Vaccine administration codes are a critical component of medical billing and coding, ensuring accurate reimbursement for healthcare providers who administer vaccines. These codes, typically found in the CPT (Current Procedural Terminology) code set, specify the method, route, and complexity of vaccine administration, rather than the vaccine product itself. Understanding which statements are true about these codes is essential for proper claim submission, as they directly impact billing accuracy and compliance with payer guidelines. For instance, it’s important to know whether these codes include counseling, the number of vaccines administered, or if they are age-specific, as misconceptions can lead to claim denials or underpayment.
| Characteristics | Values |
|---|---|
| Purpose | Used to bill for the service of administering a vaccine, not the vaccine itself. |
| CPT Code Range | 90460, 90461, 90471, 90472, 90473, 90474 (as of latest updates). |
| Age-Specific Codes | Some codes are specific to age groups (e.g., 90460 for 0-18 years). |
| Dose-Specific Codes | Certain codes apply based on the number of components in the vaccine. |
| Billing Guidelines | Must be billed separately from the vaccine product code (e.g., CPT 90716). |
| Modifier Usage | Modifiers like -LT, -RT, or -50 may be used for specific administration scenarios. |
| Reimbursement | Reimbursement varies by payer (Medicare, Medicaid, private insurance). |
| Documentation Requirements | Requires detailed documentation of vaccine type, dosage, and administration route. |
| Frequency Limitations | Some codes have limitations on how often they can be billed per patient per day. |
| Updates and Changes | Codes and guidelines are periodically updated by the AMA and CMS. |
| Crosswalk with HCPCS | Some CPT codes may have corresponding HCPCS codes for Medicare billing. |
| Global Period | Typically, vaccine administration codes do not include a global period. |
| Place of Service | Applicable in various settings (e.g., office, clinic, pharmacy). |
| Patient Consent | Requires informed consent for vaccine administration. |
| Coding Hierarchy | Use the most specific code available for accurate billing. |
| Bundle Rules | Cannot be billed with certain evaluation and management (E/M) services without modifiers. |
Explore related products






What You'll Learn
![]()
Code Selection Based on Vaccine Type
Vaccine administration codes are not one-size-fits-all; they vary significantly based on the type of vaccine being administered. Each vaccine has unique characteristics, such as dosage, route of administration, and patient age requirements, which dictate the appropriate code selection. For instance, the administration code for a single-dose influenza vaccine differs from that of a multi-dose pneumococcal vaccine. Understanding these nuances is crucial for accurate billing and reimbursement, ensuring healthcare providers comply with payer guidelines and avoid claim denials.
Consider the COVID-19 vaccine, which has become a cornerstone of public health efforts. Administration codes for COVID-19 vaccines are tied to the specific product (e.g., Pfizer, Moderna, Johnson & Johnson) and the dosage series. For example, the initial dose of the Pfizer vaccine for individuals aged 12 and older is billed using a different code than the booster dose. Additionally, the administration of an additional dose for immunocompromised patients requires a distinct code, reflecting the complexity of vaccine protocols. This specificity ensures that billing accurately captures the clinical effort and resources involved.
Age-based variations further complicate code selection. Pediatric vaccines often require different administration codes than those for adults due to differences in dosage and formulation. For example, the administration of a diphtheria, tetanus, and acellular pertussis (DTaP) vaccine to a child under 7 years old uses a different code than the tetanus, diphtheria, and acellular pertussis (Tdap) vaccine given to adolescents and adults. Providers must carefully review vaccine-specific guidelines to select the correct code, as errors can lead to payment delays or audits.
Practical tips can streamline the coding process. First, always verify the vaccine’s product name and manufacturer, as these details influence code selection. Second, consult the Centers for Medicare & Medicaid Services (CMS) or the American Medical Association (AMA) for updated coding guidelines, as changes occur frequently. Third, document the vaccine administration process thoroughly, including the date, dosage, and patient age, to support code selection in case of disputes. By mastering these details, healthcare providers can navigate the complexities of vaccine administration codes with confidence.
