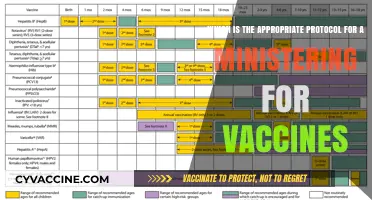
Understanding bacterial vaccines requires knowledge of their development, mechanisms, and efficacy. Key indicators of a good grasp of this topic include familiarity with how vaccines stimulate the immune system to recognize and combat specific bacterial pathogens, such as *Streptococcus pneumoniae* or *Mycobacterium tuberculosis*. A comprehensive understanding also involves recognizing the types of bacterial vaccines, such as conjugate, subunit, or toxoid vaccines, and their respective advantages and limitations. Additionally, awareness of clinical trial data, vaccination schedules, and real-world impact on disease prevention demonstrates a robust comprehension of bacterial vaccines. This knowledge is further reinforced by understanding challenges like antibiotic resistance, vaccine hesitancy, and the need for continuous research to improve vaccine efficacy and accessibility.
| Characteristics | Values |
|---|---|
| Mechanism of Action | Understanding how bacterial vaccines work, including: |
- Stimulation of adaptive immunity (humoral and cell-mediated).
- Induction of memory cells for long-term protection.
- Targeting specific bacterial antigens (e.g., capsular polysaccharides, proteins, or toxins). | | Types of Bacterial Vaccines | Knowledge of vaccine categories:
- Conjugate vaccines (e.g., Hib, pneumococcal).
- Subunit/recombinant vaccines (e.g., acellular pertussis).
- Toxoid vaccines (e.g., tetanus, diphtheria).
- Live attenuated vaccines (e.g., BCG for tuberculosis).
- Inactivated/killed whole-cell vaccines (e.g., typhoid). | | Immunological Response | Awareness of:
- Production of neutralizing antibodies.
- T-cell activation and cytokine release.
- Difference between T-dependent and T-independent antigens. | | Efficacy and Safety | Knowledge of:
- Clinical trial data and vaccine effectiveness.
- Common side effects (e.g., local pain, fever).
- Rare adverse events (e.g., anaphylaxis). | | Targeted Pathogens | Familiarity with bacterial diseases prevented by vaccines, such as:
- Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis, Bordetella pertussis, Corynebacterium diphtheriae, Clostridium tetani. | | Vaccine Development Challenges | Understanding of:
- Antigenic variation in bacteria (e.g., Streptococcus pneumoniae serotypes).
- Difficulty in developing vaccines for Gram-negative bacteria.
- Need for adjuvants in subunit vaccines. | | Public Health Impact | Recognition of:
- Reduction in disease incidence and mortality.
- Herd immunity benefits.
- Role in preventing antibiotic resistance. | | Vaccine Schedule and Administration | Knowledge of:
- Recommended age groups and dosing intervals.
- Route of administration (e.g., intramuscular, subcutaneous).
- Combination vaccines (e.g., DTaP, Tdap). | | Global Access and Equity | Awareness of:
- Vaccine distribution challenges in low-income countries.
- Role of organizations like Gavi, the Vaccine Alliance.
- Impact of vaccine hesitancy. | | Emerging Technologies | Familiarity with:
- mRNA and DNA vaccine platforms for bacterial targets.
- Reverse vaccinology approaches.
