Vaccines are designed to stimulate the immune system to recognize and combat pathogens without causing the disease itself. To achieve this, vaccines typically contain a specific piece of the pathogen, such as a protein, sugar, or genetic material, that is crucial for the pathogen's function or structure. This component, known as an antigen, triggers an immune response, allowing the body to produce antibodies and memory cells that can quickly respond to future infections. Depending on the type of vaccine, the antigen may be a whole inactivated or attenuated pathogen, a subunit of the pathogen, a toxin produced by the pathogen, or even a piece of the pathogen's genetic code, such as mRNA or viral DNA. Understanding which piece of the pathogen is included in a vaccine is essential for comprehending how it confers immunity and ensures safety and efficacy.
Explore related products






What You'll Learn
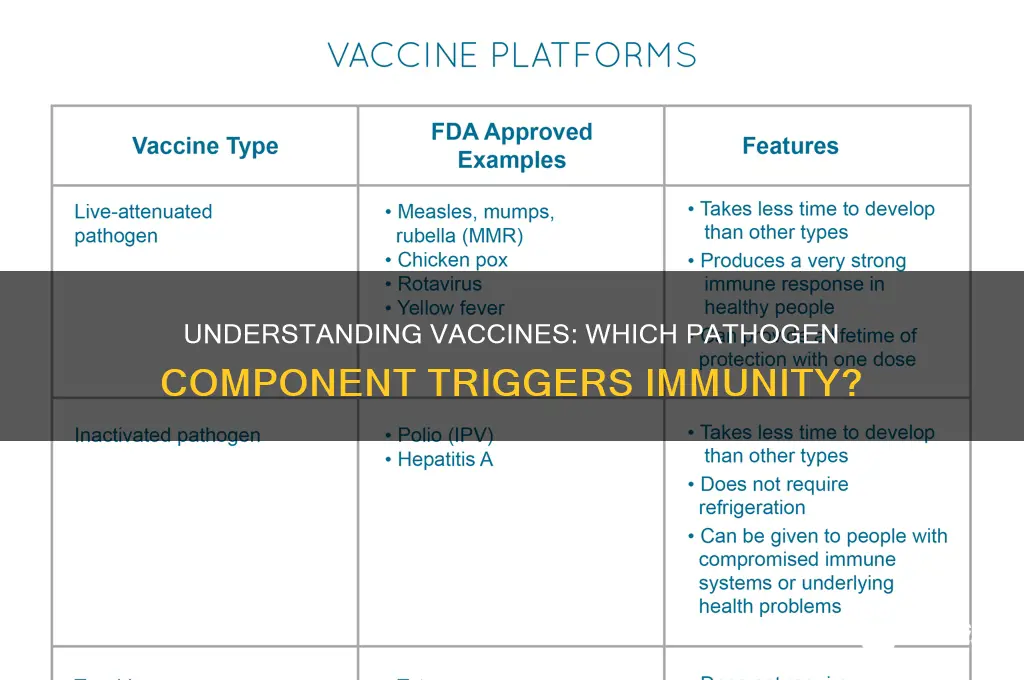
- Whole Pathogen Vaccines: Uses entire pathogens, either inactivated or attenuated, to trigger immune response
- Subunit Vaccines: Contains specific pathogen proteins or fragments to stimulate immunity safely
- Toxoid Vaccines: Includes inactivated toxins produced by pathogens to neutralize harmful effects
- Nucleic Acid Vaccines: Delivers genetic material (DNA/RNA) coding for pathogen antigens to produce immunity
- Viral Vector Vaccines: Uses modified viruses to deliver pathogen genes for immune response
![]()
Whole Pathogen Vaccines: Uses entire pathogens, either inactivated or attenuated, to trigger immune response
Whole pathogen vaccines represent a cornerstone of immunization, leveraging the entire pathogen—either inactivated or attenuated—to provoke a robust immune response. Unlike subunit or mRNA vaccines that target specific components, these vaccines expose the immune system to the full array of pathogen antigens, often leading to broader immunity. For instance, the inactivated polio vaccine (IPV) uses chemically inactivated poliovirus, while the measles, mumps, and rubella (MMR) vaccine employs live attenuated viruses. This approach mimics natural infection without causing disease, training the immune system to recognize and combat the pathogen effectively.
