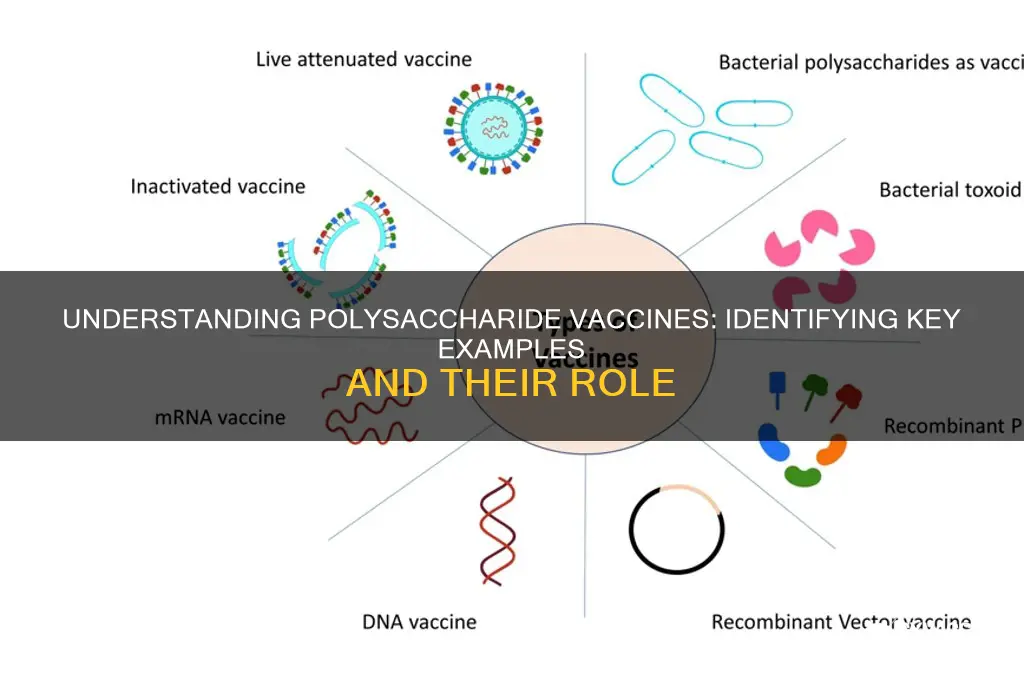
Polysaccharide vaccines are a type of vaccine that utilizes purified polysaccharides from the capsule of certain bacteria to induce an immune response. These vaccines are particularly effective against pathogens with a polysaccharide capsule, such as *Streptococcus pneumoniae*, *Neisseria meningitidis*, and *Haemophilus influenzae* type b. Unlike protein-based vaccines, polysaccharide vaccines primarily stimulate B cells to produce antibodies but do not generate immunological memory in young children, which limits their efficacy in certain age groups. To address this, conjugate vaccines, which link polysaccharides to carrier proteins, have been developed to enhance immune responses. When considering which of the following is a polysaccharide vaccine, it is essential to identify vaccines that contain only purified bacterial polysaccharides without conjugation to proteins.
Explore related products






What You'll Learn
![]()
Pneumococcal Conjugate Vaccine (PCV)
The administration of PCV follows a strict schedule tailored to age groups. For infants, the CDC recommends a 4-dose series at 2, 4, 6, and 12–15 months of age. Children aged 6–18 years with underlying medical conditions may receive a 2-dose series, while adults 65 and older typically receive a single dose of PCV20 or PCV15, followed by a dose of the pneumococcal polysaccharide vaccine (PPSV23) at least one year later. This tiered approach ensures maximum efficacy across different demographics, addressing the varying susceptibility to pneumococcal infections.
