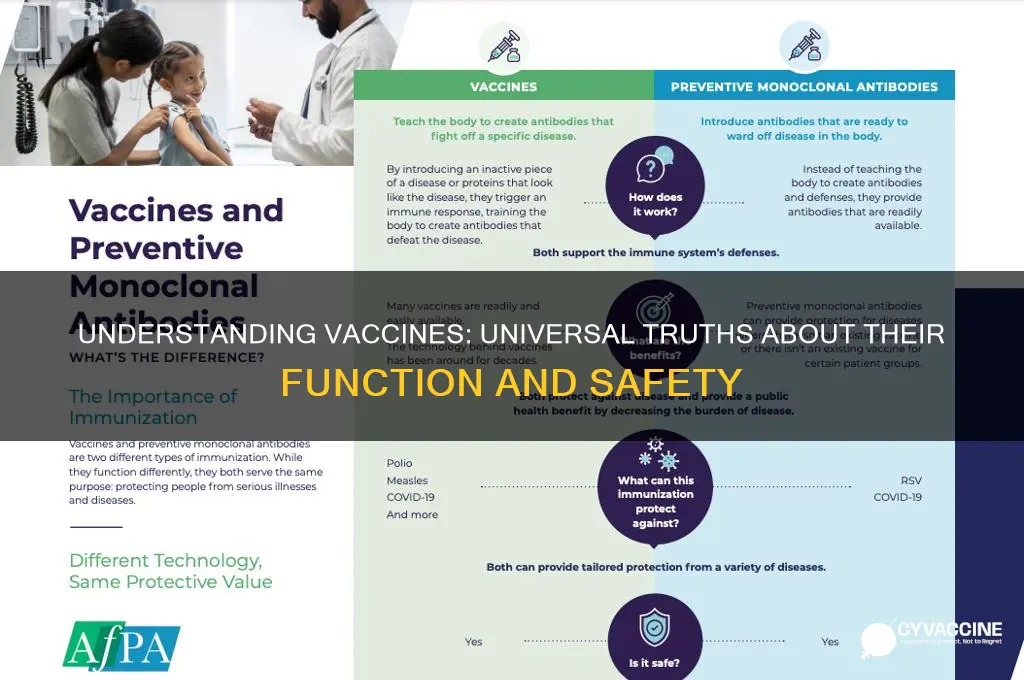
Vaccines are a cornerstone of public health, designed to stimulate the immune system to recognize and combat specific pathogens, thereby preventing or reducing the severity of diseases. When considering the statement which of the following is true of all vaccines, it is essential to recognize that while vaccines share a common purpose, they vary widely in their composition, mechanisms, and administration. For instance, all vaccines aim to induce immunity, but they may use different approaches such as live attenuated viruses, inactivated pathogens, mRNA technology, or protein subunits. Additionally, not all vaccines provide lifelong immunity, as some require booster shots to maintain protection. Therefore, while the overarching goal of preventing disease is universal, the specifics of how each vaccine achieves this can differ significantly.