- Nanoparticle-based vaccine delivery systems. |
Explore related products




$130.38 $169.99


What You'll Learn
- Vaccine Development Process: Steps from bacterial identification to clinical trials and regulatory approval
- Types of Bacterial Vaccines: Live-attenuated, inactivated, subunit, toxoid, and conjugate vaccines explained
- Immune Response Mechanisms: How vaccines trigger humoral and cell-mediated immunity against bacteria
- Efficacy and Safety: Criteria for evaluating vaccine effectiveness, side effects, and long-term protection
- Global Impact and Challenges: Vaccines' role in reducing bacterial diseases and overcoming distribution hurdles
![]()
Vaccine Development Process: Steps from bacterial identification to clinical trials and regulatory approval
The journey of a bacterial vaccine from concept to clinic is a rigorous, multi-stage process that demands precision, patience, and adherence to strict regulatory standards. It begins with the identification of a bacterial pathogen that poses a significant public health threat, such as *Streptococcus pneumoniae* or *Mycobacterium tuberculosis*. Once the target bacterium is selected, researchers isolate and study its antigens—components like proteins, polysaccharides, or toxins that trigger an immune response. For instance, the pneumococcal conjugate vaccine (PCV) targets the polysaccharide capsule of *S. pneumoniae*, a key virulence factor. This foundational step is critical, as the choice of antigen directly influences the vaccine’s efficacy and safety.
Following antigen identification, the vaccine development process moves into preclinical testing, where potential vaccine candidates are evaluated in laboratory and animal models. Here, researchers assess immunogenicity (the ability to provoke an immune response), toxicity, and dosage requirements. For example, the meningococcal vaccine MenACWY is tested in mice and rabbits to determine the optimal dose of polysaccharide conjugates, typically administered as 0.5 mL intramuscularly for adolescents and adults. This phase also involves stabilizing the vaccine formulation, ensuring it remains effective under various storage conditions, a crucial factor for distribution in low-resource settings.
Once preclinical data demonstrates promise, the vaccine advances to clinical trials, a three-phase process designed to evaluate safety, efficacy, and immunogenicity in humans. Phase I trials involve small groups (20–100 volunteers) to assess safety and dosage, often starting with microgram quantities of antigen. Phase II expands to several hundred participants, focusing on immunogenicity and refining dosage—for instance, the *Haemophilus influenzae* type b (Hib) vaccine was tested at 10 µg and 20 µg doses in infants to determine the best immune response. Phase III trials, the largest and most critical, enroll thousands of participants across diverse populations to confirm efficacy and monitor rare side effects. For the typhoid conjugate vaccine (TCV), Phase III trials demonstrated 87% efficacy in children aged 9 months to 12 years, leading to its approval for use in endemic regions.
Regulatory approval is the final hurdle, where data from all stages are scrutinized by agencies like the FDA or EMA. Manufacturers must provide detailed evidence of quality control, consistency in production, and post-market surveillance plans. For example, the FDA requires vaccines to meet specific criteria, such as a minimum antibody titer for seroprotection, as seen in the pertussis vaccine’s requirement of ≥5 EU/mL of anti-PT antibodies. Once approved, vaccines are continuously monitored through programs like the Vaccine Adverse Event Reporting System (VAERS) to ensure long-term safety. This meticulous process, though time-consuming, ensures that bacterial vaccines are both effective and safe for global use.
Human Tissue in Vaccines: Fact-Checking the Origins and Ethics
You may want to see also
Explore related products






![]()
Types of Bacterial Vaccines: Live-attenuated, inactivated, subunit, toxoid, and conjugate vaccines explained
Bacterial vaccines are categorized based on their composition and mechanism of action, each type offering distinct advantages and applications. Understanding these categories—live-attenuated, inactivated, subunit, toxoid, and conjugate vaccines—is crucial for appreciating how they prevent bacterial infections effectively.
Live-attenuated vaccines contain weakened but still living bacteria, designed to trigger a robust immune response without causing disease. Examples include the Bacillus Calmette-Guérin (BCG) vaccine for tuberculosis and the oral typhoid vaccine (Ty21a). These vaccines mimic natural infection, often requiring fewer doses to confer long-lasting immunity. However, they are contraindicated in immunocompromised individuals due to the risk of the bacteria reverting to a virulent form. For instance, the BCG vaccine is typically administered once at birth or during infancy, providing protection for up to 15 years.
