Vaccines are essential tools in preventing infectious diseases by stimulating the immune system to recognize and combat pathogens. Among the various types of vaccines, basic categories include live-attenuated vaccines, inactivated vaccines, subunit, recombinant, polysaccharide, and conjugate vaccines, as well as mRNA and viral vector vaccines. Each type operates differently, utilizing either weakened or killed pathogens, specific components of the pathogen, or genetic material to elicit an immune response. Understanding these distinctions is crucial for determining which of the following options qualifies as a basic type of vaccine, as it directly impacts efficacy, safety, and appropriate use in different populations.
Explore related products






What You'll Learn
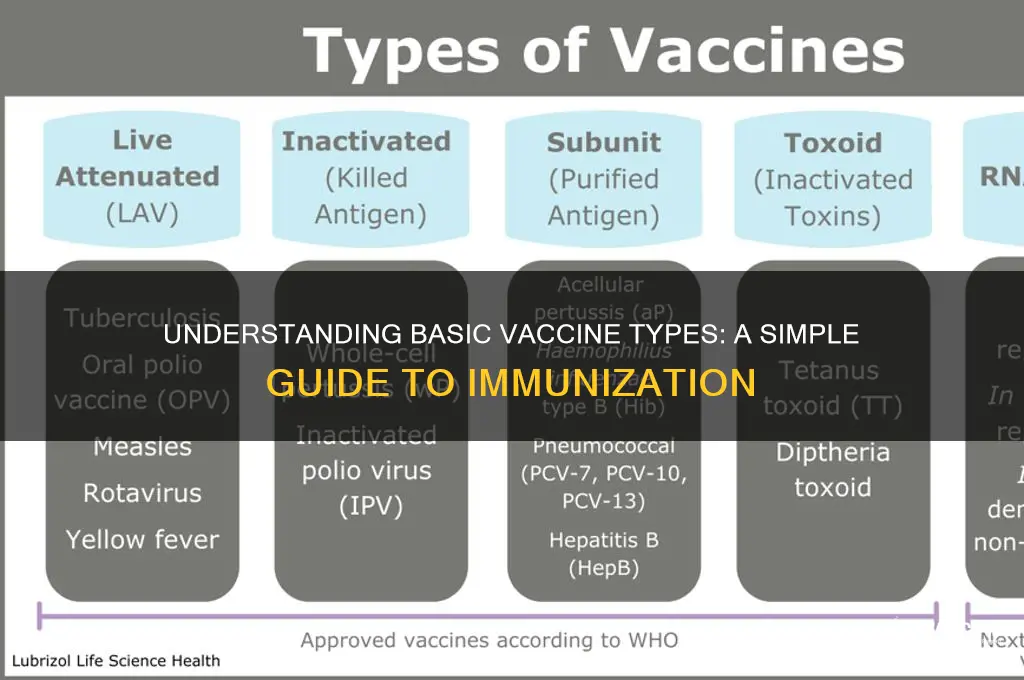
- Live-attenuated vaccines: Weakened viruses/bacteria that still replicate, triggering a strong immune response
- Inactivated vaccines: Killed pathogens that cannot replicate but stimulate immune memory
- Subunit vaccines: Contain specific antigens (proteins/sugars) from the pathogen, not the whole organism
- Toxoid vaccines: Inactivated toxins produced by bacteria, preventing harmful effects
- mRNA vaccines: Use genetic material to instruct cells to produce pathogen proteins, triggering immunity
![]()
Live-attenuated vaccines: Weakened viruses/bacteria that still replicate, triggering a strong immune response
Live-attenuated vaccines represent a cornerstone of modern immunology, leveraging weakened pathogens to stimulate robust immunity without causing disease. Unlike inactivated vaccines, which use killed pathogens, live-attenuated vaccines contain viruses or bacteria that have been modified to replicate at a reduced rate. This replication mimics a natural infection, prompting the immune system to mount a vigorous response, including the production of memory cells for long-term protection. Examples include the measles, mumps, and rubella (MMR) vaccine and the oral polio vaccine (OPV), both of which have dramatically reduced the global burden of these diseases.
Administering live-attenuated vaccines requires careful consideration of dosage and timing. For instance, the MMR vaccine is typically given in two doses: the first at 12–15 months of age and the second at 4–6 years. The oral polio vaccine, delivered as drops, is administered in multiple doses starting at 6 weeks of age in regions where polio remains endemic. These vaccines are highly effective, often conferring lifelong immunity after a complete series. However, their live nature necessitates precautions; they are generally contraindicated in immunocompromised individuals, as the weakened pathogens could potentially cause severe illness in those with weakened immune systems.
One of the key advantages of live-attenuated vaccines is their ability to induce mucosal immunity, a critical defense mechanism at the body’s entry points, such as the respiratory and gastrointestinal tracts. This is particularly important for pathogens like influenza and rotavirus, which infect through these routes. For example, the live-attenuated influenza vaccine (LAIV), administered as a nasal spray, directly targets the mucosal lining of the nose, providing localized immunity. This contrasts with injected vaccines, which primarily stimulate systemic immunity. However, LAIV is not recommended for individuals with certain chronic conditions or pregnant women, highlighting the need for tailored vaccination strategies.
Despite their efficacy, live-attenuated vaccines are not without challenges. Their requirement for refrigeration (the "cold chain") and potential for reversion to virulence—though rare—pose logistical and safety concerns. For instance, the oral polio vaccine, while highly effective, has, in extremely rare cases, caused vaccine-derived poliovirus in underimmunized populations. Such risks underscore the importance of high vaccination coverage to prevent circulation of the attenuated virus. Nonetheless, the benefits of live-attenuated vaccines far outweigh these risks, particularly in preventing diseases with high morbidity and mortality rates.
In practical terms, individuals receiving live-attenuated vaccines should avoid close contact with severely immunocompromised persons for a short period post-vaccination, as the shedding of the attenuated virus is possible. Additionally, these vaccines should be spaced at least 4 weeks apart if not administered simultaneously, to ensure optimal immune response. For travelers to regions with vaccine-preventable diseases, live-attenuated vaccines like yellow fever offer durable protection but require careful planning due to their specific administration guidelines. By understanding these nuances, healthcare providers and recipients can maximize the benefits of live-attenuated vaccines while minimizing risks.
The Invention of Feline Calicivirus Vaccine: A Historical Overview
You may want to see also
Explore related products