Puppy Parvo Vaccination Schedule: Essential Steps for Optimal Protection
You may want to see also
Explore related products






![]()
Administration vs. Counseling Codes
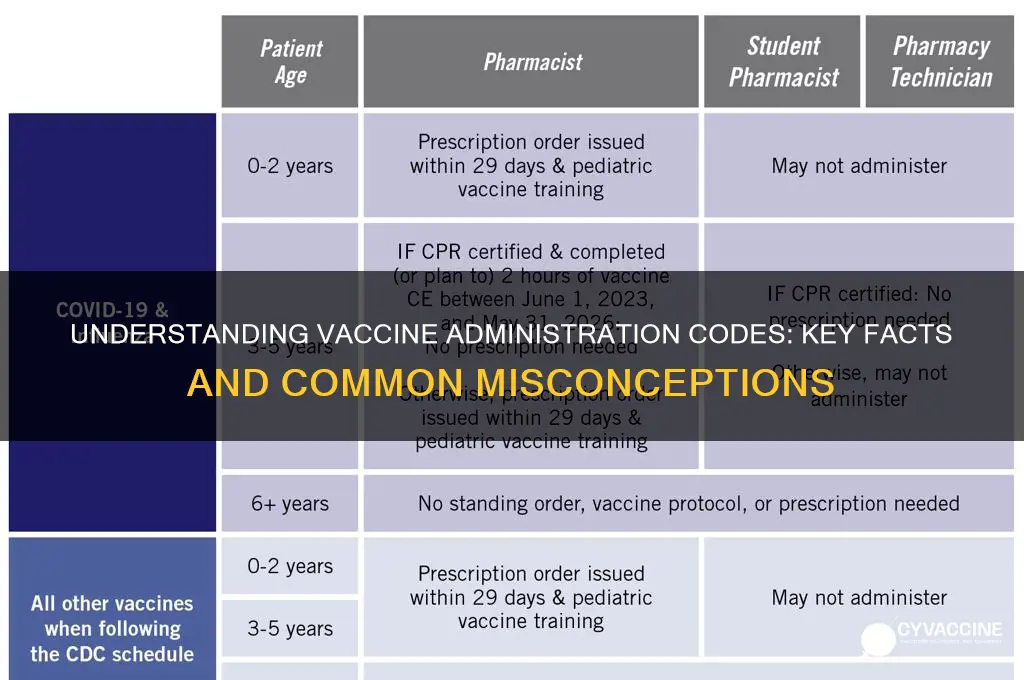
Vaccine administration codes and counseling codes serve distinct purposes in healthcare billing and patient care, yet their differences are often misunderstood. Administration codes, such as CPT 90460 or 90471, are used to bill for the physical act of administering a vaccine, including preparation, injection, and disposal of supplies. These codes are tied to specific vaccine types, routes (e.g., intramuscular, subcutaneous), and patient age groups. For instance, CPT 90460 covers the administration of immunizations like influenza for patients under 18, while 90471 is used for vaccines requiring significant counseling or preparation, such as HPV or COVID-19 vaccines. In contrast, counseling codes, like 99401-99404, are used for preventive medicine services, including discussions about vaccine benefits, risks, and scheduling. Understanding this distinction is critical to avoid billing errors, such as reporting counseling codes when only administration occurred.
Consider a scenario where a 12-year-old receives the first dose of the HPV vaccine. The provider uses CPT 90471 for administration, as this code accounts for the vaccine’s complexity and the need for detailed preparation. However, if the provider also spends 15–29 minutes counseling the patient and parent about the vaccine series, follow-up doses, and potential side effects, they could separately bill for this service using a counseling code like 99402. This dual billing is permissible because the services are distinct: one for the physical act of vaccination, the other for education and planning. Failure to differentiate these codes can result in claim denials or audits, as payers scrutinize improper bundling or unbundling of services.
A common pitfall is assuming that counseling inherently occurs during vaccine administration, justifying the use of higher-level codes. However, administration codes do not include time spent counseling unless explicitly stated. For example, CPT 90460 and 90471 focus solely on the act of administering the vaccine, not on discussions about its efficacy or side effects. Providers must document counseling separately, noting the duration and content of the discussion, to justify billing for preventive medicine services. This clarity ensures compliance with coding guidelines and maximizes reimbursement while maintaining transparency with payers.
