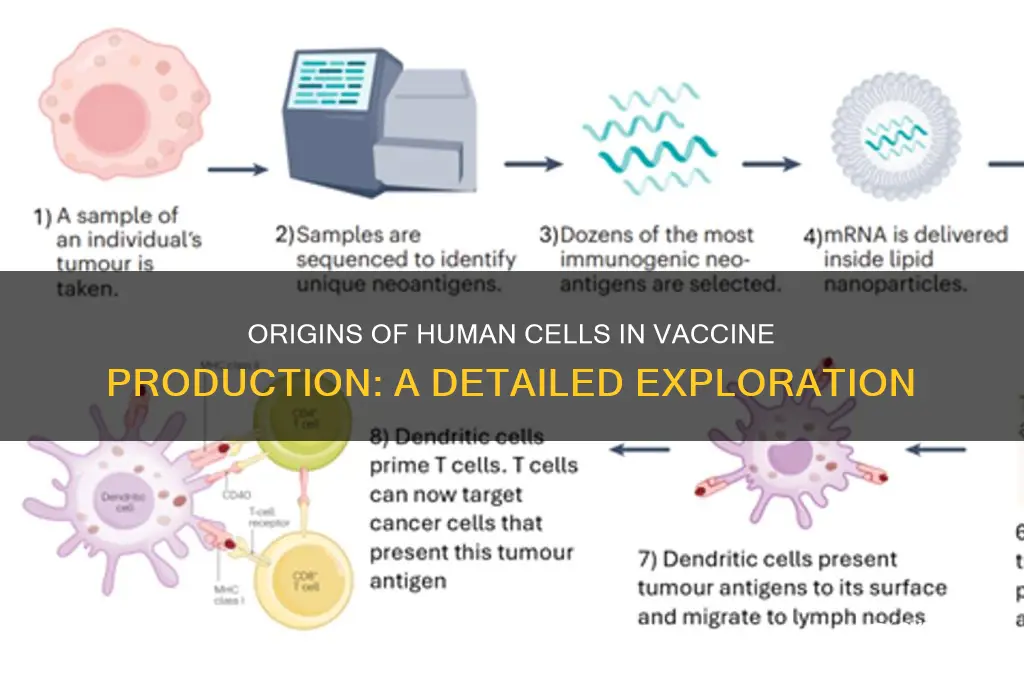
Human cells used in vaccine production are typically derived from established cell lines, which are cultured cells that can be continuously propagated in laboratories. One of the most commonly used cell lines is the Human Diploid Cell Strain WI-38, originally obtained from the lung tissue of a legally aborted fetus in the 1960s. Another widely used line is MRC-5, also sourced from fetal lung tissue. These cells are chosen for their ability to support the growth of viruses and their genetic stability, ensuring consistent vaccine production. Additionally, modern advancements have introduced alternatives such as human embryonic kidney (HEK) cells and insect cells (e.g., Sf9 cells) for certain vaccines. The use of these cells is strictly regulated to ensure ethical sourcing, safety, and efficacy in vaccine development.
