Hepatitis, a liver inflammation often caused by viral infections, encompasses several strains, including Hepatitis A, B, C, D, and E. Among these, Hepatitis A and B are the primary strains preventable through vaccination. The Hepatitis A vaccine offers highly effective protection against the virus, typically transmitted through contaminated food or water, while the Hepatitis B vaccine safeguards against a more severe form of the disease, primarily spread through blood, sexual contact, or from mother to child during birth. Both vaccines are widely available and recommended for at-risk populations, playing a crucial role in global efforts to reduce the burden of hepatitis-related illnesses and complications.
| Characteristics | Values |
|---|---|
| Hepatitis Strains Preventable by Vaccine | Hepatitis A (HAV), Hepatitis B (HBV), Hepatitis E (HEV) |
| Vaccine Availability | Widely available for HAV and HBV; HEV vaccine available in some countries (e.g., China, Europe) |
| Vaccine Type | Inactivated virus (HAV, HBV), Recombinant protein (HBV), Inactivated virus (HEV) |
| Dose Schedule (HAV) | 2 doses, 6–12 months apart |
| Dose Schedule (HBV) | 3 doses (0, 1–2, 6 months) |
| Dose Schedule (HEV) | 3 doses (0, 1, 6 months) |
| Effectiveness (HAV) | >95% after 2 doses |
| Effectiveness (HBV) | 98–100% after 3 doses |
| Effectiveness (HEV) | ~87% after 3 doses (based on available data) |
| Duration of Protection (HAV) | Long-term, likely lifelong |
| Duration of Protection (HBV) | Long-term, likely lifelong |
| Duration of Protection (HEV) | At least 4.5 years (data still evolving) |
| Target Population | All ages (HAV, HBV); travelers, pregnant women, and at-risk groups (HEV) |
| Combination Vaccines | Available for HAV + HBV |
| Global Impact | Prevention of acute hepatitis, cirrhosis, and liver cancer |
| WHO Recommendation | Routine immunization for HAV and HBV; HEV vaccine in endemic areas or for at-risk groups |
Explore related products






What You'll Learn
- Hepatitis A Vaccine: Highly effective, prevents HAV, administered in two doses, six months apart
- Hepatitis B Vaccine: Prevents HBV, part of infant immunization schedules worldwide
- Combined A & B Vaccine: Offers protection against both HAV and HBV in one vaccine
- Hepatitis D Prevention: No specific vaccine; prevented by Hepatitis B vaccination
- Hepatitis E Vaccine: Limited availability, primarily used in high-risk regions
![]()
Hepatitis A Vaccine: Highly effective, prevents HAV, administered in two doses, six months apart
Hepatitis A, a liver infection caused by the hepatitis A virus (HAV), is entirely preventable with a highly effective vaccine. This vaccine stands out as a cornerstone in public health efforts to combat viral hepatitis, offering robust protection against a strain that, while often self-limiting, can cause severe complications in certain populations. Administered in two doses, typically six months apart, it provides long-term immunity, making it a vital tool for both individual and community health.
From an analytical perspective, the hepatitis A vaccine’s efficacy is well-documented, with studies showing over 95% seroprotection after the full series. This means that nearly all vaccinated individuals develop antibodies sufficient to neutralize the virus. The dosing schedule—an initial shot followed by a booster six months later—is designed to maximize immune response and ensure lasting defense. This regimen is particularly crucial for travelers to endemic regions, healthcare workers, and individuals with chronic liver disease, who face higher risks of severe outcomes from HAV infection.
For those considering vaccination, the process is straightforward but requires adherence to the timeline. The first dose provides immediate protection, but the second dose is essential for long-term immunity. Practical tips include scheduling reminders for the booster and inquiring about combination vaccines, such as those that protect against both hepatitis A and B, which may be more convenient for certain individuals. The vaccine is approved for children as young as 12 months and adults, with no upper age limit, making it accessible to a broad demographic.
Comparatively, while hepatitis B and hepatitis A vaccines share similarities in their two-dose structure, the HAV vaccine’s efficacy is notable for its near-universal success in preventing infection. Unlike hepatitis C, which currently has no vaccine, hepatitis A’s preventable nature underscores the importance of proactive immunization. This distinction highlights the vaccine’s role as a definitive solution to a specific strain, rather than a partial or experimental measure.