Inactivated vaccines, in contrast, use bacteria that have been killed through physical or chemical methods. This approach eliminates the risk of the bacteria causing disease but often requires adjuvants to enhance immune response. The inactivated polio vaccine (IPV) and the whole-cell pertussis vaccine are prime examples. Multiple doses are usually necessary to achieve and maintain immunity. For IPV, the CDC recommends a series of four doses starting at 2 months of age, with a booster at 4–6 years.
Subunit vaccines focus on specific components of the bacterium, such as proteins or polysaccharides, to stimulate immunity. This precision reduces the risk of adverse reactions compared to whole-cell vaccines. The acellular pertussis vaccine (DTaP) and the meningococcal serogroup B vaccine (Bexsero) are subunit vaccines. Bexsero, for example, is administered in two or three doses depending on age, starting as early as 2 months. Subunit vaccines often require adjuvants to boost their immunogenicity.
Toxoid vaccines target bacterial toxins rather than the bacteria themselves. These toxins are chemically inactivated (detoxified) to form toxoids, which induce the production of neutralizing antibodies. The diphtheria and tetanus vaccines are classic toxoid vaccines, often combined in the DTaP or Tdap formulations. A single dose of Tdap is recommended for adolescents and adults who have completed the primary DTaP series, with boosters every 10 years for tetanus protection.
Conjugate vaccines address a challenge posed by certain bacterial polysaccharide coatings, which are poorly immunogenic in young children. By linking these polysaccharides to a protein carrier, conjugate vaccines enhance immune response. The Haemophilus influenzae type b (Hib) vaccine and the pneumococcal conjugate vaccine (PCV13) are widely used examples. PCV13 is administered in a series of four doses starting at 2 months of age, protecting against 13 pneumococcal serotypes.
Each vaccine type has its niche, tailored to the biology of the target bacterium and the needs of the recipient population. For instance, live-attenuated vaccines are ideal for healthy individuals requiring durable immunity, while conjugate vaccines are essential for protecting infants against encapsulated pathogens. Understanding these distinctions enables healthcare providers to make informed decisions about vaccine selection, dosing, and administration, ultimately optimizing disease prevention strategies.
Understanding Vaccination Timelines: Why Ages Matter for Immunization
You may want to see also
Explore related products


$23.58 $32.99




![]()
Immune Response Mechanisms: How vaccines trigger humoral and cell-mediated immunity against bacteria
Bacterial vaccines harness the immune system’s dual capabilities—humoral and cell-mediated immunity—to provide robust protection against pathogens. Humoral immunity, driven by B cells, produces antibodies that neutralize bacterial toxins or tag pathogens for destruction. Cell-mediated immunity, orchestrated by T cells, targets infected cells and intracellular bacteria. Vaccines like the diphtheria toxoid (0.5 mL dose for adults) exemplify this by stimulating antibody production against the toxin, while BCG (Bacillus Calmette-Württemberg) vaccine activates T cells to combat *Mycobacterium tuberculosis*. Understanding these mechanisms reveals why some vaccines require adjuvants (e.g., aluminum salts) to enhance T cell responses, while others rely on attenuated bacteria to mimic natural infection.
To trigger humoral immunity, vaccines present bacterial antigens—such as polysaccharides or proteins—to B cells. Conjugate vaccines, like the pneumococcal conjugate vaccine (PCV13), link weak bacterial polysaccharides to carrier proteins, enabling B cells to recognize and respond effectively. This is critical for infants under 2 years old, whose immature immune systems struggle with polysaccharide antigens alone. Antibodies produced (e.g., IgG) circulate in the bloodstream, providing immediate defense against reinfection. Booster doses, typically administered 6–12 months after the initial series, reinforce memory B cell populations, ensuring long-term protection.
