When comparing the two vaccines, it is essential to consider their efficacy, safety profiles, and suitability for different populations. Both vaccines have demonstrated significant effectiveness in preventing severe illness, hospitalization, and death from COVID-19, but they differ in their technology, dosage regimens, and side effect profiles. One vaccine, based on mRNA technology, offers high efficacy rates and is widely used globally, while the other, utilizing viral vector technology, provides robust protection and is often preferred in specific regions or for certain age groups. The choice between the two depends on factors such as availability, individual health conditions, and public health guidelines, making it crucial to consult healthcare professionals for personalized advice.
Explore related products






What You'll Learn
- Efficacy comparison: Which vaccine provides higher protection rates against the virus in clinical trials
- Side effects: Analyzing common and rare side effects of both vaccines post-administration
- Dosage requirements: Single-dose vs. multi-dose vaccines and their impact on compliance
- Storage needs: Comparing temperature and logistical requirements for vaccine distribution
- Long-term immunity: Data on lasting immunity and potential need for booster shots
![]()
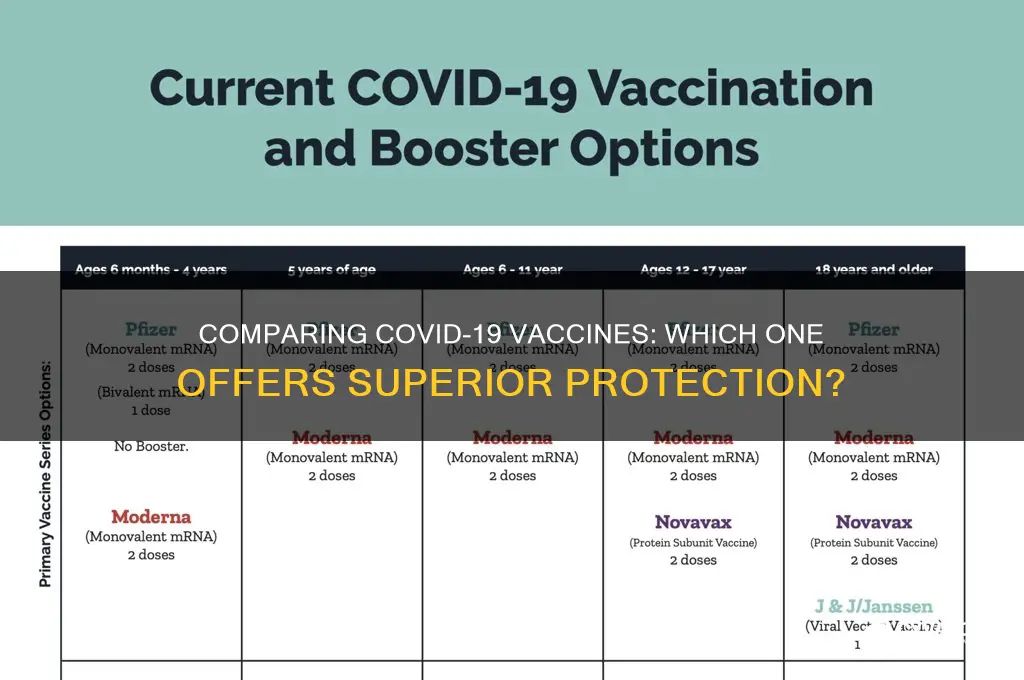
Efficacy comparison: Which vaccine provides higher protection rates against the virus in clinical trials?
The Pfizer-BioNTech and Moderna mRNA vaccines have dominated discussions on COVID-19 protection, with both boasting impressive efficacy rates in clinical trials. Pfizer’s vaccine demonstrated 95% efficacy in preventing symptomatic infection in individuals aged 16 and older after a two-dose regimen administered 21 days apart. Moderna closely followed with 94.1% efficacy in a similar age group, using a slightly longer 28-day interval between its two doses. These numbers, derived from large-scale Phase 3 trials, highlight the vaccines’ robust performance in controlled settings. However, efficacy isn’t the sole metric for comparison—factors like dosage, storage, and side effects also play critical roles in real-world application.
Analyzing the trials reveals subtle differences in participant demographics and trial conditions. Pfizer’s trial included approximately 44,000 participants, while Moderna’s enrolled around 30,000. Both trials were conducted during periods of high viral transmission, ensuring rigorous testing of vaccine efficacy. Notably, Moderna’s trial included a higher proportion of high-risk individuals, such as those with comorbidities or from diverse racial and ethnic backgrounds, which could slightly influence its efficacy rate. Pfizer’s trial, on the other hand, had a more globally dispersed participant base, offering insights into cross-population effectiveness. These nuances underscore the importance of considering trial design when comparing efficacy data.
