Inactivated vaccines are a crucial component of modern medicine, offering protection against various diseases by using pathogens that have been killed or rendered non-infectious. These vaccines work by triggering the immune system to produce antibodies without the risk of causing the disease itself. A prime example of an inactivated vaccine is the influenza vaccine, commonly known as the flu shot. This vaccine contains inactivated influenza viruses, which stimulate the body's immune response to recognize and combat the virus if exposed in the future. Other examples include the polio vaccine (IPV) and the hepatitis A vaccine, both of which use inactivated forms of the respective viruses to provide immunity. Understanding inactivated vaccines is essential for appreciating their role in preventing infectious diseases and promoting public health.
Explore related products


$33.99 $33.99




What You'll Learn
- Polio (IPV): Injects killed poliovirus to trigger immunity without live virus risk
- Hepatitis A: Uses inactivated hepatitis A virus for long-term protection
- Rabies Vaccine: Inactivated rabies virus prevents infection after exposure
- Influenza (Flu Shot): Contains inactivated flu viruses for seasonal protection
- Whole-Cell Pertussis: Inactivated Bordetella pertussis bacteria used in older vaccines
![]()
Polio (IPV): Injects killed poliovirus to trigger immunity without live virus risk
The inactivated poliovirus vaccine, known as IPV, stands as a cornerstone in the global eradication of polio. Unlike its live-attenuated counterpart, IPV contains no viable virus, making it a safer option for individuals with weakened immune systems or those living in regions where the risk of vaccine-derived poliovirus is a concern. This vaccine is administered through injection, typically into the leg or arm, and works by introducing the inactivated virus to the immune system, which then produces antibodies to protect against future infection.
From a practical standpoint, the IPV vaccine is usually given in a series of doses to ensure robust immunity. In the United States, the Centers for Disease Control and Prevention (CDC) recommends a four-dose schedule for children: at 2 months, 4 months, 6-18 months, and 4-6 years. Adults who are at increased risk of exposure to poliovirus, such as travelers to endemic areas or healthcare workers, may also receive IPV. A single dose of IPV is 0.5 mL for both children and adults, delivered intramuscularly or subcutaneously. It’s crucial to follow the recommended schedule, as incomplete vaccination can leave gaps in immunity.
One of the key advantages of IPV is its safety profile. Since the virus is completely inactivated, there is no risk of the vaccine causing polio, a rare but serious complication associated with the oral polio vaccine (OPV). This makes IPV particularly suitable for immunocompromised individuals, pregnant women, and those with certain medical conditions. However, it’s important to note that IPV may not provide the same level of intestinal immunity as OPV, which can limit its effectiveness in preventing viral shedding and transmission in communities.
Comparatively, IPV’s role in polio eradication efforts is distinct from OPV’s. While OPV is more effective in interrupting wild poliovirus transmission due to its ability to induce mucosal immunity, IPV is favored in countries that have eliminated polio to avoid the rare risk of vaccine-associated paralytic polio (VAPP). This strategic shift from OPV to IPV in many regions reflects a global transition from eradication to sustained immunity without live virus risks. For parents and caregivers, understanding this difference is essential when discussing vaccination options with healthcare providers.
In practice, administering IPV requires attention to detail. The vaccine should be stored at 2°C to 8°C and protected from light. Healthcare providers must ensure the correct dosage and route of administration, as errors can compromise immunity. For travelers, carrying documentation of vaccination is advisable, especially when visiting countries with polio outbreaks. While IPV is highly effective, it’s not a standalone solution; maintaining high vaccination coverage and surveillance remains critical to preventing polio’s resurgence. This inactivated vaccine exemplifies how modern science balances safety and efficacy in disease prevention.
Vaccines Triumph: Eradicating Diseases and Saving Lives Globally
You may want to see also
Explore related products






![]()
Hepatitis A: Uses inactivated hepatitis A virus for long-term protection
Hepatitis A vaccines stand out as a prime example of inactivated vaccines, offering robust, long-term protection against a virus that causes acute liver inflammation. Unlike live attenuated vaccines, which use weakened forms of the virus, inactivated vaccines contain viruses that have been killed, eliminating the risk of the vaccine causing the disease it aims to prevent. This method ensures safety while still triggering a strong immune response, making it ideal for individuals with compromised immune systems or those at high risk of severe complications from Hepatitis A.