Cell-mediated immunity, essential for intracellular bacterial infections, relies on vaccines that expose the immune system to live or subunit antigens. The TB vaccine, BCG, introduces a live attenuated strain of *Mycobacterium bovis*, activating CD4+ T cells (helper T cells) and CD8+ T cells (cytotoxic T cells). These cells identify and destroy infected host cells, preventing bacterial replication. For instance, a single 0.05 mL intradermal dose of BCG in newborns primes the immune system to recognize *M. tuberculosis* antigens. However, this response wanes over 10–15 years, highlighting the need for research into more durable T cell-based vaccines.
Practical considerations underscore the importance of vaccine delivery and timing. Inactivated vaccines, like the tetanus toxoid (0.5 mL dose), often require multiple administrations (primary series plus boosters every 10 years) to sustain humoral immunity. Live attenuated vaccines, such as typhoid Ty21a (4 oral capsules over alternating days), stimulate both arms of the immune system but may be contraindicated in immunocompromised individuals. Adjuvants like AS04 (used in the HPV vaccine) enhance antigen presentation to T cells, improving cell-mediated responses. Tailoring vaccine formulations to specific bacterial threats ensures optimal immune activation, balancing safety and efficacy across age groups.
In summary, bacterial vaccines leverage humoral and cell-mediated immunity through strategic antigen delivery and adjuvant use. Humoral responses neutralize toxins and mark pathogens, while cell-mediated responses eliminate infected cells. Vaccines like PCV13 and BCG exemplify these mechanisms, with dosing and schedules optimized for age-specific immune capabilities. By understanding these pathways, healthcare providers can administer vaccines effectively, ensuring broad-spectrum protection against bacterial infections. Practical tips, such as adhering to booster schedules and considering adjuvant roles, further enhance vaccine-induced immunity.
Essential Vaccines for Protecting Newborns: A Guide for Family & Friends
You may want to see also
Explore related products






![]()
Efficacy and Safety: Criteria for evaluating vaccine effectiveness, side effects, and long-term protection
Vaccine efficacy is the cornerstone of public health strategies against bacterial infections, yet it’s a metric often misunderstood. Clinical trials measure efficacy by comparing infection rates in vaccinated versus unvaccinated groups, typically expressed as a percentage reduction in disease incidence. For instance, the *Streptococcus pneumoniae* conjugate vaccine (PCV13) demonstrates 97% efficacy against invasive pneumococcal disease in infants, a gold standard in bacterial vaccine performance. However, real-world effectiveness can vary due to factors like population immunity, pathogen evolution, and vaccine delivery logistics. Understanding this distinction is critical for interpreting vaccine impact and setting realistic expectations for public health outcomes.
Evaluating safety requires a meticulous examination of side effects, both immediate and long-term. Mild reactions such as injection site pain, fever, or fatigue are common and typically resolve within 48 hours. For example, the *MenACWY* meningococcal vaccine often causes soreness in 50–60% of recipients, while severe systemic reactions occur in less than 1% of cases. Rare but serious adverse events, like anaphylaxis or Guillain-Barré syndrome, are rigorously monitored through post-licensure surveillance systems like the Vaccine Adverse Event Reporting System (VAERS). Transparency in reporting and clear communication of risk-benefit ratios are essential to maintaining public trust in vaccination programs.
Long-term protection is a critical yet complex criterion, influenced by factors such as immune memory, pathogen mutation, and vaccine formulation. Booster doses are often necessary to sustain immunity; for instance, the *Tetanus toxoid* vaccine requires decennial boosters to maintain protective antibody levels. In contrast, the *Haemophilus influenzae type b* (Hib) vaccine provides near-lifelong immunity after the primary series in early childhood. Advances in adjuvant technology and mRNA platforms hold promise for extending protection durations, but ongoing research is needed to validate their efficacy against bacterial targets.
Practical considerations for healthcare providers include adhering to age-specific dosing schedules and contraindications. For example, the *Typhoid conjugate vaccine* (TCV) is approved for children as young as 6 months, while live attenuated vaccines like *Bacillus Calmette-Guérin* (BCG) are contraindicated in immunocompromised individuals. Storage conditions, such as maintaining the cold chain for *Cholera* vaccines, also play a pivotal role in ensuring potency. By integrating efficacy data, safety profiles, and logistical requirements, providers can optimize vaccine deployment and maximize population-level benefits.