![]()
Inactivated vaccines: Killed pathogens that cannot replicate but stimulate immune memory
Inactivated vaccines represent a cornerstone of modern immunization strategies, leveraging the immune system’s ability to recognize and remember pathogens without the risk of active infection. Unlike live-attenuated vaccines, which use weakened but still viable pathogens, inactivated vaccines contain pathogens that have been killed through physical or chemical methods, such as heat or formaldehyde. This process renders the pathogen incapable of replicating within the body, eliminating the possibility of causing disease, even in immunocompromised individuals. The immune system, however, still identifies the pathogen’s structural components, triggering the production of antibodies and the formation of immune memory. This dual benefit—safety and efficacy—makes inactivated vaccines particularly valuable for populations at higher risk, including the elderly, pregnant individuals, and those with chronic illnesses.
Consider the influenza vaccine, one of the most widely administered inactivated vaccines globally. Each year, the World Health Organization selects strains of the influenza virus most likely to circulate, and these are grown in eggs or cell cultures, harvested, and inactivated. The resulting vaccine is typically administered as a single 0.5 mL dose for adults and children over 3 years old, with a lower dose for younger children. While inactivated vaccines often require multiple doses or booster shots to achieve robust immunity—due to their inability to replicate and provide prolonged antigen exposure—their safety profile makes them a preferred choice for routine immunization programs. For instance, the hepatitis A vaccine, another inactivated vaccine, is given in two doses, six months apart, providing long-term protection against the virus.
One of the key advantages of inactivated vaccines is their stability and ease of storage compared to live vaccines, which often require refrigeration. This makes them particularly suitable for use in resource-limited settings or during mass vaccination campaigns. However, their inability to replicate means they may not elicit as strong a mucosal or cell-mediated immune response as live vaccines. To compensate, adjuvants—substances like aluminum salts—are often added to enhance the immune response. For example, the inactivated polio vaccine (IPV) contains an adjuvant to boost its effectiveness, ensuring protection against all three poliovirus strains with minimal side effects, such as soreness at the injection site.
Despite their safety, inactivated vaccines are not without limitations. Their production process, which involves growing and inactivating pathogens, can be time-consuming and costly, potentially limiting their availability during outbreaks. Additionally, the immune response they generate may wane over time, necessitating periodic boosters. For instance, the tetanus vaccine, an inactivated toxoid, requires booster doses every 10 years to maintain immunity. Nevertheless, their proven track record in preventing diseases like rabies, cholera, and pertussis underscores their importance in global health.
In practice, inactivated vaccines offer a reliable and safe option for individuals across all age groups, particularly those with compromised immune systems. For parents, understanding that these vaccines cannot cause the disease they prevent can alleviate concerns about vaccination. Healthcare providers should emphasize the importance of completing the full vaccine series to ensure optimal protection. For travelers to regions with high disease prevalence, inactivated vaccines like those for typhoid or Japanese encephalitis can be lifesaving. By combining safety with efficacy, inactivated vaccines remain a vital tool in the fight against infectious diseases, demonstrating the power of harnessing the immune system’s memory without risking active infection.
Step-by-Step Guide to Registering for Your Vaccine at Ford Field
You may want to see also
Explore related products