| Characteristics | Values |
|---|---|
| Source of Human Cells | Primarily derived from cell lines established decades ago, such as MRC-5 (derived from fetal lung tissue in 1966) and WI-38 (derived from fetal lung tissue in 1962). |
| Origin of Fetal Tissue | Historically obtained from elective abortions, but no new fetal tissue has been used for decades. Existing cell lines are continuously cultured and used for vaccine production. |
| Vaccines Using Human Cell Lines | Examples include Varicella (chickenpox), Rubella (MMR), Hepatitis A, Rabies, and some COVID-19 vaccines (e.g., AstraZeneca and Johnson & Johnson). |
| Ethical Considerations | The use of historical fetal cell lines is widely accepted by major health organizations (WHO, CDC, Vatican) due to the absence of ongoing fetal tissue procurement. |
| Alternatives | Research is ongoing to develop vaccines using non-fetal cell lines or synthetic methods, but current alternatives are not yet widely implemented. |
| Cell Line Immortality | Cell lines like MRC-5 and WI-38 are "immortalized," meaning they can replicate indefinitely in lab conditions, ensuring a consistent supply for vaccine production. |
| Role in Vaccine Production | Human cells are used to grow viruses or viral proteins that are then purified and used in vaccines, ensuring safety and efficacy. |
| Regulatory Approval | Vaccines produced using human cell lines undergo rigorous testing and approval by regulatory bodies like the FDA and EMA. |
| Public Awareness | Transparency about the use of historical fetal cell lines has increased, with health organizations providing detailed information to address public concerns. |
Explore related products






What You'll Learn
- Donor Sources: Cells from human donors, like fetal tissues, are used in vaccine development
- Cell Lines: Immortalized cell lines, e.g., HEK293, are commonly used for vaccine production
- Ethical Considerations: Fetal cell use in vaccines raises ethical and moral debates
- Alternative Methods: Modern techniques explore non-human or synthetic cells for vaccine manufacturing
- Regulatory Standards: Strict guidelines ensure safety and ethical sourcing of human cells in vaccines
![]()
Donor Sources: Cells from human donors, like fetal tissues, are used in vaccine development
Human cells derived from donors, particularly fetal tissues, have been integral to vaccine development for decades. These cells, often obtained from elective abortions, provide a unique environment for cultivating viruses and producing vaccines. The most well-known example is the WI-38 cell line, established in the 1960s from lung tissue of a female fetus. This cell line has been used to develop vaccines for diseases like rubella, chickenpox, and shingles, saving millions of lives globally. The use of fetal cell lines is not widespread in all vaccines; only a select few rely on this method due to its historical efficacy and safety record.
Ethical Considerations and Public Perception
The use of fetal tissues in vaccine production raises ethical concerns for some individuals and groups. Critics argue that sourcing cells from elective abortions is morally problematic, even if the abortions were not performed for this purpose. Proponents counter that the tissues would otherwise be discarded and that their use in life-saving vaccines justifies their application. Transparency in vaccine development processes is crucial to addressing these concerns. For instance, vaccine manufacturers often provide detailed information about cell lines used, ensuring informed decision-making for recipients.
Scientific Advantages of Fetal Cell Lines
Fetal cells are favored in vaccine development due to their rapid growth and stability. Unlike adult cells, fetal cells can divide many times without losing their ability to support virus replication, making them ideal for large-scale vaccine production. For example, the rubella vaccine, developed using the WI-38 cell line, has prevented thousands of congenital rubella syndrome cases annually. This efficiency underscores why fetal cell lines remain a cornerstone of certain vaccine technologies, despite ongoing research into alternative methods.
Alternatives and Future Directions
As ethical debates persist, scientists are exploring alternatives to fetal cell lines. One promising approach involves using cells from adult donors or ethically non-controversial sources, such as pluripotent stem cells. Another method is employing animal cell lines, though these sometimes lack the compatibility needed for human vaccines. Regulatory bodies like the FDA and WHO are actively supporting research into these alternatives to ensure vaccine production remains both ethical and sustainable. For now, fetal cell lines remain a critical, if contentious, tool in the fight against infectious diseases.
Practical Implications for Vaccine Recipients
For individuals concerned about the origins of vaccine components, it’s essential to consult healthcare providers or trusted resources for accurate information. While fetal cell lines are used in specific vaccines, the cells themselves are not present in the final product. The vaccines undergo rigorous purification processes to ensure safety and efficacy. Understanding these details can help recipients make informed choices, balancing ethical considerations with the undeniable benefits of vaccination in preventing disease and protecting public health.
