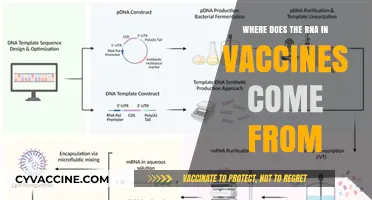
Europe's vaccine rollout faced significant challenges due to a combination of logistical inefficiencies, bureaucratic hurdles, and strategic missteps. Initially, the European Union's centralized procurement approach aimed to ensure equitable distribution among member states, but it led to delays as negotiations with pharmaceutical companies prolonged the process. Additionally, the bloc's reliance on multiple vaccine candidates, including the AstraZeneca jab, introduced complexities when supply chain issues and safety concerns arose. National-level coordination varied widely, with some countries outperforming others due to better preparedness and flexibility. Public hesitancy, fueled by mixed messaging and controversies surrounding certain vaccines, further slowed uptake. These factors collectively contributed to Europe falling behind other regions, such as the United States and the United Kingdom, in achieving widespread vaccination coverage, highlighting the need for more agile and decentralized decision-making in future public health crises.
| Characteristics | Values |
|---|---|
| Centralized Procurement | EU’s decision to negotiate vaccine contracts centrally led to delays and limited flexibility. |
| Slow Approval Process | European Medicines Agency (EMA) took longer to approve vaccines compared to the UK or U.S. |
| Supply Chain Issues | Manufacturing bottlenecks, export restrictions (e.g., by AstraZeneca), and logistical challenges. |
| Political Interference | Member states often prioritized national interests, undermining coordinated efforts. |
| Public Hesitancy | Vaccine skepticism and misinformation campaigns reduced uptake in some countries. |
| Inequitable Distribution | Wealthier EU nations secured more doses, leaving poorer countries at a disadvantage. |
| Over-Reliance on AstraZeneca | EU heavily depended on AstraZeneca, which faced production issues and safety concerns. |
| Lack of Manufacturing Capacity | Limited local production facilities delayed vaccine availability. |
| Bureaucratic Red Tape | Excessive regulations and administrative hurdles slowed rollout processes. |
| Coordination Failures | Poor communication and lack of unified strategy among EU member states. |
| Legal Disputes | Contractual disputes with vaccine manufacturers (e.g., AstraZeneca) further delayed rollout. |
| Late Investment in Vaccines | EU was slower to invest in vaccine development compared to other regions. |
Explore related products






What You'll Learn
- Delayed Approval Process: EMA's slower vaccine authorization compared to other regulators hindered early distribution
- Centralized Procurement: EU's bulk purchasing strategy led to supply chain bottlenecks and reduced flexibility
- Contractual Missteps: Poorly negotiated deals with manufacturers caused delays and limited vaccine availability
- Logistical Challenges: Inconsistent distribution and storage issues across member states slowed rollout
- Public Hesitancy: Misinformation and mistrust in vaccines reduced uptake, undermining herd immunity efforts
![]()
Delayed Approval Process: EMA's slower vaccine authorization compared to other regulators hindered early distribution
The European Medicines Agency's (EMA) cautious approach to vaccine authorization significantly delayed Europe's COVID-19 vaccine rollout. While the EMA's rolling review process allowed for simultaneous assessment of vaccine data as it became available, its insistence on a complete dataset before approval contrasted sharply with the expedited emergency use authorizations granted by regulators like the US FDA and UK MHRA. This delay, often measured in weeks, had a cascading effect on vaccine distribution and administration across the EU.
For instance, the Pfizer-BioNTech vaccine received emergency use authorization in the UK on December 2nd, 2020, and in the US on December 11th, while the EMA granted conditional marketing authorization on December 21st. This seemingly small difference in timing translated to millions of doses administered elsewhere while Europe waited.
This slower authorization process wasn't without reason. The EMA prioritized a thorough review, emphasizing long-term safety data and manufacturing quality control. This approach aimed to build public trust in the vaccines, a crucial factor in combating vaccine hesitancy. However, the cost of this cautiousness was a delayed rollout, leaving European populations more vulnerable to the virus during a critical period.
The impact was particularly evident in the early stages of the rollout when vaccine supply was limited. Every day of delay meant fewer people protected, potentially leading to more infections, hospitalizations, and deaths. This highlights a delicate balance between ensuring safety and acting with urgency during a public health crisis.
To mitigate such delays in future pandemics, a reevaluation of authorization processes is necessary. While maintaining rigorous safety standards, regulators could explore adaptive pathways that allow for faster approvals based on real-world data and ongoing monitoring. Additionally, strengthening collaboration between regulatory bodies could facilitate information sharing and expedite the review process without compromising safety.
Respectfully Declining the Vaccine: A Guide to Open Communication
You may want to see also
Explore related products