In conclusion, the hepatitis A vaccine is a prime example of preventive medicine’s power. Its high efficacy, simple dosing schedule, and broad applicability make it an indispensable resource in the fight against viral hepatitis. By understanding its specifics and following through with vaccination, individuals can safeguard their health and contribute to reducing the global burden of HAV.
Post-Vaccine Lethargy in Babies: Understanding Normal Reactions and Concerns
You may want to see also
Explore related products






![]()
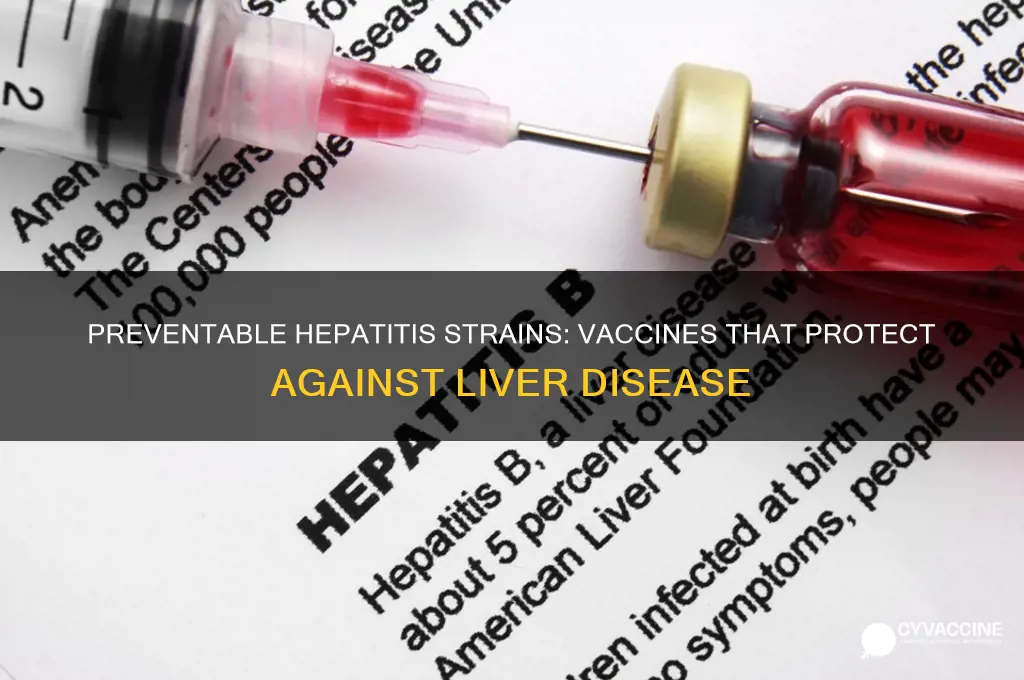
Hepatitis B Vaccine: Prevents HBV, part of infant immunization schedules worldwide
Hepatitis B (HBV) is a vaccine-preventable liver infection caused by the hepatitis B virus, and its prevention is a cornerstone of global public health efforts. Unlike hepatitis A, which is primarily transmitted through contaminated food or water, HBV spreads through contact with infected blood, semen, or other bodily fluids. This distinction makes HBV a more insidious threat, often silently transmitted from mother to child during birth or through unsafe medical practices. The hepatitis B vaccine, introduced in the 1980s, has since become a critical tool in combating this disease, offering nearly 100% protection against HBV when administered correctly.
The inclusion of the hepatitis B vaccine in infant immunization schedules worldwide is a testament to its importance. Most countries recommend a three-dose series for infants, typically starting at birth. The first dose, administered within 24 hours of birth, is crucial for preventing perinatal transmission. Subsequent doses are given at 1–2 months and 6–18 months of age, depending on the national schedule. For example, the U.S. Centers for Disease Control and Prevention (CDC) recommends the 0-1-6 month schedule, while some countries opt for a 0-1-2 month regimen. This early vaccination not only protects infants but also helps establish herd immunity, reducing the overall prevalence of HBV in communities.
While the vaccine is highly effective, adherence to the schedule is essential. Missing doses can leave individuals vulnerable to infection. For older children and adults who were not vaccinated as infants, a "catch-up" schedule is available. Adults typically receive a three-dose series over six months, with higher antigen doses compared to the pediatric formulation. Travelers to regions with high HBV prevalence, healthcare workers, and individuals with multiple sexual partners are particularly encouraged to get vaccinated. It’s worth noting that the vaccine is safe for pregnant women and those with chronic liver disease, making it accessible to a broad population.