Inactivated vaccines, such as the whole-cell pertussis vaccine, are created by killing the pathogen with heat, chemicals, or radiation. This process preserves the pathogen’s structural integrity, allowing the immune system to identify multiple antigens. However, inactivated vaccines often require higher doses or adjuvants to enhance immunity, as the pathogen’s ability to replicate is eliminated. For example, the hepatitis A vaccine uses inactivated virus particles, typically administered in two doses spaced 6–12 months apart for individuals aged 1 year and older. While safe, inactivated vaccines may elicit milder immune responses compared to live attenuated alternatives.
Live attenuated vaccines, on the other hand, use weakened pathogens that retain their ability to replicate but are incapable of causing severe disease. This replication triggers a strong, long-lasting immune response, often requiring fewer doses. The yellow fever vaccine, for instance, is a live attenuated vaccine administered as a single dose, providing lifelong immunity for most recipients. However, these vaccines carry a small risk of reverting to a virulent form or causing adverse reactions in immunocompromised individuals. Thus, they are contraindicated for pregnant women, HIV patients, or those with severe allergies.
The choice between inactivated and attenuated whole pathogen vaccines depends on factors like safety, efficacy, and target population. Inactivated vaccines are preferred for vulnerable groups, such as infants or the immunocompromised, due to their safety profile. Attenuated vaccines, however, are ideal for healthy populations requiring durable immunity with minimal doses. For example, the oral typhoid vaccine (Ty21a) uses attenuated Salmonella typhi and is recommended for travelers to endemic regions, administered in 3–4 doses over 5–7 days. Practical tips include avoiding antibiotics during vaccination, as they can interfere with the live attenuated pathogen’s replication.
Despite their effectiveness, whole pathogen vaccines face challenges. Inactivated vaccines may require booster shots to maintain immunity, while attenuated vaccines pose theoretical risks in specific populations. Advances in technology, such as improved attenuation methods or adjuvant formulations, aim to enhance safety and efficacy. For instance, the development of the acellular pertussis vaccine reduced side effects by using only key antigens instead of the whole cell. Nonetheless, whole pathogen vaccines remain indispensable, particularly in low-resource settings where simplicity and cost-effectiveness are critical. Their ability to confer broad immunity with minimal infrastructure underscores their enduring value in global health.
Navy Enlistment: Vaccination Requirements and Exemptions
You may want to see also
Explore related products






![]()
Subunit Vaccines: Contains specific pathogen proteins or fragments to stimulate immunity safely
Subunit vaccines represent a precision approach to immunization, focusing on the most critical components of a pathogen to trigger a robust immune response without the risks associated with live or whole-dead pathogens. Unlike traditional vaccines, which use entire viruses or bacteria, subunit vaccines contain only specific proteins or fragments—often called antigens—that are essential for immune recognition. This targeted strategy minimizes side effects while maximizing safety, making subunit vaccines particularly suitable for vulnerable populations, such as the elderly, infants, and immunocompromised individuals. For instance, the hepatitis B vaccine uses a single protein, the hepatitis B surface antigen (HBsAg), to induce long-lasting immunity, demonstrating the efficacy of this approach.
Consider the process of creating a subunit vaccine: scientists identify key pathogen proteins through genetic sequencing and structural analysis, then produce these proteins in large quantities using recombinant DNA technology or chemical synthesis. This method ensures purity and consistency, eliminating the risk of accidental infection from the vaccine itself. For example, the acellular pertussis vaccine (DTaP) contains purified fragments of the *Bordetella pertussis* bacterium, such as pertussis toxin and filamentous hemagglutinin, which are critical for immunity but stripped of other components that could cause adverse reactions. This refinement reduces side effects like fever and swelling compared to the older whole-cell pertussis vaccine.