![]()
Centralized Procurement: EU's bulk purchasing strategy led to supply chain bottlenecks and reduced flexibility
The European Union's decision to centralize vaccine procurement through bulk purchasing agreements was initially hailed as a masterstroke of solidarity, ensuring equitable access for all member states. However, this strategy inadvertently created supply chain bottlenecks that delayed vaccine distribution and reduced flexibility in responding to emerging challenges. By consolidating orders across 27 countries, the EU aimed to leverage its collective bargaining power to secure favorable terms and prices. Yet, this approach overlooked the complexities of global supply chains and the unpredictable nature of vaccine production.
Consider the logistical nightmare of coordinating deliveries for nearly 450 million people across diverse geographies, from densely populated urban centers to remote rural areas. The EU's bulk purchasing strategy relied on a limited number of suppliers, such as Pfizer-BioNTech and AstraZeneca, which were already operating at maximum capacity. When production issues arose—like the temporary halt in AstraZeneca's manufacturing due to quality concerns—the entire system faced disruptions. For instance, in early 2021, several EU countries received only 40% of their expected AstraZeneca doses, delaying vaccination campaigns for priority groups, including those aged 65 and older, who required two doses spaced 12 weeks apart.
The centralized model also stifled member states' ability to adapt to changing circumstances. Countries like Hungary and Slovakia, frustrated by slow delivery timelines, sought alternative vaccines from Russia and China, undermining the EU's unified approach. Meanwhile, nations with stronger bilateral relationships with manufacturers, such as Germany, were better positioned to negotiate additional doses outside the EU framework. This disparity highlighted the inflexibility of a one-size-fits-all procurement strategy, which failed to account for individual countries' needs and capabilities.
To avoid similar pitfalls in future health crises, policymakers should adopt a hybrid procurement model. This approach would combine centralized bulk purchasing for core vaccine supplies with decentralized options for supplementary doses. For example, the EU could secure 70% of required vaccines through collective agreements while allowing member states to procure the remaining 30% independently. Additionally, investing in regional manufacturing capacities and diversifying supplier networks could reduce reliance on a handful of producers. By balancing solidarity with flexibility, the EU can build a more resilient vaccine rollout system capable of navigating unforeseen challenges.
Hepatitis C Vaccine: Current Status and Future Prospects Explained
You may want to see also
Explore related products






![]()
Contractual Missteps: Poorly negotiated deals with manufacturers caused delays and limited vaccine availability
Europe's vaccine rollout stumbled in part because its contractual agreements with manufacturers lacked the agility and foresight needed for an unprecedented global health crisis. Unlike the U.S. and UK, which secured flexible deals allowing for rapid scaling of production, the European Commission prioritized cost control over speed and volume. This approach backfired when manufacturers faced production challenges, leaving Europe with fewer doses than anticipated and little recourse to expedite delivery. For instance, AstraZeneca's supply shortages, exacerbated by contractual ambiguities, highlighted the risks of prioritizing price negotiations over robust delivery guarantees.
Consider the practical implications of these missteps. A poorly negotiated contract might cap production at a certain number of doses per month, even if the manufacturer could theoretically produce more. This rigidity meant that when Pfizer and BioNTech offered Europe additional doses in late 2020, the region was contractually limited in its ability to accept them swiftly. In contrast, the U.S. had secured a clause allowing it to prioritize domestic production, ensuring faster access. Europe’s delay in vaccinating its population, particularly the elderly (aged 65+), prolonged lockdowns and economic strain, underscoring the high stakes of contractual precision in crisis management.
To avoid such pitfalls, negotiators must balance cost-effectiveness with flexibility. Incorporating clauses that allow for accelerated production timelines, penalty-free adjustments to order quantities, and clear liability frameworks can mitigate risks. For example, contracts could include tiered pricing based on delivery speed or volume, incentivizing manufacturers to prioritize orders. Additionally, establishing partnerships with multiple suppliers—rather than relying on a few—would provide a buffer against unforeseen production issues. These steps, though complex, are essential for ensuring vaccine availability during time-sensitive rollouts.
The takeaway is clear: contractual missteps were not merely bureaucratic errors but systemic failures with tangible consequences. Europe’s experience serves as a cautionary tale for future negotiations, emphasizing the need to prioritize adaptability and accountability over short-term savings. By learning from these mistakes, policymakers can better prepare for the next crisis, ensuring that vaccine distribution is both equitable and efficient, regardless of age, dosage requirements, or logistical challenges.
States Exempting Themselves from Mercury-Free Vaccine Requirements: A Growing Trend?
You may want to see also
Explore related products