Is Asking for Vaccination Status in Ontario Illegal? Legal Insights
You may want to see also
Explore related products






![]()
Global Impact and Challenges: Vaccines' role in reducing bacterial diseases and overcoming distribution hurdles
Bacterial vaccines have significantly reduced the global burden of diseases like tuberculosis, pneumonia, and meningitis, saving millions of lives annually. The World Health Organization (WHO) estimates that vaccines prevent 2–3 million deaths each year, with bacterial vaccines playing a pivotal role. For instance, the pneumococcal conjugate vaccine (PCV) has slashed pneumonia cases in children under five by up to 50% in countries with high immunization rates. However, this success is unevenly distributed, with low-income nations often lacking access to these life-saving tools. Understanding this disparity is critical to addressing the global impact and challenges of bacterial vaccines.
One of the most pressing challenges in vaccine distribution is the cold chain requirement, which mandates storage temperatures between 2°C and 8°C. This is particularly problematic in regions with unreliable electricity or inadequate infrastructure. For example, the Bacillus Calmette-Guérin (BCG) vaccine for tuberculosis must be stored at 2°C–8°C, and exposure to higher temperatures can render it ineffective. Innovations like solar-powered refrigerators and thermostable vaccines are emerging solutions, but their implementation remains slow and costly. Without overcoming these logistical hurdles, even the most effective vaccines will fail to reach those who need them most.
Another critical challenge is vaccine hesitancy, fueled by misinformation and cultural barriers. In some communities, skepticism about vaccines, such as the typhoid conjugate vaccine (TCV), hinders uptake despite its proven efficacy in preventing typhoid fever. Public health campaigns must tailor messaging to local contexts, leveraging trusted figures like healthcare workers or religious leaders to build confidence. For instance, in India, community health workers have successfully increased TCV acceptance by addressing concerns in local languages and providing clear, evidence-based information.
To maximize the global impact of bacterial vaccines, equitable access must be prioritized. Initiatives like Gavi, the Vaccine Alliance, have made strides by subsidizing vaccine costs for low-income countries, enabling the introduction of PCV in over 60 nations. However, funding gaps persist, and donor fatigue threatens progress. Policymakers must commit to sustainable financing models, such as advance market commitments, which incentivize vaccine development and distribution. Simultaneously, strengthening local healthcare systems is essential to ensure vaccines are administered effectively, particularly in remote or conflict-affected areas.
In conclusion, while bacterial vaccines have transformed global health, their full potential remains untapped due to distribution challenges and inequities. By addressing cold chain limitations, combating hesitancy, and ensuring sustainable funding, the world can move closer to eradicating preventable bacterial diseases. Practical steps, such as investing in thermostable vaccines and community-driven education, are not just recommendations—they are imperatives for a healthier, more equitable future.
Understanding Government's Police Power in Vaccine Mandates and Public Health
You may want to see also
Frequently asked questions
The primary purpose of bacterial vaccines is to stimulate the immune system to recognize and combat specific bacterial pathogens, preventing or reducing the severity of bacterial infections.
Bacterial vaccines often target components like polysaccharides, proteins, or toxins produced by bacteria, whereas viral vaccines typically target viral proteins or weakened/inactivated viruses.
Examples include the vaccines for *Streptococcus pneumoniae* (pneumococcal vaccine), *Haemophilus influenzae* type b (Hib vaccine), and *Bacillus anthracis* (anthrax vaccine).
Conjugate vaccines combine a weak antigen (e.g., bacterial polysaccharide) with a strong antigen (e.g., protein carrier) to enhance the immune response, particularly in young children and the elderly.
Herd immunity reduces the spread of bacterial pathogens within a population, protecting unvaccinated individuals and decreasing the overall disease burden, even for vaccine-preventable bacterial infections.