One of the standout advantages of subunit vaccines is their stability and ease of storage, particularly in resource-limited settings. Because they contain only purified proteins or peptides, they are less prone to degradation and often do not require stringent cold chain logistics. The human papillomavirus (HPV) vaccine, for instance, uses virus-like particles (VLPs) composed of the L1 protein, which self-assemble into structures resembling the virus but lack genetic material, ensuring safety and stability. This has facilitated its global distribution, contributing to significant reductions in cervical cancer rates.
However, the specificity of subunit vaccines can sometimes be a double-edged sword. While they are safer, they may require adjuvants—substances that enhance the immune response—to achieve sufficient immunity. For example, the shingles vaccine (Shingrix) combines a glycoprotein E antigen with a proprietary adjuvant system (AS01B) to stimulate a strong and durable immune response in adults over 50, a demographic at higher risk for shingles. Without such adjuvants, the immune response might be insufficient, underscoring the importance of formulation design in subunit vaccines.
In practical terms, subunit vaccines offer a versatile platform for addressing emerging pathogens. During the COVID-19 pandemic, several subunit vaccines, such as Novavax, were developed using recombinant spike proteins stabilized in their prefusion conformation. These vaccines provided an alternative to mRNA and viral vector technologies, catering to individuals with specific concerns or contraindications. Their approval highlighted the adaptability of subunit vaccines in rapidly evolving public health crises. For optimal protection, it’s crucial to follow dosing schedules—often two or three doses spaced weeks apart—to ensure the immune system mounts a full response. Always consult healthcare providers for personalized advice, especially regarding age-specific recommendations and potential interactions with other medications.
Is Tdap Vaccine Covered by Medicare Part D? Find Out
You may want to see also
Explore related products






![]()
Toxoid Vaccines: Includes inactivated toxins produced by pathogens to neutralize harmful effects
Toxoid vaccines represent a unique approach to immunization, targeting the harmful toxins produced by pathogens rather than the pathogens themselves. Unlike traditional vaccines that use weakened or killed pathogens, toxoid vaccines contain inactivated toxins, known as toxoids, which have been chemically treated to eliminate their toxicity while retaining their ability to stimulate an immune response. This strategy is particularly effective against diseases where the toxin, not the pathogen itself, is the primary cause of illness. Examples include tetanus and diphtheria, both of which are prevented by toxoid vaccines.
The process of creating a toxoid vaccine involves treating the toxin with formaldehyde, a process called formalin inactivation. This modifies the toxin’s structure, rendering it harmless but still recognizable by the immune system. When administered, the toxoid prompts the body to produce antibodies specifically tailored to neutralize the actual toxin if future exposure occurs. For instance, the tetanus toxoid vaccine, typically given as part of the DTaP (Diphtheria, Tetanus, and Pertussis) series in childhood, provides long-lasting immunity with booster doses recommended every 10 years for adults. Dosage varies by age: infants receive 0.5 mL per dose, while older children and adults receive 0.5 mL of the adsorbed product.
One of the key advantages of toxoid vaccines is their safety profile. Since they do not contain live or even dead pathogens, the risk of adverse reactions is significantly lower compared to other vaccine types. However, this also means that multiple doses are often required to build and maintain immunity. For example, the diphtheria toxoid vaccine is administered in a series of shots, starting at 2 months of age, followed by boosters at 4–6 years and every 10 years thereafter. Practical tips for recipients include scheduling boosters during routine health check-ups and keeping a vaccination record to track doses.