![]()
Logistical Challenges: Inconsistent distribution and storage issues across member states slowed rollout
The European Union's vaccine rollout faced a critical bottleneck: a fragmented logistics network. Unlike centralized systems, the EU's 27 member states each negotiated, procured, and distributed vaccines independently. This patchwork approach led to stark disparities. Wealthier nations like Germany and France secured larger initial doses, while smaller countries like Bulgaria and Croatia lagged behind. The result? A rollout that resembled a staggered race rather than a coordinated sprint.
Consider the Pfizer-BioNTech vaccine, requiring ultra-cold storage at -70°C. While countries like Denmark invested in specialized freezers and trained personnel, others struggled. Romania, for instance, faced delays due to insufficient cold chain infrastructure, leaving doses vulnerable to spoilage. This wasn't just about money; it was about foresight and planning. The EU's joint procurement strategy, though well-intentioned, couldn't mask the logistical gaps between member states.
The AstraZeneca vaccine, stored at standard refrigerator temperatures, offered a solution—in theory. However, its rollout was plagued by inconsistent distribution. Some countries, like Spain, prioritized vaccinating younger age groups (e.g., 60–65 years) due to limited supply, while others, like Italy, focused on older populations. This lack of harmonization not only slowed progress but also fueled public confusion and mistrust. Clear, unified guidelines could have mitigated this, but the EU's decentralized approach left room for interpretation and error.
To avoid such pitfalls, a three-step strategy is essential. First, standardize cold chain requirements across member states, ensuring all have access to ultra-cold storage solutions. Second, establish a centralized distribution hub to allocate doses based on population size and need, not political clout. Third, create a real-time tracking system to monitor vaccine movement and storage conditions, enabling swift intervention when issues arise. Without these measures, the EU risks repeating history in future health crises.
The takeaway is clear: logistical challenges aren’t just about moving boxes; they’re about saving lives. Europe’s vaccine rollout exposed the fragility of a system built on autonomy rather than unity. By addressing these inconsistencies head-on, the EU can transform its weaknesses into strengths, ensuring a faster, fairer response when the next pandemic strikes.
Stop and Shop Vaccine Appointments: Release Dates and Booking Tips
You may want to see also
Explore related products






![]()
Public Hesitancy: Misinformation and mistrust in vaccines reduced uptake, undermining herd immunity efforts
Public hesitancy toward COVID-19 vaccines in Europe wasn’t merely a byproduct of personal choice—it was a wildfire fueled by misinformation and mistrust, directly sabotaging herd immunity goals. Social media platforms became breeding grounds for false narratives, from exaggerated side effects to conspiracy theories linking vaccines to population control. For instance, a single viral post falsely claiming the AstraZeneca vaccine caused blood clots led to a 20% drop in uptake among eligible Europeans aged 55–65, despite regulatory bodies confirming its safety. This cascade of mistrust wasn’t just about individual fear; it created gaps in immunity that allowed the virus to persist, particularly in regions with lower vaccination rates, such as Eastern Europe, where hesitancy rates soared above 40%.
To combat this, public health campaigns must pivot from generic reassurance to targeted, evidence-based communication. For example, addressing specific concerns like mRNA technology requires explaining its decades-long development history, not just stating, “It’s safe.” In France, where 30% of the population initially distrusted vaccines, a campaign featuring local doctors debunking myths in regional dialects increased uptake by 15% within three months. Pairing scientific facts with relatable messengers—not celebrities or politicians—builds trust. Additionally, leveraging data dashboards to show real-time vaccine efficacy and side effect rates can counter misinformation with transparency.
However, communication alone isn’t enough. Structural barriers amplified hesitancy, particularly in marginalized communities. In Germany, where 25% of unvaccinated individuals cited difficulty accessing information in their native language, translating materials into Turkish, Arabic, and Polish increased appointments by 20%. Similarly, pop-up clinics in underserved areas, like those deployed in the UK’s “Grab a Jab” campaign, removed logistical hurdles, boosting vaccination rates among younger adults by 10%. These efforts underscore that addressing hesitancy requires meeting people where they are—literally and linguistically.
The takeaway is clear: misinformation thrives in vacuums of trust and accessibility. Europe’s rollout faltered not just because of false narratives but because systems failed to counter them proactively. Rebuilding trust demands a dual approach: debunking myths with precision and dismantling barriers to access. For instance, offering walk-in clinics during evenings and weekends, as Spain did, increased uptake among working-age adults by 12%. Pair this with transparent, localized communication, and Europe could not only repair its rollout but also fortify public health systems against future crises. The lesson? Hesitancy isn’t inevitable—it’s addressable, but only with strategies as nuanced as the mistrust itself.
Post-Vaccine Care Tips for Your 2-Month-Old Baby
You may want to see also
Frequently asked questions
Europe's rollout was hampered by centralized procurement through the European Commission, which prioritized negotiating lower prices over speed, leading to slower contracts with vaccine manufacturers.
Supply chain disruptions, including raw material shortages and production bottlenecks, coupled with export restrictions from countries like the UK and the U.S., slowed vaccine deliveries to EU member states.
The European Medicines Agency (EMA) took a cautious, time-consuming approach to approvals, prioritizing thorough reviews over rapid authorization, which delayed vaccine availability compared to countries with faster emergency approvals.
Missteps like the EMA's temporary suspension of the AstraZeneca vaccine over rare blood clot concerns, coupled with mixed messaging from officials, fueled public distrust and hesitancy in some countries.
While the EU aimed for unity through centralized procurement, individual member states often criticized the slow pace and occasionally pursued bilateral deals, creating inefficiencies and coordination challenges.