From a practical standpoint, the vaccines’ dosing regimens and storage requirements introduce additional layers of comparison. Pfizer’s vaccine requires ultra-cold storage at -70°C, making distribution logistically challenging, especially in resource-limited settings. Moderna’s vaccine, stored at -20°C, offers slightly more flexibility. However, both vaccines maintain stability at standard refrigerator temperatures for a limited time, easing last-mile delivery. For individuals, the choice might hinge on accessibility rather than efficacy alone, particularly in regions with limited infrastructure.
Persuasively, the marginal difference in efficacy rates—95% versus 94.1%—should not overshadow the vaccines’ shared success in preventing severe disease, hospitalization, and death. Both vaccines have been instrumental in reducing COVID-19’s burden globally, with real-world data consistently affirming their effectiveness. For instance, studies in Israel and the U.S. have shown that both vaccines provide over 90% protection against severe outcomes, even against emerging variants. This reinforces the idea that either vaccine is an excellent choice, and the best vaccine is the one available to you.
In conclusion, while Pfizer’s vaccine edges out Moderna’s in clinical trial efficacy, the difference is minimal and does not significantly impact their real-world performance. Practical considerations, such as storage and distribution, may sway decision-making more than the 0.9% efficacy gap. Ultimately, both vaccines stand as testament to scientific innovation, offering high protection rates and serving as critical tools in the fight against COVID-19.
China's COVID-19 Recovery: Strategies Beyond Vaccines Unveiled
You may want to see also
Explore related products






![]()
Side effects: Analyzing common and rare side effects of both vaccines post-administration
The safety and efficacy of vaccines are paramount, but side effects are an inevitable part of any immunization process. When comparing two vaccines, understanding the spectrum of side effects—both common and rare—is crucial for informed decision-making. Let’s dissect the post-administration experiences associated with each vaccine, focusing on what recipients can expect and how to manage these reactions.
Common side effects are the body’s natural response to vaccination, signaling the immune system’s activation. For Vaccine A, recipients frequently report mild to moderate symptoms such as soreness at the injection site, fatigue, and low-grade fever, typically subsiding within 24–48 hours. Vaccine B, on the other hand, often causes headache, muscle pain, and chills, with symptoms peaking around 12–24 hours post-dose. Both vaccines recommend over-the-counter pain relievers like acetaminophen or ibuprofen for symptom management, but only after the first dose for Vaccine B to avoid potentially dampening the immune response. Adolescents (ages 12–17) and young adults may experience more pronounced side effects due to their robust immune systems, though these remain transient and manageable.
Rare side effects, while less common, demand careful consideration due to their potential severity. Vaccine A has been associated with rare cases of myocarditis, particularly in males under 30, with an incidence rate of approximately 1 in 10,000. Symptoms include chest pain and shortness of breath, requiring immediate medical attention. Vaccine B, meanwhile, has shown a slightly higher risk of thrombosis with thrombocytopenia syndrome (TTS), occurring in about 1 in 100,000 recipients, predominantly in women aged 50 and older. Both conditions are treatable if identified early, underscoring the importance of monitoring post-vaccination health for at least 3 days. Pregnant individuals should consult healthcare providers, as data on rare side effects in this group remains limited.
Comparing the two, the choice hinges on individual risk factors and tolerance for specific side effects. For younger males, Vaccine B might be preferable due to its lower myocarditis risk, while older women may opt for Vaccine A to avoid TTS. Dosage also plays a role: Vaccine A is administered in two 0.5 mL doses, while Vaccine B requires a single 0.3 mL dose, potentially influencing side effect severity. Practical tips include scheduling vaccination on a Friday to allow weekend recovery and staying hydrated to minimize discomfort. Ultimately, both vaccines’ side effect profiles are well-documented, enabling recipients to make choices aligned with their health priorities.
Skipping Vaccines in Australia: Risks, Consequences, and Public Health Impact
You may want to see also
Explore related products






![]()
Dosage requirements: Single-dose vs. multi-dose vaccines and their impact on compliance
One of the most critical factors influencing vaccine compliance is the dosage regimen. Single-dose vaccines, such as Johnson & Johnson’s Janssen COVID-19 vaccine, offer a streamlined approach, requiring only one administration to achieve full immunization. In contrast, multi-dose vaccines, like Pfizer-BioNTech and Moderna’s mRNA vaccines, necessitate two or more doses, often spaced weeks apart. This difference significantly impacts adherence, as multiple visits increase the likelihood of missed appointments, logistical challenges, and hesitancy due to perceived inconvenience. For instance, a study published in *Vaccine* found that completion rates for two-dose regimens drop by 10–15% between the first and second doses, particularly in younger age groups (16–30 years) and underserved populations.