MMR Vaccine for Babies: Post-Shot Symptoms and Care Tips
You may want to see also
Explore related products





![]()
Cell Lines: Immortalized cell lines, e.g., HEK293, are commonly used for vaccine production
Immortalized cell lines, such as HEK293, are the unsung heroes of modern vaccine production. Derived from human embryonic kidney cells in the 1970s, HEK293 cells have been genetically modified to replicate indefinitely, making them a reliable workhorse for manufacturing vaccines. Their ability to efficiently express foreign proteins, like viral antigens, allows scientists to produce large quantities of vaccine components in a controlled environment. This scalability is critical for meeting global demand during outbreaks, as seen with COVID-19 vaccines, where billions of doses were required in record time.
The process begins with introducing genetic material (e.g., DNA or mRNA) encoding the target antigen into the HEK293 cells. These cells then act as tiny factories, synthesizing the antigen, which is later purified and formulated into the vaccine. For instance, the Johnson & Johnson COVID-19 vaccine used HEK293 cells to produce the adenovirus vector carrying the SARS-CoV-2 spike protein. This method ensures consistency across batches, a key advantage over traditional egg-based production, which can be prone to variability.
While HEK293 cells are widely used, their origin from embryonic tissue has sparked ethical debates. However, it’s important to note that these cells are decades old and no longer linked to their original source. Regulatory bodies, including the FDA and WHO, have deemed their use safe and ethical, emphasizing their role in saving millions of lives. Alternatives, such as insect or yeast cells, are also employed, but HEK293 remains preferred for its human-like protein processing, which ensures proper antigen folding and functionality.
For researchers or manufacturers considering HEK293 cells, optimizing growth conditions is crucial. These cells thrive in a humidified incubator at 37°C with 5% CO2, using serum-free media to minimize contamination risks. Passaging should occur every 2–3 days to maintain viability, and regular testing for mycoplasma is essential to avoid compromising the culture. When scaling up, bioreactors with controlled pH and oxygen levels ensure consistent productivity, a critical factor for meeting dosage requirements, typically ranging from 0.5 to 1 mL per vaccine dose.
In conclusion, HEK293 cells exemplify the intersection of biology and technology in vaccine development. Their immortality, coupled with their protein-producing prowess, makes them indispensable for rapid, large-scale manufacturing. While ethical considerations persist, their proven track record underscores their value in global health. For practitioners, mastering their cultivation and application is key to advancing vaccine accessibility and efficacy.
America's Most Vaccinated City: Unveiling the Leader in Immunization Efforts
You may want to see also
Explore related products






![]()
Ethical Considerations: Fetal cell use in vaccines raises ethical and moral debates
The use of fetal cell lines in vaccine development, particularly those derived from abortions decades ago, has sparked intense ethical and moral debates. These cell lines, such as WI-38 and MRC-5, have been instrumental in producing vaccines for diseases like rubella, chickenpox, and hepatitis A. While the original fetal tissue was obtained with consent and long before the vaccines were developed, the historical connection to abortion remains a contentious issue. This raises questions about the moral responsibility of using such cells, even when they have saved millions of lives.
From an analytical perspective, the ethical dilemma hinges on the principle of double effect, a philosophical framework that evaluates actions with both good and bad consequences. Proponents argue that the use of these cell lines is justifiable because the original act (abortion) was not performed with the intent of vaccine development, and the greater good (disease prevention) outweighs the moral concerns. Critics, however, contend that any utilization of fetal tissue, regardless of its origin, normalizes practices they deem unethical. This debate is further complicated by differing cultural, religious, and legal perspectives on abortion and fetal tissue research.
Instructively, individuals grappling with this issue should consider the following steps: first, educate themselves on the specific vaccines involved and the historical context of the cell lines used. Second, weigh the public health benefits against personal ethical beliefs. Third, explore alternative vaccines or medical options if available, though these are often limited. For example, some vaccines, like the newer shingles vaccine Shingrix, do not rely on fetal cell lines. However, for diseases like rubella, alternatives are not always feasible, leaving individuals with a difficult decision.