Comparatively, toxoid vaccines differ from subunit or mRNA vaccines, which target specific proteins or genetic material of a pathogen. Toxoid vaccines focus exclusively on the toxin, making them highly specialized tools in disease prevention. This specificity is both a strength and a limitation: while they are ineffective against non-toxin-mediated diseases, they excel in neutralizing toxin-based threats. For instance, while an mRNA vaccine like Pfizer’s COVID-19 vaccine targets the virus’s spike protein, the tetanus toxoid vaccine directly counteracts the tetanus toxin’s ability to cause muscle stiffness and spasms.
In conclusion, toxoid vaccines are a critical component of modern immunization strategies, offering targeted protection against toxin-mediated diseases. Their inactivated toxin components ensure safety and efficacy, making them suitable for diverse age groups, from infants to the elderly. By understanding their mechanism, dosage requirements, and practical administration tips, individuals can better appreciate the role of toxoid vaccines in public health and ensure timely vaccination to maintain immunity.
Vaccination Requirements for Entry into Canada
You may want to see also
Explore related products






![]()
Nucleic Acid Vaccines: Delivers genetic material (DNA/RNA) coding for pathogen antigens to produce immunity
Nucleic acid vaccines represent a groundbreaking shift in immunization technology by delivering genetic material—either DNA or RNA—that encodes for specific pathogen antigens. Unlike traditional vaccines, which use weakened or inactivated pathogens, or subunit vaccines that contain isolated proteins, nucleic acid vaccines instruct our cells to produce the antigen themselves. This approach harnesses the body’s own machinery to trigger an immune response, offering a precise and adaptable method for combating infectious diseases. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna’s COVID-19 vaccines deliver mRNA sequences coding for the SARS-CoV-2 spike protein, enabling cells to manufacture this antigen and elicit immunity without exposing the recipient to the virus.
The process begins with the administration of the vaccine, typically via intramuscular injection. Once inside the body, the genetic material enters cells, where it is transcribed (in the case of DNA vaccines) or directly translated (in the case of mRNA vaccines) into the target antigen. This antigen is then displayed on the cell surface, signaling immune cells to mount a response. Notably, the genetic material does not integrate into the host genome, ensuring safety and transient expression. Dosage is critical; for example, the Pfizer-BioNTech COVID-19 vaccine delivers 30 micrograms of mRNA per dose, while Moderna’s uses 100 micrograms. These doses are optimized to balance efficacy and minimize side effects, such as fatigue or injection site pain, which are generally mild and short-lived.
One of the most compelling advantages of nucleic acid vaccines is their rapid development potential. Traditional vaccines often require years of research and production, but nucleic acid vaccines can be designed and manufactured within weeks once the pathogen’s genetic sequence is known. This speed was pivotal during the COVID-19 pandemic, where mRNA vaccines were developed, tested, and deployed in under a year. Additionally, these vaccines can be easily modified to target emerging variants or entirely new pathogens, making them a versatile tool for future pandemics. For example, updated COVID-19 boosters now include mRNA coding for Omicron subvariant spike proteins, providing enhanced protection against evolving strains.
Despite their promise, nucleic acid vaccines are not without challenges. mRNA vaccines, in particular, require ultra-cold storage (e.g., -70°C for Pfizer’s vaccine) to maintain stability, which poses logistical hurdles in low-resource settings. DNA vaccines, while more stable, have shown lower immunogenicity in clinical trials, often requiring electroporation—a technique to enhance DNA uptake by cells—to improve efficacy. Age-specific considerations also play a role; these vaccines are generally approved for individuals aged 12 and older, with ongoing trials evaluating safety and efficacy in younger children. Practical tips for recipients include staying hydrated, resting after vaccination, and monitoring for rare but serious side effects like myocarditis, particularly in young males.
In conclusion, nucleic acid vaccines redefine immunization by delivering the genetic blueprint for pathogen antigens, enabling the body to produce its own immune triggers. Their speed, adaptability, and precision make them a cornerstone of modern vaccinology, as evidenced by their role in combating COVID-19. While challenges like storage and immunogenicity persist, ongoing research continues to refine these technologies. For those eligible, nucleic acid vaccines offer a safe, effective, and innovative way to protect against infectious diseases, marking a new era in global health.