One of the most compelling aspects of the hepatitis B vaccine is its long-term efficacy. Studies show that protection lasts for at least 20 years, and likely a lifetime, in most individuals. Even if antibody levels decline over time, immune memory cells provide continued protection against infection. This durability sets the HBV vaccine apart from others that may require periodic boosters. However, individuals at high risk, such as those with weakened immune systems, may benefit from periodic antibody testing to ensure ongoing immunity.
Incorporating the hepatitis B vaccine into infant immunization schedules is a practical and cost-effective strategy for global health. It not only prevents acute HBV infections but also reduces the risk of chronic complications like cirrhosis and liver cancer. For parents, ensuring their child receives the vaccine on time is a simple yet powerful way to safeguard their future health. Healthcare providers play a critical role in educating families about the vaccine’s importance and dispelling myths, such as unfounded concerns about safety. With widespread vaccination, the vision of a world free from hepatitis B is within reach.
Debunking Myths: Can Vaccines Be Removed from the Body?
You may want to see also
Explore related products






![]()
Combined A & B Vaccine: Offers protection against both HAV and HBV in one vaccine
Hepatitis A and B are two distinct but potentially severe liver infections caused by the hepatitis A virus (HAV) and hepatitis B virus (HBV), respectively. While both can lead to acute illness, HBV is particularly concerning due to its potential to cause chronic liver disease, cirrhosis, and liver cancer. Fortunately, vaccination offers a powerful tool to prevent these outcomes. The combined A & B vaccine is a convenient and effective solution, providing protection against both viruses in a single immunization series.
This dual-action vaccine is typically administered as a series of three intramuscular injections, with the second dose given one month after the first and the third dose administered six months after the initial shot. The standard dosage for adults and adolescents is 1 mL per dose, while children aged 1 to 15 years receive a reduced volume of 0.5 mL. It’s important to note that the combined vaccine is approved for individuals aged one year and older, making it a versatile option for a wide age range. For travelers to regions with high prevalence of HAV and HBV, this vaccine is particularly valuable, as it simplifies the immunization process and ensures comprehensive protection.
One of the key advantages of the combined A & B vaccine is its ability to streamline prevention efforts. Instead of requiring separate vaccines for HAV and HBV, individuals receive dual protection through a single series. This not only reduces the number of injections needed but also improves adherence to vaccination schedules. For healthcare providers, it simplifies inventory management and administration, making it a practical choice for clinics and immunization programs. Additionally, the vaccine has been shown to be highly immunogenic, with studies indicating that over 95% of recipients develop protective antibody levels after completing the series.
However, it’s essential to consider contraindications and precautions. Individuals with a history of severe allergic reactions to any component of the vaccine, including yeast or latex, should avoid it. Pregnant women can receive the vaccine if the benefits outweigh the risks, but it’s generally recommended to defer vaccination until after pregnancy unless there’s a high risk of exposure. Mild side effects, such as soreness at the injection site, headache, or fatigue, are common but typically resolve within a few days. For optimal protection, ensure all doses are completed as scheduled, as partial vaccination may not provide adequate immunity.
Incorporating the combined A & B vaccine into routine immunization practices can significantly reduce the global burden of hepatitis A and B. It is especially beneficial for at-risk groups, including healthcare workers, international travelers, men who have sex with men, and individuals with chronic liver disease. By offering dual protection in a single vaccine, it represents a practical and efficient approach to hepatitis prevention, aligning with public health goals to eliminate viral hepatitis as a major health threat. For those eligible, this vaccine is a straightforward yet powerful step toward safeguarding liver health.
Optimal Needle Change Practices for Safe Livestock Vaccination Procedures
You may want to see also
Explore related products






![]()
Hepatitis D Prevention: No specific vaccine; prevented by Hepatitis B vaccination
Hepatitis D, a liver infection caused by the hepatitis D virus (HDV), is unique in that it can only occur in individuals already infected with hepatitis B (HBV). This dependency on HBV for replication means that preventing hepatitis B effectively prevents hepatitis D. Despite the absence of a specific vaccine for hepatitis D, the hepatitis B vaccine serves as a powerful tool to combat both infections. This dual protection underscores the critical importance of widespread hepatitis B vaccination.
The hepatitis B vaccine is administered in a series of three doses, typically given at 0, 1, and 6 months. For infants, the first dose is recommended within 24 hours of birth, followed by the second dose at 1–2 months and the third dose at 6–18 months. Adults and adolescents can follow a similar schedule, though accelerated options are available in certain situations. Ensuring timely completion of the vaccine series is crucial, as it provides over 90% protection against HBV and, by extension, HDV.