The Hepatitis A vaccine is typically administered in two doses, with the initial dose followed by a booster shot 6 to 12 months later. This schedule ensures the development of antibodies that provide immunity for over 20 years, and possibly even a lifetime. The vaccine is recommended for children aged 12 to 23 months, travelers to regions with high Hepatitis A prevalence, men who have sex with men, people with chronic liver disease, and those experiencing homelessness. For adults, a combined Hepatitis A and B vaccine is also available, streamlining protection against both viruses.
One of the key advantages of the inactivated Hepatitis A vaccine is its safety profile. Side effects are generally mild and may include soreness at the injection site, headache, or fatigue. Serious adverse reactions are extremely rare, making it a reliable choice for widespread use. Its efficacy is well-documented, with studies showing that over 95% of recipients develop protective antibodies after the full series. This high success rate underscores its role as a cornerstone of preventive medicine.
Practical considerations for vaccination include ensuring timely administration of the booster dose to maximize immunity. For travelers, it’s advisable to receive the first dose at least 2 weeks before departure, as this provides initial protection. While the vaccine is highly effective, it does not replace safe practices such as proper hand hygiene and avoiding contaminated food or water, especially in endemic areas. Combining vaccination with these precautions offers comprehensive defense against Hepatitis A.
In summary, the inactivated Hepatitis A vaccine exemplifies the power of modern vaccinology, providing long-term protection through a safe and effective method. Its targeted use in at-risk populations and straightforward dosing schedule make it an essential tool in global health efforts. By understanding its mechanism, benefits, and practical application, individuals can make informed decisions to safeguard their health against this preventable disease.
White House Employees: Vaccinated or Exempted?
You may want to see also
Explore related products






![]()
Rabies Vaccine: Inactivated rabies virus prevents infection after exposure
The rabies vaccine stands as a critical tool in preventing a disease that, once symptomatic, is nearly 100% fatal. Unlike live-attenuated vaccines, the rabies vaccine is an inactivated vaccine, meaning it contains a killed version of the rabies virus that cannot cause disease but still triggers a protective immune response. This inactivated form is particularly crucial for post-exposure prophylaxis (PEP), where it works in conjunction with rabies immunoglobulin to neutralize the virus before it reaches the central nervous system. Administered in a series of doses over 14 days, the vaccine is a lifeline for individuals bitten by potentially rabid animals, offering a second chance at survival.
From a practical standpoint, the rabies vaccine regimen is straightforward yet precise. For post-exposure treatment, the World Health Organization (WHO) recommends a five-dose intramuscular injection schedule (days 0, 3, 7, 14, and 28) for previously unvaccinated individuals. However, those who have been previously vaccinated or immunocompromised may follow a modified protocol. The vaccine is typically administered in the deltoid muscle for adults and the anterolateral thigh for children, ensuring optimal absorption. It’s essential to complete the full course without interruption, as partial vaccination may not provide adequate protection. Additionally, immediate wound care—thorough washing with soap and water for at least 15 minutes—is a critical first step before vaccination begins.
Comparatively, the rabies vaccine’s inactivated nature sets it apart from other vaccines like the MMR (measles, mumps, rubella), which uses live-attenuated viruses. This distinction is particularly advantageous in post-exposure scenarios, where the immune system must respond rapidly to a potential threat. The inactivated vaccine’s safety profile also makes it suitable for a wide range of individuals, including pregnant women and those with compromised immunity, though precautions and consultations with healthcare providers are always advised. Its effectiveness in preventing rabies, a disease with no cure once symptoms appear, underscores its role as a cornerstone of public health interventions.