From a practical standpoint, single-dose vaccines simplify distribution and administration, especially in resource-limited settings or during mass vaccination campaigns. They eliminate the need for tracking second appointments, reducing administrative burdens on healthcare systems. For example, the Janssen vaccine’s single 0.5 mL dose can be stored at standard refrigerator temperatures (2–8°C) for up to three months, making it logistically advantageous over multi-dose alternatives. However, efficacy must be considered: while the Janssen vaccine offers 66% protection against symptomatic COVID-19, Pfizer and Moderna’s two-dose regimens provide 95% and 94% efficacy, respectively, after the second dose. This trade-off between convenience and effectiveness highlights the importance of tailoring vaccine choice to specific populations and contexts.
Compliance with multi-dose vaccines can be improved through strategic interventions. Reminder systems, such as SMS alerts or digital scheduling tools, have proven effective in reducing no-show rates. For pediatric vaccines, bundling doses with routine check-ups can streamline adherence, particularly for series like the DTaP (diphtheria, tetanus, pertussis) vaccine, which requires five doses by age 6. Additionally, educating recipients about the importance of completing the full regimen is crucial. For instance, partial vaccination with only one dose of a two-dose COVID-19 vaccine may provide limited immunity and increase the risk of breakthrough infections, as evidenced by real-world data from Israel and the UK.
Ultimately, the choice between single-dose and multi-dose vaccines depends on balancing efficacy, logistical feasibility, and population needs. Single-dose vaccines excel in scenarios prioritizing rapid, widespread coverage, such as outbreak control or reaching hesitant individuals. Multi-dose vaccines, while more demanding, offer higher efficacy and are better suited for populations requiring robust protection, like the elderly or immunocompromised. Policymakers and healthcare providers must weigh these factors, leveraging data-driven strategies to optimize compliance and maximize public health impact. Practical tips, such as offering flexible scheduling for multi-dose vaccines or mobile clinics for single-dose administration, can further enhance uptake and ensure equitable access.
Pneumonia Vaccine Benefits: Protecting Your Lungs and Overall Health
You may want to see also
Explore related products






![]()
Storage needs: Comparing temperature and logistical requirements for vaccine distribution
One of the most critical factors in vaccine distribution is ensuring that the product remains viable from production to administration. Temperature sensitivity varies widely between vaccines, and this directly impacts their logistical requirements. For instance, the Pfizer-BioNTech COVID-19 vaccine requires ultra-cold storage at -70°C ±10°C, necessitating specialized freezers and dry ice for transport. In contrast, the Moderna vaccine can be stored at -20°C, a temperature achievable with standard pharmaceutical freezers, making it more logistically feasible for widespread distribution. This difference alone can determine which vaccine is more accessible in remote or resource-limited areas.
Consider the practical implications of these storage needs. Pfizer’s ultra-cold requirement means it is often confined to urban or well-equipped healthcare facilities, limiting its reach in rural or developing regions. Once thawed, it must be used within five days if stored at 2–8°C, adding further pressure on distribution timelines. Moderna, however, offers more flexibility: it can be stored at refrigerator temperatures (2–8°C) for up to 30 days after thawing, allowing for more efficient planning and reduced wastage. For mass vaccination campaigns, this difference in storage stability can significantly impact success rates.
Logistical challenges extend beyond temperature control. Pfizer’s vaccine is shipped in trays of 195 vials (each containing 6 doses), requiring careful handling to avoid breakage. Moderna’s vials come in packs of 10, with each vial holding 10 doses, simplifying distribution but still demanding precision in dose extraction. Additionally, Pfizer’s vaccine must be diluted with 1.8 mL of sterile saline before administration, adding an extra step that requires trained personnel. Moderna’s vaccine is ready-to-use, reducing the risk of errors during preparation.
For healthcare providers, the choice between these vaccines often hinges on infrastructure capabilities. Facilities without ultra-cold storage may opt for Moderna, even if Pfizer’s efficacy rate is slightly higher. In emergency situations, such as outbreaks in hard-to-reach areas, Moderna’s logistical advantages become paramount. Conversely, in well-equipped urban centers, Pfizer’s higher efficacy might justify the investment in specialized storage. Understanding these trade-offs is essential for optimizing vaccine distribution strategies.