$23.58 $32.99





![]()
Subunit vaccines: Contain specific antigens (proteins/sugars) from the pathogen, not the whole organism
Subunit vaccines represent a precision-focused approach in immunology, isolating and delivering only the essential components of a pathogen to stimulate an immune response. Unlike whole-cell or live-attenuated vaccines, which use the entire organism, subunit vaccines contain specific antigens—proteins or sugars—that are critical to the pathogen’s structure or function. This targeted strategy minimizes the risk of adverse reactions while maximizing efficacy, making subunit vaccines a cornerstone of modern vaccination efforts.
Consider the hepatitis B vaccine, a classic example of a subunit vaccine. It contains only the hepatitis B surface antigen (HBsAg), a protein derived from the virus’s outer envelope. Administered in a series of three doses (typically at 0, 1, and 6 months), this vaccine triggers the production of antibodies that neutralize the virus, providing long-term immunity. Its safety profile is particularly notable: it is approved for all age groups, from infants to the elderly, and is free from the risk of causing the disease it prevents. This specificity underscores the subunit vaccine’s ability to protect without overwhelming the immune system.
The development of subunit vaccines involves meticulous identification and extraction of key antigens, often aided by recombinant DNA technology. For instance, the human papillomavirus (HPV) vaccine uses virus-like particles (VLPs) composed of the L1 protein, which self-assembles into structures mimicking the virus but lacks its genetic material. This design ensures the vaccine cannot cause infection while effectively priming the immune system. Such advancements highlight the role of biotechnology in refining vaccine safety and efficacy.
One of the most compelling advantages of subunit vaccines is their suitability for vulnerable populations, including immunocompromised individuals and pregnant women. Because they do not contain live or even inactivated pathogens, the risk of vaccine-induced illness is virtually eliminated. For example, the acellular pertussis vaccine (part of the DTaP series) uses purified antigens like pertussis toxin and filamentous hemagglutinin, offering protection against whooping cough without the side effects associated with the older whole-cell vaccine. This makes subunit vaccines a preferred choice in scenarios where safety is paramount.
Despite their benefits, subunit vaccines are not without challenges. Their highly specific nature often requires the inclusion of adjuvants—substances like aluminum salts—to enhance the immune response. Additionally, multiple doses may be necessary to achieve robust immunity, as seen with the HPV and hepatitis B vaccines. However, these considerations are outweighed by the vaccines’ safety and efficacy, particularly in preventing diseases with severe outcomes. As research progresses, subunit vaccines continue to evolve, offering a blueprint for next-generation immunizations tailored to the complexities of modern health threats.
Discover Your Vaccination Records: A Step-by-Step Guide to Your Immunization History
You may want to see also
Explore related products