Persuasively, the rabies vaccine exemplifies the power of inactivated vaccines in saving lives. While pre-exposure vaccination is recommended for high-risk groups like veterinarians and travelers to rabies-endemic regions, its true value shines in emergency situations. The cost of PEP, though significant, pales in comparison to the human and economic toll of untreated rabies. By investing in widespread vaccination programs and education, communities can reduce the burden of this preventable disease. Practical tips include knowing local rabies risks, keeping pets vaccinated, and seeking medical attention immediately after any animal bite, even if the risk seems low. In the fight against rabies, the inactivated vaccine is not just a medical tool—it’s a lifeline.
Unveiling the Science: How Vaccines Are Developed and Created
You may want to see also
Explore related products






![]()
Influenza (Flu Shot): Contains inactivated flu viruses for seasonal protection
The influenza vaccine, commonly known as the flu shot, is a prime example of an inactivated vaccine, designed to protect against the ever-evolving strains of the influenza virus. Each year, the vaccine is meticulously updated to match the predicted dominant strains, ensuring seasonal protection for millions worldwide. This annual adjustment is crucial because influenza viruses undergo frequent genetic changes, requiring a tailored approach to immunization.
From a practical standpoint, the flu shot contains inactivated (killed) flu viruses, rendering them incapable of causing illness but still effective in stimulating the immune system. This process involves growing the viruses in eggs or cell cultures, then inactivating them using chemicals like formaldehyde. The vaccine is typically administered as a single dose, with the exception of children under nine years old who may require two doses if they are receiving it for the first time. The recommended dosage for adults and children over six months is 0.5 mL, usually injected into the deltoid muscle for adults and the anterolateral thigh for infants and young children.
One of the key advantages of the flu shot is its broad applicability across age groups. It is approved for individuals aged six months and older, making it a versatile tool in public health. However, certain populations, such as pregnant women, the elderly, and those with chronic conditions like asthma or diabetes, are particularly encouraged to get vaccinated due to their higher risk of severe complications from the flu. For these groups, the flu shot not only reduces the likelihood of infection but also diminishes the severity of symptoms if infection does occur.
Despite its benefits, the flu shot is not without limitations. Its effectiveness can vary from season to season, depending on how well the vaccine strains match the circulating viruses. Additionally, while side effects are generally mild—such as soreness at the injection site, low-grade fever, or muscle aches—some individuals may experience more significant reactions. To maximize protection, it’s advisable to get vaccinated early in the flu season, typically starting in September, as it takes about two weeks for immunity to develop fully.
In conclusion, the influenza vaccine exemplifies the power of inactivated vaccines in preventing widespread illness. Its annual reformulation, broad age applicability, and proven safety profile make it a cornerstone of seasonal health protection. By understanding its mechanism, dosage, and target groups, individuals can make informed decisions to safeguard themselves and their communities against the flu.
The Rise of Anti-Vaccine Beliefs in America: A Historical Perspective
You may want to see also
Explore related products






![]()
Whole-Cell Pertussis: Inactivated Bordetella pertussis bacteria used in older vaccines
Whole-cell pertussis vaccines, once the cornerstone of whooping cough prevention, relied on inactivated *Bordetella pertussis* bacteria to stimulate immunity. Unlike acellular vaccines that use purified components, these older formulations contained the entire killed bacterium, preserving a broad array of antigens. This approach mimicked natural infection more closely, prompting a robust immune response. Administered in a series of doses—typically at 2, 4, 6, and 15–18 months of age, followed by a booster at 4–6 years—the vaccine was a standard in childhood immunization schedules for decades. Its effectiveness was undeniable, contributing to a dramatic decline in pertussis cases worldwide.
However, the whole-cell pertussis vaccine was not without drawbacks. The inclusion of the entire bacterial cell led to a higher incidence of adverse reactions, ranging from mild fever and soreness at the injection site to more severe events like persistent crying, seizures, and, in rare cases, hypotonic-hyporesponsive episodes. These side effects fueled public concern and vaccine hesitancy, prompting a search for safer alternatives. By the 1990s, many countries transitioned to acellular pertussis vaccines, which, while less reactogenic, offered comparable protection with fewer antigens.
