israel, which implemented a widespread booster campaign, have reported a significant decline in severe cases and hospitalizations, even amid Delta surges. This example highlights the dual benefit of boosters: safeguarding personal health while contributing to the broader public health effort.
Comparatively, while booster shots are effective, they are not a standalone solution. Combining them with non-pharmaceutical interventions, such as mask-wearing and social distancing, remains crucial, especially in regions with low vaccination coverage. Additionally, the development of variant-specific vaccines is underway, offering another layer of defense. However, until these become available, boosters serve as a practical and immediate measure to enhance immunity against the Delta variant and other strains. By understanding their role and following recommended guidelines, individuals can take proactive steps to protect themselves and their communities.
Applying for Religious Exemption: A Guide to Vaccine Exemptions
You may want to see also
Explore related products






![]()
Global Vaccine Accessibility Challenges
The emergence of the Indian variant, now known as Delta, has underscored the urgent need for effective vaccines. However, the global vaccine rollout has been marred by accessibility challenges, exacerbating disparities between wealthy and low-income nations. While vaccines like Pfizer-BioNTech and Moderna have shown high efficacy against Delta, their distribution remains concentrated in affluent countries. For instance, as of late 2021, over 70% of vaccine doses had been administered in just 10 countries, leaving many low-income nations with less than 1% of their populations vaccinated. This inequity not only prolongs the pandemic but also allows variants to emerge and spread unchecked.
One critical challenge is the logistical complexity of distributing vaccines, particularly those requiring ultra-cold storage, such as Pfizer’s mRNA vaccine, which must be stored at -70°C. This poses significant hurdles for countries with limited infrastructure, where reliable electricity and refrigeration systems are scarce. In contrast, vaccines like AstraZeneca and Johnson & Johnson, which are stable at standard refrigerator temperatures (2–8°C), are more feasible for widespread distribution. However, supply shortages and export restrictions, particularly from manufacturing hubs like India, have further hindered access to these alternatives.
Another barrier is the cost and intellectual property rights associated with vaccines. Wealthy nations have secured billions of doses through advance purchase agreements, leaving little for the global South. The COVAX initiative, aimed at equitable distribution, has fallen short of its targets due to funding gaps and vaccine hoarding. For example, while the U.S. and EU have vaccinated over 60% of their populations, many African countries have vaccinated less than 5%. This disparity highlights the need for patent waivers and technology transfers to enable local production, a proposal supported by over 100 countries but opposed by pharmaceutical giants and some high-income nations.
Practical steps to address these challenges include prioritizing dose-sharing mechanisms, where countries with surplus vaccines donate to those in need. For instance, the U.S. has pledged to share 1.1 billion doses globally, but only a fraction has been delivered. Additionally, investing in local manufacturing capacity in low-income regions can reduce dependency on imports. Countries like India and South Africa have already begun producing vaccines domestically, but scaling up requires financial and technical support from the international community.
In conclusion, while vaccines like Pfizer and Moderna are highly effective against the Delta variant, their inaccessibility in many parts of the world perpetuates the pandemic. Addressing global vaccine inequity demands a multifaceted approach: simplifying distribution logistics, reducing costs, and fostering international cooperation. Without urgent action, the divide between vaccinated and unvaccinated nations will widen, leaving the world vulnerable to new variants and prolonged health and economic crises.
Kitten Vaccine Storage: Fridge or Freezer?
You may want to see also
Frequently asked questions
Studies show that both Pfizer-BioNTech and Moderna (mRNA vaccines) offer high protection against the Delta variant, with around 88% effectiveness after two doses. AstraZeneca (Covishield in India) is also effective, providing around 60-67% protection after two doses.
Yes, Covaxin has demonstrated effectiveness against the Delta variant. Clinical trial data and real-world studies indicate that it provides robust protection, especially against severe disease and hospitalization.
Mixing vaccines (e.g., taking one dose of Covishield and one dose of Covaxin) has shown promising results in some studies, potentially enhancing immune response. However, it’s best to follow local health guidelines for vaccine schedules.
No, one dose provides limited protection against the Delta variant. Full vaccination (two doses) is essential for optimal immunity, especially against severe illness and hospitalization.
Booster shots can enhance immunity and provide additional protection, especially for vulnerable populations. However, the need for a booster depends on factors like time since vaccination and individual health status. Consult healthcare authorities for recommendations.