| Characteristics | Values |
|---|---|
| Purpose | Prevent infectious diseases by inducing an immune response |
| Composition | Contain antigens (weakened/killed pathogens or their components) |
| Administration | Typically given via injection, orally, or nasally |
| Immune Response | Stimulate the production of antibodies and memory cells |
| Safety | Rigorously tested for safety and efficacy before approval |
| Side Effects | Generally mild (e.g., soreness, fever) and rare severe reactions |
| Effectiveness | High efficacy in preventing targeted diseases |
| Duration of Protection | Varies; some require boosters for continued immunity |
| Storage Requirements | Specific conditions (e.g., refrigeration) to maintain potency |
| Global Impact | Significantly reduce morbidity and mortality from vaccine-preventable diseases |
| Regulation | Approved and monitored by health authorities (e.g., FDA, WHO) |
| Herd Immunity | Contribute to community protection when widely administered |
| Development Time | Typically takes years, though expedited in emergencies (e.g., COVID-19) |
| Cost | Varies by region; many are subsidized or free in public health programs |
| Accessibility | Global efforts to improve access, especially in low-income countries |
Explore related products

$23.58 $32.99





What You'll Learn
- Vaccines undergo rigorous testing for safety and efficacy before approval by regulatory authorities
- All vaccines aim to stimulate the immune system to prevent specific diseases
- Side effects from vaccines are typically mild and temporary, such as soreness or fever
- Vaccines do not cause the diseases they are designed to prevent
- Herd immunity depends on widespread vaccination to protect vulnerable populations effectively
![]()
Vaccines undergo rigorous testing for safety and efficacy before approval by regulatory authorities
Vaccines are not rushed to market. Before any vaccine receives approval, it undergoes a meticulous, multi-stage testing process that can span years, even decades. This process is designed to ensure not just that the vaccine works, but that it is safe for widespread use across diverse populations. The journey begins with preclinical testing, where potential vaccines are studied in laboratories and animal models to assess their basic safety and immunogenicity. Only the most promising candidates progress to human trials, which are divided into three phases. Phase 1 trials involve a small group of healthy volunteers (typically 20-100 individuals) to evaluate safety, dosage, and immune response. Phase 2 expands to several hundred participants to further assess safety and efficacy, often including specific demographics like children or the elderly. Phase 3 trials are the largest, involving thousands to tens of thousands of people, to confirm efficacy, monitor side effects, and compare the vaccine to a placebo or existing vaccine. Even after approval, vaccines are continuously monitored through Phase 4 trials and surveillance systems like the Vaccine Adverse Event Reporting System (VAERS) in the U.S., ensuring long-term safety and effectiveness.
Consider the COVID-19 vaccines, which were developed at an unprecedented pace but still adhered to these rigorous standards. Despite the urgency, no steps were skipped. For instance, the Pfizer-BioNTech vaccine’s Phase 3 trial included over 43,000 participants, with half receiving the vaccine and half a placebo. The trial specifically tracked outcomes like severe COVID-19 cases and side effects, which were overwhelmingly mild (e.g., fatigue, headache) and short-lived. Regulatory authorities like the FDA and EMA reviewed all data before granting emergency use authorization, ensuring the benefits far outweighed the risks. This process was transparent, with data published in peer-reviewed journals like *The New England Journal of Medicine*, allowing independent scientists to scrutinize the findings.
One common misconception is that vaccine testing is less stringent for certain populations, like children. In reality, pediatric vaccines often require even more careful scrutiny. For example, the MMR (measles, mumps, rubella) vaccine was tested in multiple trials involving infants and young children to confirm its safety and efficacy at specific dosages (0.5 mL for the first dose at 12-15 months and a second dose at 4-6 years). Similarly, the HPV vaccine underwent extensive testing in adolescents aged 9-26 to ensure its effectiveness in preventing cervical cancer and other HPV-related diseases. Parents can take practical steps to ensure their children’s safety, such as reviewing the vaccine information sheet (VIS) provided by healthcare providers, which outlines potential side effects and contraindications.
Critics often argue that expedited approvals compromise safety, but this is a misunderstanding of how regulatory flexibility works. For example, the FDA’s Fast Track and Priority Review programs allow for accelerated timelines without bypassing safety checks. These programs focus on streamlining administrative processes, such as rolling submissions of trial data, rather than reducing the rigor of testing. Similarly, emergency use authorizations (EUAs) are granted only when there is sufficient evidence of safety and efficacy from Phase 3 trials, and they are temporary, requiring full approval after additional data is collected. This balance ensures that life-saving vaccines can reach the public quickly without sacrificing the standards that protect us.
In practical terms, understanding the testing process can empower individuals to make informed decisions. For instance, knowing that vaccines are tested across diverse age groups can reassure older adults or those with chronic conditions about their safety. Similarly, awareness of post-approval monitoring systems like the CDC’s Vaccine Safety Datalink (VSD) can provide confidence in ongoing oversight. For travelers, checking the specific vaccines required for their destination and understanding their testing history can ensure preparedness. Ultimately, the rigorous testing of vaccines is not just a regulatory requirement—it’s a cornerstone of public trust and global health.