From a manufacturing perspective, whole-cell pertussis vaccines were relatively straightforward to produce. The process involved growing *Bordetella pertussis* in culture, inactivating the bacteria using heat or chemicals, and then purifying the suspension. This method was cost-effective, making the vaccine accessible in low-resource settings. However, the variability in bacterial strains and inactivation techniques sometimes led to inconsistencies in potency and safety profiles, further underscoring the need for refinement.
Despite its phase-out in many developed nations, the whole-cell pertussis vaccine remains in use in parts of the world where cost and accessibility are paramount. Its legacy is twofold: it demonstrated the power of inactivated vaccines in disease prevention, while also highlighting the importance of balancing efficacy with safety. For those administering or considering this vaccine, understanding its historical context and limitations is crucial. Always follow local immunization guidelines, monitor for adverse reactions, and educate caregivers about potential side effects to ensure informed decision-making.
Exploring the Diverse World of Vaccines: Types and Purposes
You may want to see also
Frequently asked questions
An inactivated vaccine is a type of vaccine made from a virus or bacterium that has been killed or inactivated using heat, chemicals, or radiation, so it cannot cause disease but can still trigger an immune response.
An example of an inactivated vaccine is the inactivated poliovirus vaccine (IPV), which is used to prevent polio.
Yes, the flu shot is typically an inactivated vaccine, as it contains killed influenza viruses that cannot cause the flu but can stimulate the immune system to produce antibodies.
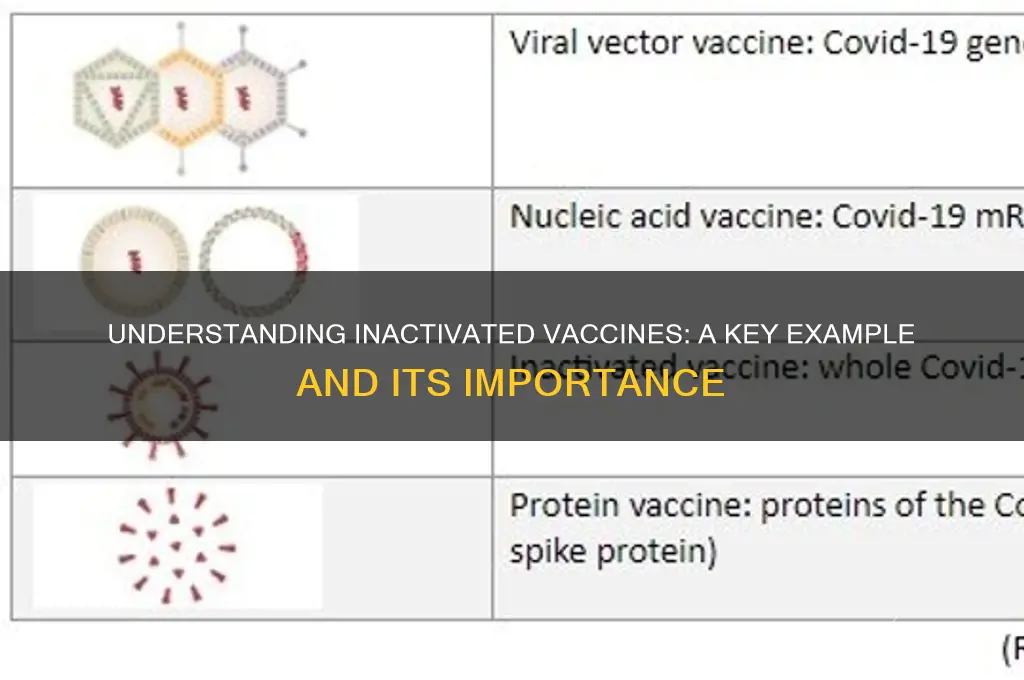
No, not all COVID-19 vaccines are inactivated. Examples of inactivated COVID-19 vaccines include Sinovac (CoronaVac) and Sinopharm, while others like Pfizer-BioNTech and Moderna are mRNA vaccines, and Johnson & Johnson is a viral vector vaccine.