Understanding Influenza Vaccine Components: What's Inside the Flu Shot?
You may want to see also
Explore related products



![]()
Viral Vector Vaccines: Uses modified viruses to deliver pathogen genes for immune response
Viral vector vaccines represent a sophisticated approach to immunization, leveraging the power of modified viruses to deliver specific pathogen genes into the body, thereby eliciting a targeted immune response. Unlike traditional vaccines that use weakened or inactivated pathogens, viral vector vaccines act as molecular delivery trucks, transporting genetic material directly to cells. This method is particularly effective for pathogens that are difficult to culture or pose safety risks in their whole form, such as HIV or malaria. The key lies in the precision of the delivery system: the vector virus is engineered to be harmless while retaining its ability to infect cells, ensuring the pathogen’s genes are expressed without causing disease.
Consider the Johnson & Johnson COVID-19 vaccine, a prime example of a viral vector vaccine. It employs a modified adenovirus (Ad26) to deliver the gene encoding the SARS-CoV-2 spike protein. Once administered, typically as a single 0.5 mL intramuscular dose for adults aged 18 and older, the adenovirus enters cells and releases the genetic instructions. The cells then produce the spike protein, which the immune system recognizes as foreign, triggering the production of antibodies and activation of T-cells. This mechanism not only provides robust protection but also demonstrates the versatility of viral vectors in addressing emerging pathogens.
One of the standout advantages of viral vector vaccines is their adaptability. The same vector can be repurposed to target different pathogens by simply swapping out the inserted genes. For instance, the Oxford-AstraZeneca COVID-19 vaccine uses a chimpanzee adenovirus (ChAdOx1) as its vector, a platform previously tested in vaccines for Ebola and MERS. This modularity accelerates vaccine development during outbreaks, as seen in the rapid deployment of COVID-19 vaccines. However, this approach is not without challenges. Pre-existing immunity to the vector virus can reduce vaccine efficacy, as some individuals may have antibodies that neutralize the vector before it delivers its payload.
Practical considerations for viral vector vaccines include dosage, administration, and target populations. For optimal efficacy, precise dosing is critical; the Moderna and Pfizer mRNA vaccines, for comparison, require 0.3 mL and 0.5 mL doses, respectively, while viral vector vaccines often use a single dose. Storage conditions are also less stringent than for mRNA vaccines, making them more accessible in resource-limited settings. However, healthcare providers must screen for contraindications, such as severe allergic reactions to vaccine components. For parents, it’s essential to note that viral vector vaccines are currently approved for adults, with pediatric formulations still under study.
In conclusion, viral vector vaccines exemplify the intersection of biology and engineering, offering a dynamic solution to the challenge of pathogen-specific immunity. By delivering only the essential genetic material, they minimize risks while maximizing immune response. As research progresses, their role in combating both established and emerging diseases will likely expand, underscoring their importance in the global vaccine arsenal. Whether addressing a pandemic or routine immunization, viral vector vaccines stand as a testament to the ingenuity of modern medicine.
Debunking Myths: Peer-Reviewed Research on Autism and Vaccines
You may want to see also
Frequently asked questions
Vaccines often contain a weakened or inactivated form of the pathogen, a specific protein or sugar from its surface, or a fragment of its genetic material (like mRNA or viral DNA).
Using only a piece of the pathogen reduces the risk of causing disease while still triggering a strong immune response, making vaccines safer and more effective.
Yes, mRNA vaccines contain a small piece of the pathogen’s genetic code (mRNA) that instructs cells to produce a harmless protein, which then triggers an immune response.
No, different vaccines target specific pieces of a pathogen depending on the type of vaccine (e.g., live-attenuated, inactivated, protein subunit, or mRNA) and the pathogen itself.