$63.74 $84.99




![]()
Toxoid vaccines: Inactivated toxins produced by bacteria, preventing harmful effects
Toxoid vaccines represent a unique approach to immunization, targeting the harmful toxins produced by certain bacteria rather than the bacteria themselves. These vaccines contain inactivated toxins, known as toxoids, which are rendered harmless but still capable of eliciting a protective immune response. This strategy is particularly effective against diseases where bacterial toxins are the primary cause of illness, such as tetanus and diphtheria. By neutralizing the toxins, toxoid vaccines prevent the severe symptoms associated with these infections, offering long-term immunity with minimal risk.
Consider the tetanus toxoid vaccine, a cornerstone of preventive medicine. Tetanus, caused by the bacterium *Clostridium tetani*, produces a potent toxin that leads to muscle stiffness and spasms, often fatal without treatment. The vaccine typically requires an initial series of three doses, administered over several weeks, followed by booster shots every 10 years. This regimen ensures sustained immunity, particularly crucial for individuals at higher risk of exposure, such as gardeners, construction workers, or those traveling to areas with poor sanitation. The vaccine’s safety profile is well-established, with mild side effects like soreness at the injection site being the most common.
In contrast to live or attenuated vaccines, toxoid vaccines are entirely non-infectious, making them suitable for individuals with compromised immune systems. This characteristic also eliminates the risk of the vaccine causing the disease it aims to prevent, a rare but possible outcome with live vaccines. However, toxoid vaccines often require adjuvants—substances added to enhance the immune response—since the inactivated toxins alone may not stimulate sufficient immunity. Aluminum salts are commonly used adjuvants in toxoid vaccines, ensuring a robust and durable immune reaction.
Practical considerations for toxoid vaccines include their storage and administration. Unlike some vaccines requiring strict cold chain maintenance, toxoid vaccines are relatively stable, making them accessible in resource-limited settings. For parents and caregivers, ensuring children receive the diphtheria-tetanus-pertussis (DTaP) vaccine series on schedule is critical. The first dose is typically given at 2 months of age, followed by additional doses at 4 months, 6 months, 15–18 months, and 4–6 years. Adolescents and adults should receive the Tdap booster to maintain protection against tetanus, diphtheria, and pertussis.
In summary, toxoid vaccines exemplify the precision of modern immunology, targeting specific bacterial toxins to prevent disease. Their safety, efficacy, and accessibility make them indispensable tools in public health. Whether protecting against tetanus in a construction worker or diphtheria in a schoolchild, these vaccines demonstrate the power of tailoring immunization strategies to the unique mechanisms of infection. By understanding their role and following recommended schedules, individuals can maximize the benefits of toxoid vaccines, contributing to both personal and community health.
CVS Vaccine Appointments: When and How to Secure Your Slot
You may want to see also
Explore related products






![]()
mRNA vaccines: Use genetic material to instruct cells to produce pathogen proteins, triggering immunity
MRNA vaccines represent a groundbreaking approach in immunology, leveraging the body's own cellular machinery to mount a defense against pathogens. Unlike traditional vaccines that introduce a weakened or inactivated pathogen, mRNA vaccines deliver a genetic blueprint—a strand of messenger RNA (mRNA)—that instructs cells to produce a specific protein found on the pathogen’s surface. This protein triggers an immune response, preparing the body to recognize and combat the actual pathogen if exposed later. The Pfizer-BioNTech and Moderna COVID-19 vaccines are prime examples, demonstrating both the efficacy and rapid development potential of this technology.
The process begins with a precisely engineered mRNA sequence, encapsulated in lipid nanoparticles to protect it from degradation and facilitate entry into cells. Once inside, the mRNA is translated by ribosomes into the target protein, typically a viral spike protein. This protein is then displayed on the cell surface, where immune cells detect it as foreign, prompting the production of antibodies and activation of T-cells. Notably, the mRNA does not alter the recipient’s DNA, as it operates solely in the cytoplasm and degrades quickly after fulfilling its role. This mechanism ensures both safety and specificity in immune training.
One of the most compelling advantages of mRNA vaccines is their versatility and speed of development. Traditional vaccines often require years to produce, as they involve culturing pathogens or developing attenuated strains. In contrast, mRNA vaccines can be designed and manufactured within weeks once the genetic sequence of a pathogen is known. During the COVID-19 pandemic, this capability proved invaluable, enabling the deployment of vaccines in record time. Additionally, mRNA technology can be adapted to target a wide range of diseases, from influenza to cancer, making it a cornerstone of future vaccine development.
Practical considerations for mRNA vaccines include storage and administration. The Pfizer-BioNTech vaccine, for instance, requires ultra-cold storage at -70°C, while Moderna’s can be stored at -20°C, easing distribution challenges. Both vaccines are administered in two doses, typically 3–4 weeks apart, with a booster recommended for prolonged immunity. Side effects are generally mild to moderate, including pain at the injection site, fatigue, and fever, resolving within a few days. These vaccines are approved for individuals aged 5 and older, with dosage adjustments for younger age groups.
In conclusion, mRNA vaccines exemplify the fusion of molecular biology and immunology, offering a dynamic and efficient method to induce immunity. Their ability to rapidly respond to emerging pathogens, coupled with their safety profile, positions them as a transformative tool in global health. As research advances, mRNA technology is poised to address not only infectious diseases but also chronic conditions, underscoring its potential as a basic yet revolutionary type of vaccine.
Could a Hidden Cure: Existing Treatments as Potential Coronavirus Vaccines?
You may want to see also
Frequently asked questions
Live-attenuated vaccines are a basic type of vaccine, as they use a weakened form of the live virus or bacteria to stimulate immunity.
Inactivated vaccines are a basic type of vaccine, as they use a killed version of the germ to trigger an immune response.
Live-attenuated vaccines are a basic type of vaccine, as they use a weakened form of the live pathogen to induce immunity.