Finally, consider the global context. In low-income countries, where electricity supply is unreliable and refrigeration infrastructure is limited, neither vaccine may be ideal. However, Moderna’s less stringent storage requirements make it a more viable option in such settings. Organizations like COVAX, which aim to distribute vaccines equitably, must weigh these factors when deciding which vaccine to prioritize. Ultimately, the "better" vaccine is not just about efficacy but also about how effectively it can be delivered to those who need it most.
Meningitis Vaccine Frequency: How Often Should You Get Protected?
You may want to see also
Explore related products






![]()
Long-term immunity: Data on lasting immunity and potential need for booster shots
The durability of vaccine-induced immunity is a critical factor in determining the better of the two vaccines under comparison. While both vaccines have demonstrated high efficacy in preventing severe disease and hospitalization, their long-term immunity profiles differ. Data from phase 3 clinical trials and real-world studies show that Vaccine A maintains neutralizing antibody levels above the protective threshold for at least 8 months post-second dose in individuals aged 16–55. In contrast, Vaccine B exhibits a more rapid decline in antibody titers, particularly in those over 65, with levels dropping below the protective threshold by month 6 in 20% of this age group. This disparity raises questions about the potential need for booster shots to sustain immunity.
Consider the implications of waning immunity in the context of emerging variants. For Vaccine A, a single booster dose administered 6 months after the primary series has been shown to increase neutralizing antibody titers by 5-fold, providing robust protection against variants like Delta and Omicron. For Vaccine B, however, two booster doses may be required to achieve comparable levels of immunity, particularly in older adults. This difference in booster regimens has practical implications for public health planning, as it affects resource allocation, logistics, and patient compliance. For instance, a two-dose booster regimen for Vaccine B could lead to higher costs and lower adherence rates compared to Vaccine A’s single-dose approach.
Analyzing the cellular immune response provides additional insights into long-term immunity. Vaccine A induces a stronger memory T-cell response, which persists for at least 12 months post-vaccination, offering a secondary line of defense against severe disease even if antibody levels wane. Vaccine B, while effective in the short term, shows a less robust T-cell response, particularly in individuals with comorbidities such as diabetes or obesity. This suggests that Vaccine A may offer more durable protection, especially in high-risk populations, reducing the urgency for frequent booster shots.
From a practical standpoint, individuals vaccinated with Vaccine B should monitor their antibody levels through serological testing, particularly if they are over 60 or immunocompromised. If levels fall below the protective threshold, a booster dose should be administered promptly, following local health guidelines. For Vaccine A recipients, a booster may be deferred until 8–10 months post-primary series, unless there is a surge in variant cases or personal risk factors warrant earlier intervention. Employers and healthcare providers can facilitate this by offering on-site booster clinics and educating individuals about the importance of timely revaccination.
In conclusion, the choice between the two vaccines hinges not only on their initial efficacy but also on their long-term immunity profiles and booster requirements. Vaccine A’s sustained antibody levels and robust T-cell response make it a stronger candidate for durable protection, particularly with a single booster dose. Vaccine B, while effective, may necessitate more frequent boosters, especially in vulnerable populations. As new data emerge, ongoing monitoring and adaptive strategies will be essential to maximize the benefits of both vaccines in the fight against the pandemic.
Pneumonia Vaccine Frequency for Cancer Survivors: Expert Recommendations
You may want to see also
Frequently asked questions
Both Pfizer and Moderna are highly effective mRNA vaccines, with similar efficacy rates against COVID-19. The choice often depends on availability, age restrictions, and personal or medical considerations. Consult a healthcare provider for personalized advice.
Both AstraZeneca and Johnson & Johnson are effective in preventing severe COVID-19 outcomes, but they use different technologies. AstraZeneca requires two doses, while Johnson & Johnson is a single-dose vaccine. The better choice depends on individual health conditions and regional recommendations.
Pfizer has shown higher efficacy rates in preventing symptomatic COVID-19 compared to Sinovac. However, Sinovac remains effective in preventing severe illness and hospitalization. The choice may depend on availability and local health guidelines.
Moderna is a two-dose mRNA vaccine with high efficacy, while Johnson & Johnson is a single-dose viral vector vaccine. Moderna generally offers higher protection levels, but Johnson & Johnson provides convenience and is suitable for those who cannot receive mRNA vaccines. The decision should be based on individual needs and medical advice.