One of the most compelling aspects of PCV is its impact on global health. Since its introduction, PCV has significantly reduced the incidence of invasive pneumococcal diseases, particularly in children under 5, who are most vulnerable. Studies show a 50–70% reduction in pneumococcal pneumonia cases and a 60–90% decrease in pneumococcal meningitis following widespread vaccination campaigns. This success underscores the vaccine’s role as a cornerstone of preventive medicine, saving millions of lives annually.
Despite its efficacy, PCV is not without limitations. The vaccine covers only a subset of the 90+ pneumococcal serotypes, leaving room for non-vaccine serotypes to cause infections—a phenomenon known as serotype replacement. Additionally, while generally safe, mild side effects such as redness, swelling, or fever at the injection site are common. Rare but serious reactions, such as severe allergic responses, require immediate medical attention. Understanding these nuances is crucial for healthcare providers and caregivers to manage expectations and ensure proper use.
In conclusion, PCV exemplifies the evolution of polysaccharide vaccines, leveraging conjugation technology to provide robust, targeted immunity against pneumococcal diseases. Its age-specific dosing, global health impact, and ongoing challenges highlight its complexity and importance. For parents, healthcare workers, and policymakers, PCV remains a vital tool in the fight against preventable infections, offering a practical and effective means to protect vulnerable populations.
Delayed Baby Vaccination: Risks, Consequences, and What Parents Need to Know
You may want to see also
Explore related products






![]()
Haemophilus influenzae type b (Hib) Vaccine
The Haemophilus influenzae type b (Hib) vaccine stands out as a pivotal example of a polysaccharide-based vaccine, specifically a conjugate vaccine, designed to protect against a once-common bacterial infection. This vaccine targets *Haemophilus influenzae* type b, a bacterium that can cause severe diseases such as meningitis, pneumonia, and epiglottitis, particularly in young children. Unlike plain polysaccharide vaccines, the Hib vaccine combines the polysaccharide antigen from the bacterial capsule with a protein carrier, enhancing the immune response, especially in infants and young children whose immune systems are less mature.
From an analytical perspective, the development of the Hib conjugate vaccine marked a significant advancement in vaccinology. Before its introduction in the 1990s, Hib was the leading cause of bacterial meningitis in children under 5 years old, with approximately 20,000 cases annually in the United States alone. The vaccine’s efficacy lies in its ability to elicit a T-cell-dependent immune response, leading to the production of protective antibodies and immunological memory. This contrasts with plain polysaccharide vaccines, which are T-cell-independent and less effective in young children. The Hib vaccine’s success has led to a dramatic decline in Hib-related diseases, with a 99% reduction in cases in countries with widespread vaccination programs.
For parents and caregivers, understanding the Hib vaccine’s administration is crucial. The vaccine is typically given as part of routine childhood immunizations, starting at 2 months of age, with additional doses at 4 months and 6 months. A booster dose is often recommended between 12 and 15 months. The exact schedule may vary by country, so consulting local health guidelines is essential. The vaccine is safe and well-tolerated, with mild side effects such as redness at the injection site, fever, or irritability being rare. Ensuring timely vaccination is key, as delays can leave children vulnerable during the period when they are most at risk.
Comparatively, the Hib vaccine’s impact on global health underscores its importance as a polysaccharide-based vaccine. Unlike vaccines targeting viruses, such as the measles or polio vaccines, the Hib vaccine addresses a bacterial pathogen, demonstrating the versatility of polysaccharide conjugation technology. Its success has inspired the development of other conjugate vaccines, such as those for pneumococcal and meningococcal diseases. This highlights the broader implications of the Hib vaccine’s design, which has become a template for combating encapsulated bacterial pathogens.
In practical terms, the Hib vaccine’s role in preventing life-threatening diseases cannot be overstated. For travelers or families in regions with lower vaccination rates, ensuring Hib immunization is particularly important, as the bacterium can still circulate in unvaccinated populations. Additionally, maintaining a complete vaccination record is vital, as it ensures continuity of care and adherence to recommended schedules. The Hib vaccine is a testament to the power of scientific innovation in transforming public health, offering protection to millions of children worldwide and serving as a cornerstone of pediatric immunization programs.