Practical tips for accurate coding include verifying the patient’s age and vaccine type, as these factors determine the appropriate administration code. For instance, CPT 90460 is used for patients under 18, while 90461 applies to adults. Additionally, providers should document the route of administration (e.g., intramuscular for COVID-19 vaccines) and any unusual circumstances, such as managing anaphylaxis, which may require additional codes. When counseling occurs, use a stopwatch to track time spent discussing vaccine-related topics, ensuring the service meets the criteria for 99401-99404. Finally, educate staff on the differences between administration and counseling codes to streamline billing processes and reduce errors.
In summary, administration and counseling codes are separate entities in vaccine billing, each with specific criteria and purposes. Administration codes focus on the physical delivery of the vaccine, while counseling codes address patient education and preventive care planning. By understanding these distinctions and adhering to coding guidelines, providers can ensure accurate billing, avoid compliance issues, and deliver comprehensive care to patients. Mastery of these codes not only optimizes revenue but also reinforces the importance of clear documentation and ethical billing practices in healthcare.
MMR Vaccine and Autism: Separating Facts from Fiction
You may want to see also
Explore related products






![]()
Age-Specific Coding Guidelines
Vaccine administration codes are not one-size-fits-all; they vary significantly based on the patient’s age, which directly impacts dosage, route, and billing accuracy. For instance, the hepatitis B vaccine for newborns (aged 0–18 years) uses a different administration code than the adult formulation, even though the vaccine itself may be the same. This distinction ensures proper reimbursement and adherence to clinical guidelines, as pediatric doses often require smaller volumes and specialized techniques, such as intramuscular injection into the vastus lateralis muscle for infants.
Consider the influenza vaccine, where age-specific coding is critical due to varying formulations and routes. Children aged 6–35 months receive a 0.25 mL dose, while those aged 3 years and older get a 0.5 mL dose. Coders must select the appropriate administration code (e.g., CPT 90658 for preservative-free pediatric doses) to reflect these differences. Failure to do so can result in claim denials or underpayment, as payers scrutinize age-dose alignment to verify medical necessity and compliance with FDA-approved guidelines.
A persuasive argument for strict adherence to age-specific coding lies in the financial and clinical consequences of errors. For example, administering the wrong dose of the meningococcal vaccine to a teenager (e.g., using a pediatric code for a 16-year-old) not only risks improper billing but also compromises patient safety. Practices must train staff to cross-reference age, dose, and administration codes using resources like the CDC’s Vaccine Administration Codes table, which categorizes codes by age group and vaccine type.
Comparatively, age-specific coding for combination vaccines (e.g., DTaP-IPV-Hib) highlights the complexity of this system. A 2-month-old receiving a 0.5 mL dose requires a different administration code than a 4-year-old receiving a 0.5 mL booster, despite the volume being identical. This distinction arises from differences in vaccine composition and clinical indications, underscoring the need for coders to verify both age and vaccine product before assigning a code.
In practice, coders should adopt a systematic approach: first, confirm the patient’s age and vaccine type; second, consult age-specific dosage guidelines (e.g., ACIP recommendations); and third, match the administration code to the exact vaccine product and route. For example, the COVID-19 vaccine for children aged 6 months–5 years uses a lower dose (10 mcg) and a unique administration code compared to adolescents and adults (30 mcg). Tools like coding decision trees or software with built-in age-dose validators can minimize errors and streamline the process.
By mastering age-specific coding guidelines, healthcare providers ensure accurate billing, maximize reimbursement, and uphold patient safety—a trifecta of benefits that justify the attention to detail this task demands.
Leprosy: Exploring the Reality of Treatments and Potential Vaccines
You may want to see also
Explore related products






![]()
Handling Multiple Vaccines in One Visit
In the context of vaccine administration codes, handling multiple vaccines in one visit requires precision and adherence to coding guidelines to ensure accurate billing and optimal patient care. When administering multiple vaccines, each vaccine must be coded separately, reflecting the distinct preparation and administration processes involved. For instance, if a patient receives both the influenza vaccine (CPT code 90658) and the Tdap vaccine (CPT code 90715) during the same visit, two separate administration codes (e.g., 90460 and 90461) are required, along with the appropriate vaccine product codes. This granularity ensures that the complexity of the service is appropriately captured and reimbursed.