Ireland's MMR Vaccine Introduction: A Historical Timeline and Impact
You may want to see also
Explore related products






![]()
All vaccines aim to stimulate the immune system to prevent specific diseases
Vaccines are designed with a singular, critical purpose: to train the immune system to recognize and combat specific pathogens before they cause disease. This process begins with the introduction of a harmless component of the pathogen, such as a protein or a weakened version of the virus or bacterium. For instance, the measles, mumps, and rubella (MMR) vaccine contains live but attenuated (weakened) viruses, while the COVID-19 mRNA vaccines deliver genetic instructions for cells to produce a harmless piece of the virus’s spike protein. Regardless of the type, the goal is consistent: to provoke an immune response that includes the production of antibodies and the activation of memory cells, which stand ready to mount a rapid defense if the real pathogen is encountered.
Consider the influenza vaccine, which is reformulated annually to match the most prevalent strains. It typically contains inactivated virus particles, administered in a single 0.5 mL dose for adults and children over 6 months. The immune system responds by generating antibodies within about two weeks, offering protection during flu season. This example underscores a key principle: vaccines are tailored to target specific diseases, and their effectiveness depends on the immune system’s ability to "remember" the pathogen. For optimal results, follow vaccination schedules closely, as timing and dosage are calibrated to maximize immune response without overwhelming the body.
A persuasive argument for the universality of this aim lies in the diversity of vaccine types and their shared outcome. Whether it’s the oral polio vaccine, which uses a live but weakened virus to confer gut immunity, or the HPV vaccine, which employs virus-like particles to prevent cervical cancer, all vaccines converge on the same endpoint: disease prevention through immune stimulation. Even newer technologies, like mRNA vaccines, adhere to this principle by teaching cells to produce a pathogen-specific antigen, triggering a targeted immune response. This consistency across vaccine platforms highlights the fundamental truth that immune stimulation is the cornerstone of vaccination.
Comparatively, the immune response elicited by vaccines differs from natural infection in one crucial way: it bypasses the disease itself. For example, a natural chickenpox infection exposes the body to the full varicella-zoster virus, leading to itchy blisters and potential complications like bacterial skin infections. In contrast, the varicella vaccine introduces a weakened form of the virus, stimulating immunity without causing severe illness. This controlled approach not only prevents the targeted disease but also reduces the risk of transmission, as vaccinated individuals are less likely to carry and spread the pathogen. Practical tip: keep a vaccination record to track doses and due dates, ensuring continuous protection.
In conclusion, the unifying truth about vaccines is their shared objective to harness the immune system’s power to prevent specific diseases. From traditional inactivated vaccines to cutting-edge mRNA technologies, each type is engineered to provoke a protective immune response without causing the disease itself. Understanding this principle empowers individuals to make informed decisions about vaccination, following recommended schedules and dosages for themselves and their families. By stimulating immunity in a safe, controlled manner, vaccines remain one of the most effective tools in public health, saving millions of lives annually.
England's Vaccination Progress: Current Rates and Key Insights
You may want to see also
Explore related products






![]()
Side effects from vaccines are typically mild and temporary, such as soreness or fever
Vaccines, by design, stimulate the immune system to build protection against diseases, and this process can sometimes lead to side effects. These reactions are generally mild and short-lived, serving as a sign that the body is responding to the vaccine. Common side effects include soreness at the injection site, fatigue, headache, muscle pain, and low-grade fever. For instance, the COVID-19 mRNA vaccines frequently cause arm soreness in over 70% of recipients, with fever occurring in about 10–15% of cases, typically resolving within 1–2 days. These symptoms are not only temporary but also far less severe than the potential complications of the diseases vaccines prevent.