Uploading Foreign Vaccination Certificates to MySejahtera: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Polysaccharide vs. Conjugate Vaccines
Polysaccharide vaccines, such as the pneumococcal polysaccharide vaccine (PPSV23), target specific bacterial infections by using purified capsular polysaccharides from the pathogen’s outer coating. These vaccines are effective in adults but have limitations in children under 2 years old because their immature immune systems cannot mount a robust response to T-cell-independent antigens. For instance, PPSV23 is recommended for adults 65 and older and high-risk individuals aged 2–64, with a single dose providing protection against 23 pneumococcal serotypes. However, its efficacy wanes over time, often requiring a booster dose after 5 years for those with specific medical conditions.
Conjugate vaccines, like the pneumococcal conjugate vaccine (PCV13 or PCV15), address the shortcomings of polysaccharide vaccines by chemically linking the polysaccharide antigens to a carrier protein. This conjugation enables T-cell-dependent immune responses, making these vaccines highly effective in infants and young children. PCV13, for example, is administered in a 4-dose series starting at 2 months of age, with doses given at 2, 4, 6, and 12–15 months. This schedule ensures long-lasting immunity and reduces the risk of invasive pneumococcal disease in vulnerable age groups. The success of conjugate vaccines has led to their widespread use in pediatric immunization programs globally.
A critical difference between the two lies in their immunological mechanisms. Polysaccharide vaccines rely on B-cell activation alone, producing short-lived antibodies without immune memory. Conjugate vaccines, however, stimulate both B-cells and T-cells, generating immunological memory and higher-affinity antibodies. This distinction explains why conjugate vaccines offer better protection in young children and why polysaccharide vaccines are reserved for older populations. For example, while PPSV23 is effective in preventing pneumococcal pneumonia in adults, PCV13 is the preferred choice for preventing otitis media and bacteremia in children.
Practically, healthcare providers must consider age, immune status, and comorbidities when choosing between these vaccines. For adults with conditions like asplenia or HIV, both PPSV23 and PCV13 are recommended in a sequential schedule, starting with PCV13 followed by PPSV23 at least 8 weeks later. In children, PCV13 is the standard, with PPSV23 reserved for those with high-risk conditions after age 2. Understanding these nuances ensures optimal protection against pneumococcal diseases across all age groups.
China's COVID-19 Recovery: Strategies Beyond Vaccines Unveiled
You may want to see also
Explore related products






![]()
Meningococcal Polysaccharide Vaccine (MPSV4)
The Meningococcal Polysaccharide Vaccine (MPSV4) is a critical tool in the fight against meningococcal disease, a severe bacterial infection that can lead to meningitis and sepsis. Unlike conjugate vaccines, MPSV4 contains purified polysaccharides from the outer capsules of four *Neisseria meningitidis* serogroups (A, C, Y, and W-135), stimulating the immune system to produce antibodies against these pathogens. This vaccine is particularly notable for its role in protecting older children, adolescents, and adults, as it is approved for individuals aged 56 years and older, filling a gap in meningococcal prevention strategies.
Administering MPSV4 involves a single 0.5 mL dose injected intramuscularly or subcutaneously, typically in the deltoid muscle for adults and the anterolateral thigh for younger recipients. While it offers rapid immunity, its efficacy wanes over time, necessitating booster doses every 3–5 years for those at continued risk, such as travelers to endemic areas or individuals with persistent immune deficiencies. Despite its utility, MPSV4 has limitations: it induces a T-cell-independent immune response, resulting in lower antibody production and no immune memory, particularly in young children under 2 years of age, for whom it is not recommended.