From a practical standpoint, administering multiple vaccines simultaneously demands careful planning to avoid errors. Vaccines should be administered at different anatomical sites to minimize discomfort and allow for clear documentation of any adverse reactions. For example, an intramuscular vaccine like Tdap might be given in the deltoid muscle, while a subcutaneous vaccine like the MMR (CPT code 90707) could be administered in the lateral thigh for infants or the upper arm for older children. Providers must also ensure that the vaccines are compatible for co-administration, as outlined in the CDC’s guidelines, to avoid potential interactions.
One critical aspect often overlooked is the dosage and age-specific considerations when handling multiple vaccines. For pediatric patients, combination vaccines like DTaP-IPV-Hib (CPT code 90700) can streamline administration by reducing the number of injections while still requiring a single administration code. However, for older adults receiving vaccines like pneumococcal conjugate (CPT code 90670) and zoster (CPT code 90681), providers must verify eligibility and dosing intervals, as these vaccines often have specific age or health status requirements. Missteps in these areas can lead to claim denials or suboptimal patient outcomes.
To navigate these complexities, providers should adopt a systematic approach. First, review the patient’s vaccination history and consult the latest ACIP guidelines to determine which vaccines are due. Second, prepare each vaccine separately, ensuring proper storage and handling conditions. Third, document each vaccine administration clearly in the medical record, noting the site, route, and time of administration. Finally, verify that the billing codes align with the services provided, using modifiers if necessary to indicate distinct procedures. For example, if a second nurse assists with simultaneous administrations, modifier -59 might be appended to indicate separate sessions.
In conclusion, handling multiple vaccines in one visit is a nuanced task that requires attention to detail, adherence to coding rules, and a patient-centered approach. By understanding the specific requirements for each vaccine, leveraging combination vaccines where appropriate, and maintaining meticulous documentation, providers can ensure efficient care delivery and accurate reimbursement. This not only optimizes practice workflows but also enhances patient satisfaction by minimizing the number of visits required to complete their vaccination schedule.
Coronavirus Vaccine: Protection Against All Strains?
You may want to see also
Explore related products






![]()
Billing for Booster or Additional Doses
A key factor in billing for boosters is verifying the patient’s eligibility based on time since the last dose and clinical guidelines. For example, COVID-19 boosters are typically administered at least 5 months after the initial series for Pfizer-BioNTech or Moderna vaccines, or 2 months after the single-dose Johnson & Johnson vaccine. Pediatric boosters may have different intervals, such as 3 months for children aged 5–11. Providers must document these details clearly to support the medical necessity of the booster dose, as payers often scrutinize these claims more closely than initial doses.
Another critical aspect is distinguishing between booster doses and additional primary doses, particularly for immunocompromised patients. For example, moderately to severely immunocompromised individuals may require a third dose of an mRNA COVID-19 vaccine as part of their primary series, followed by a booster dose later. The administration code for the additional primary dose differs from that of a booster, and incorrect coding can lead to reimbursement issues. Providers should consult the latest CDC and payer guidelines to ensure accurate billing for these scenarios.
Practical tips for seamless billing include training staff to verify patient history, including prior doses and dates, before administering boosters. Using electronic health records (EHR) with built-in vaccine tracking can streamline this process. Additionally, providers should stay updated on payer-specific policies, as some may require prior authorization for booster doses or have unique documentation requirements. Cross-referencing CPT codes with the vaccine product’s NDC (National Drug Code) is also essential to ensure alignment between the vaccine administered and the billed code.
In conclusion, billing for booster or additional doses demands attention to detail, from verifying eligibility to selecting the correct administration code. By staying informed about evolving guidelines and implementing robust documentation practices, providers can navigate this complex landscape effectively, ensuring proper reimbursement while delivering essential care to patients.
FDA's Role in Setting and Extending Vaccine Expiration Dates
You may want to see also
Frequently asked questions
This is false. Vaccine administration codes are used to bill for the service of administering the vaccine, not the vaccine product itself.
This is true. Vaccine administration codes differ depending on the route of administration, such as intramuscular, subcutaneous, or intranasal.
This is false. Vaccine administration codes do not include the cost of the vaccine; they only cover the service of administering it.
This is true. Vaccine administration codes are reported separately from the codes used to bill for the vaccine product itself.
This is false. Vaccine administration codes may vary based on factors such as patient age, complexity of administration, or additional services provided.