From an analytical perspective, the mild nature of vaccine side effects is rooted in their mechanism of action. Vaccines introduce a harmless piece of a pathogen (or a weakened/dead version of it) to train the immune system without causing illness. This controlled exposure can trigger inflammation or immune activity, leading to symptoms like redness, swelling, or fever. For example, the flu vaccine often causes soreness at the injection site due to local immune activation, while the MMR vaccine may induce a mild fever as the body mounts a systemic response. These reactions are both predictable and manageable, typically requiring no medical intervention beyond rest and hydration.
For parents and caregivers, understanding these side effects is crucial for managing expectations and ensuring comfort post-vaccination. Children, in particular, may experience fussiness or loss of appetite after vaccines like DTaP or Hib, but these symptoms usually subside within 24–48 hours. Practical tips include applying a cool, wet washcloth to the injection site to reduce soreness and administering age-appropriate doses of acetaminophen or ibuprofen for fever or discomfort, following healthcare provider guidance. It’s also important to monitor for rare severe reactions, such as high fever or persistent crying, and seek medical attention if they occur.
Comparatively, the mild side effects of vaccines stand in stark contrast to the risks of the diseases they prevent. For example, measles can lead to pneumonia, encephalitis, and even death, while polio causes paralysis. The temporary discomfort of a vaccine is a small price to pay for lifelong immunity against such devastating illnesses. This perspective underscores the importance of viewing mild side effects not as drawbacks but as indicators of a functioning immune response. By reframing these reactions as a normal part of the vaccination process, individuals can approach immunization with confidence and clarity.
In conclusion, the mild and temporary side effects of vaccines, such as soreness or fever, are a testament to their safety and efficacy. These reactions are not only expected but also manageable with simple measures. Understanding their nature and purpose empowers individuals to make informed decisions and reinforces the value of vaccination in protecting public health. Whether for routine childhood immunizations or novel vaccines like those for COVID-19, recognizing these side effects as a sign of immune engagement highlights the remarkable balance vaccines strike between protection and tolerability.
Debunking Anti-Vaccine Myths: Evidence-Based Strategies to Counter False Claims
You may want to see also
Explore related products






![]()
Vaccines do not cause the diseases they are designed to prevent
Vaccines are meticulously designed to train the immune system without causing the disease they target. This is achieved through the use of weakened or inactivated pathogens, specific components of the pathogen, or genetic material that codes for a harmless piece of the pathogen. For example, the measles, mumps, and rubella (MMR) vaccine contains live attenuated viruses that are significantly weakened, allowing them to stimulate immunity without causing the full-blown disease. Similarly, mRNA vaccines like Pfizer-BioNTech and Moderna’s COVID-19 vaccines deliver genetic instructions for cells to produce a harmless spike protein, triggering an immune response without introducing the actual virus. This targeted approach ensures that vaccines mimic infection just enough to build immunity, but not enough to cause illness.
Consider the influenza vaccine, which is administered annually to millions worldwide. It contains inactivated or fragmented viral components, rendering it incapable of replicating or causing the flu. Despite this, some individuals may experience mild symptoms like soreness at the injection site or low-grade fever, which are not the disease itself but rather signs of the immune system responding to the vaccine. These reactions are a normal part of the immune process and should not be confused with the flu. Understanding this distinction is crucial for dispelling the myth that vaccines cause the diseases they prevent.
From a practical standpoint, parents and caregivers should follow age-specific vaccine schedules to ensure optimal protection without risk of disease transmission. For instance, the rotavirus vaccine is given orally to infants in multiple doses starting at 2 months of age. The virus in the vaccine is weakened to the point where it cannot cause severe diarrhea, the hallmark of rotavirus infection, but still prompts the immune system to produce protective antibodies. Adhering to recommended dosages and timing ensures that vaccines remain safe and effective, reinforcing their role as disease preventers, not causers.
Critics often point to rare cases of vaccine-related adverse events as evidence of vaccines causing diseases. However, these instances are distinct from the diseases themselves. For example, the oral polio vaccine (OPV) contains a live attenuated virus that, in extremely rare cases (about 1 in 2.7 million doses), can revert to a form capable of causing paralysis. This is not polio acquired from the wild virus but a vaccine-associated event. Modern vaccines, like the inactivated polio vaccine (IPV), eliminate even this minuscule risk by using a non-living form of the virus. Such advancements highlight the rigorous safety measures in vaccine development, ensuring they remain tools of prevention, not causation.