One of the most effective strategies to prevent hepatitis D is to target at-risk populations for hepatitis B vaccination. These include healthcare workers, individuals with multiple sexual partners, injection drug users, and those living in regions with high HBV prevalence. For example, in countries like Mongolia and the Amazon Basin, where both HBV and HDV are endemic, vaccination campaigns have significantly reduced the incidence of both infections. Public health initiatives should prioritize these areas to maximize impact.
While the hepatitis B vaccine is highly effective, it is not foolproof. Breakthrough infections can occur, particularly in immunocompromised individuals or those with waning immunity. Booster doses are generally not required for healthy individuals, but antibody level testing may be recommended for those at high risk. Additionally, practicing safe behaviors, such as using sterile needles and practicing safe sex, complements vaccination efforts by reducing exposure to HBV and, consequently, HDV.
In summary, the prevention of hepatitis D hinges entirely on the prevention of hepatitis B through vaccination. By adhering to the recommended vaccine schedule and targeting at-risk populations, public health systems can effectively curb the spread of both viruses. This approach not only saves lives but also reduces the global burden of liver disease, highlighting the hepatitis B vaccine as a cornerstone of hepatitis D prevention.
Vaccine Tracking Systems: How Governments Monitor Immunization Records
You may want to see also
Explore related products






![]()
Hepatitis E Vaccine: Limited availability, primarily used in high-risk regions
Hepatitis E, a liver disease caused by the hepatitis E virus (HEV), is often overshadowed by its more widely recognized counterparts, yet it poses significant health risks, particularly in certain regions. Unlike hepatitis A and B, which have globally available vaccines, the hepatitis E vaccine remains a niche intervention, primarily accessible in China and a few other countries. This limited availability raises questions about its role in global health strategies and underscores the challenges of addressing region-specific diseases.
From an analytical perspective, the hepatitis E vaccine, known as Hecolin, is a prime example of a targeted medical solution. Developed by Xiamen Innovax Biotech in China, it is administered in a three-dose regimen, typically given at 0, 1, and 6 months. The vaccine has demonstrated efficacy rates exceeding 90% in clinical trials, making it a powerful tool in high-prevalence areas. However, its distribution remains confined to regions with high endemicity, such as parts of Asia, Africa, and the Middle East, where HEV is often transmitted through contaminated water. This regional focus highlights the economic and logistical barriers to global vaccine rollout, as pharmaceutical companies prioritize markets with immediate demand and regulatory approval.
For individuals living in or traveling to high-risk regions, understanding the hepatitis E vaccine’s availability and administration is crucial. Travelers to endemic areas, particularly pregnant women—who face a higher risk of severe complications from HEV infection—should consult healthcare providers about vaccination options. While the vaccine is not yet approved in many Western countries, some travelers opt to receive it in China or other countries where it is licensed. Practical tips include ensuring the vaccine is stored and administered under proper conditions, as it requires refrigeration, and verifying the authenticity of the product, given the risk of counterfeit medications in some regions.
Comparatively, the hepatitis E vaccine’s limited availability contrasts sharply with the widespread accessibility of hepatitis A and B vaccines, which are included in routine immunization schedules globally. This disparity reflects broader inequalities in global health, where diseases affecting low- and middle-income countries often receive less investment in prevention and treatment. While efforts to expand access to the hepatitis E vaccine are ongoing, including potential approvals in Europe, the current landscape underscores the need for international collaboration to address neglected tropical diseases.
In conclusion, the hepatitis E vaccine stands as a critical yet underutilized tool in the fight against HEV, primarily due to its restricted availability. For those in high-risk regions or planning travel to such areas, awareness of this vaccine and its administration protocols can be life-saving. As global health initiatives evolve, expanding access to such targeted interventions will be essential to reducing the burden of hepatitis E and other region-specific diseases.
Allergies and Live Vaccines: Which Shots to Avoid for Safety
You may want to see also
Frequently asked questions
Hepatitis A and Hepatitis B are the strains that are preventable with vaccines.
No, there is currently no vaccine available for Hepatitis C, though research is ongoing.
The Hepatitis B vaccine specifically protects against Hepatitis B virus (HBV) and does not provide protection against other strains like Hepatitis A, C, D, or E.
Yes, there is a combined vaccine available that protects against both Hepatitis A and Hepatitis B, offering convenience for those needing both immunizations.