Comparatively, MPSV4 is often contrasted with meningococcal conjugate vaccines (MCV4), which are preferred for younger populations due to their ability to elicit a stronger, longer-lasting immune response and their efficacy in infants. However, MPSV4 remains a valuable option for older adults and specific at-risk groups, such as military personnel or laboratory workers, where rapid protection is needed. Its affordability and broader age approval also make it accessible in regions with limited healthcare resources.
Practical considerations for MPSV4 include monitoring for common side effects, such as pain at the injection site, headache, or mild fever, which typically resolve within a few days. It is crucial to avoid co-administration with other vaccines in the same syringe, as this can reduce immunogenicity. For travelers, scheduling vaccination at least 1–2 weeks before departure ensures adequate immune response. While MPSV4 is not a one-size-fits-all solution, its targeted application underscores its importance in a comprehensive meningococcal prevention strategy.
Monoclonal Antibodies vs. Vaccines: Understanding the Key Differences
You may want to see also
Explore related products


![]()
Immune Response to Polysaccharide Antigens
Polysaccharide antigens, derived from the cell walls of bacteria, elicit a unique immune response that differs significantly from protein-based antigens. Unlike proteins, polysaccharides are T-cell independent antigens, meaning they do not require processing by antigen-presenting cells (APCs) or T-cell help to stimulate B-cell activation. This characteristic makes them both a challenge and an opportunity in vaccine development. For instance, vaccines like the pneumococcal polysaccharide vaccine (PPSV23) directly activate B cells, leading to the production of antibodies. However, this response is often short-lived and less effective in infants and young children, whose immune systems are still maturing.
The immune response to polysaccharide antigens is primarily mediated by B-2 cells, which produce IgM antibodies. These antibodies are effective at opsonization and complement activation, critical for clearing encapsulated bacteria like *Streptococcus pneumoniae* and *Neisseria meningitidis*. However, the response lacks immunological memory and isotype switching to IgG, which limits long-term protection. This limitation is particularly evident in children under two years of age, whose immune systems are less capable of responding to T-cell independent antigens. To address this, conjugate vaccines, such as the pneumococcal conjugate vaccine (PCV13), link polysaccharides to carrier proteins, converting them into T-cell dependent antigens. This modification enhances the immune response by enabling class switching, affinity maturation, and the development of memory B cells.
One practical consideration in polysaccharide vaccine administration is the dosage and schedule. For example, PPSV23 is typically administered as a single 0.5 mL dose in adults, while PCV13 requires a series of doses (e.g., 2, 4, 6, and 12–15 months) in infants. The choice between these vaccines depends on age, immune status, and risk factors. For instance, PPSV23 is recommended for adults over 65 and immunocompromised individuals, whereas PCV13 is preferred for children and younger adults due to its ability to induce a more robust and durable immune response.
A critical takeaway is that while polysaccharide antigens are effective in eliciting an immediate immune response, their limitations necessitate innovative approaches like conjugation. Understanding these nuances is essential for healthcare providers when selecting the appropriate vaccine for different populations. For example, travelers to regions with high rates of meningococcal disease may benefit from a meningococcal conjugate vaccine (MenACWY), which provides broader and longer-lasting protection compared to its polysaccharide counterpart. By tailoring vaccine selection to the individual’s immune capabilities and risk profile, clinicians can optimize protection against polysaccharide-encapsulated pathogens.
Exploring HSV-1 and HSV-2: Current Vaccine Development and Hope
You may want to see also
Frequently asked questions
The Pneumococcal conjugate vaccine is a polysaccharide vaccine.
A polysaccharide vaccine is made from the polysaccharide (sugar) components of bacterial cell walls, which stimulate an immune response.
No, the HPV vaccine is not a polysaccharide vaccine; it is a recombinant protein vaccine.
Neither; however, some meningococcal vaccines (e.g., MenACWY) use polysaccharides or conjugated polysaccharides.
Yes, conjugate vaccines combine polysaccharides with carrier proteins to enhance the immune response, making them polysaccharide-based vaccines.