In conclusion, the assertion that vaccines do not cause the diseases they prevent is grounded in their scientific design and decades of real-world application. By using weakened, inactivated, or partial components of pathogens, vaccines activate the immune system without inducing illness. Practical adherence to dosing guidelines and awareness of normal immune responses further solidify their safety. While rare adverse events exist, they are not the diseases vaccines aim to prevent and are continually minimized through technological advancements. This clarity is essential for building trust in vaccines as a cornerstone of public health.
New York's Vaccination Laws: Updates, Changes, and Public Health Impact
You may want to see also
Explore related products






![]()
Herd immunity depends on widespread vaccination to protect vulnerable populations effectively
Vaccines are not just individual shields against disease; they are collective tools that fortify entire communities. Herd immunity, the indirect protection that occurs when a large portion of a population becomes immune to a disease, hinges on widespread vaccination. This phenomenon is particularly crucial for safeguarding vulnerable populations—infants too young to be vaccinated, the elderly with weakened immune systems, and individuals with medical conditions that prevent immunization. For example, the measles vaccine requires at least 93–95% of the population to be vaccinated to achieve herd immunity, effectively halting the disease’s spread and protecting those who cannot receive the vaccine. Without this collective effort, outbreaks can occur, putting these vulnerable groups at grave risk.
Achieving herd immunity is not a passive process; it demands active participation and strategic planning. Vaccination campaigns must target specific age groups and demographics to maximize coverage. For instance, the influenza vaccine is annually recommended for everyone aged 6 months and older, with particular emphasis on pregnant women, healthcare workers, and individuals over 65. However, herd immunity for influenza is more challenging to attain due to the virus’s rapid mutation, requiring consistent vaccination efforts and high uptake rates. Practical tips for communities include hosting vaccination clinics in schools, workplaces, and community centers, as well as leveraging digital reminders and incentives to encourage participation.
Critics often question the necessity of herd immunity, arguing that individual immunity should suffice. Yet, this perspective overlooks the interconnectedness of public health. A comparative analysis of smallpox and polio eradication efforts highlights the power of collective vaccination. Smallpox was eradicated globally in 1980 through a coordinated vaccination campaign, while polio persists in a few regions due to incomplete immunization coverage. The takeaway is clear: even highly effective vaccines like the polio vaccine, which provides immunity after 3 doses, cannot eliminate a disease without widespread adoption. Herd immunity is not just a theoretical concept—it’s a proven strategy that relies on societal commitment.
To effectively protect vulnerable populations, policymakers and healthcare providers must address barriers to vaccination, such as misinformation, access issues, and hesitancy. Persuasive communication that emphasizes the communal benefits of vaccination can shift public perception. For example, framing vaccination as a civic duty rather than a personal choice has been shown to increase uptake. Additionally, ensuring vaccines are affordable and accessible, particularly in underserved areas, is critical. A descriptive example is the success of the HPV vaccine in Australia, where a school-based program achieved over 70% coverage, significantly reducing cervical cancer rates. Such initiatives demonstrate that with the right approach, herd immunity can be a tangible reality, not just an aspirational goal.
Choosing the Right Vaccine Color: Personalized Recommendations for Optimal Health
You may want to see also
Frequently asked questions
No, not all vaccines provide lifelong immunity. Some vaccines require booster shots to maintain protection.
No, not all vaccines are made from live viruses. Some use inactivated viruses, protein subunits, or mRNA technology.
No, not all vaccines prevent infection entirely. Some primarily reduce the severity of symptoms or prevent serious illness.
No, vaccine effectiveness can vary depending on factors like age, health status, and individual immune response.
No, side effects vary by vaccine type. Common side effects include soreness, fatigue, or mild fever, but specifics differ.