Persuasively, it’s crucial to recognize that the fetal cell lines in question are not continuously sourced from new abortions but are self-replicating descendants of cells obtained decades ago. This distinction is vital for understanding the ethical landscape. While the initial procurement of the cells remains a point of contention, their ongoing use does not directly contribute to further abortions. This fact should temper the debate, encouraging a focus on the broader implications of vaccine refusal, such as increased disease transmission and public health risks.
Comparatively, the ethical debate over fetal cell use in vaccines parallels discussions around other medical practices, such as organ donation or blood transfusions, where personal beliefs often clash with societal needs. Just as Jehovah’s Witnesses may refuse blood transfusions based on religious grounds, individuals opposed to fetal cell use may opt out of certain vaccines. However, unlike refusing a transfusion, which primarily affects the individual, vaccine refusal can have communal consequences, particularly for vulnerable populations like infants or immunocompromised individuals.
In conclusion, the ethical considerations surrounding fetal cell use in vaccines are complex and deeply personal. By approaching the issue with a balanced understanding of history, science, and philosophy, individuals can make informed decisions that align with their values while considering the broader impact on public health. For those seeking alternatives, consulting healthcare providers and staying informed about vaccine developments is essential. Ultimately, this debate underscores the need for continued dialogue and transparency in medical research and practice.
Maryland Cat Rabies Vaccination Schedule: Frequency and Requirements Explained
You may want to see also
Explore related products






![]()
Alternative Methods: Modern techniques explore non-human or synthetic cells for vaccine manufacturing
The traditional reliance on human cell lines for vaccine production, such as the widely used MRC-5 and WI-38, has been a cornerstone of medical science for decades. However, the quest for more efficient, scalable, and ethically unburdened methods has spurred innovation in vaccine manufacturing. Modern techniques are now exploring non-human and synthetic cells as viable alternatives, offering promising solutions to longstanding challenges in vaccine development and distribution.
One of the most groundbreaking approaches involves the use of insect cells, particularly those derived from the fall armyworm (*Spodoptera frugiperda*). These cells, when infected with recombinant baculoviruses, can produce large quantities of viral proteins or virus-like particles (VLPs) used in vaccines. For instance, the FDA-approved FluBlok, a seasonal influenza vaccine, utilizes this method. Insect cells offer several advantages: they grow rapidly in serum-free media, reducing contamination risks, and their post-translational modifications are compatible with many human proteins. This technique is particularly useful for producing vaccines against complex viruses like influenza, where traditional egg-based methods often fall short in scalability and antigenic match.
Another innovative strategy leverages plant-based systems, which use plant cells or leaves to express vaccine antigens. Plants like tobacco (*Nicotiana benthamiana*) are genetically engineered to produce specific viral proteins, which are then extracted and purified for vaccine formulation. This method has been explored for vaccines against diseases such as COVID-19, Zika, and influenza. Plant-based systems are cost-effective, scalable, and free from the risk of mammalian pathogens. For example, Medicago’s COVID-19 vaccine candidate, which uses plant-derived VLPs, demonstrated efficacy in clinical trials and received approval in Canada. While still in its early stages, this approach holds immense potential for rapid vaccine production during pandemics.
Synthetic biology is also revolutionizing vaccine manufacturing through the use of cell-free systems. These systems bypass the need for living cells altogether by using purified cellular components, such as enzymes and ribosomes, to synthesize proteins in vitro. This method is particularly advantageous for producing complex antigens that are difficult to express in living cells. For instance, cell-free systems have been used to manufacture personalized cancer vaccines, where tumor-specific antigens are synthesized on demand. While still experimental, this technique offers unparalleled flexibility and precision, potentially enabling the development of tailored vaccines for individual patients.
Despite their promise, these alternative methods are not without challenges. Insect and plant cells may require additional processing to ensure proper protein folding and glycosylation, which are critical for vaccine efficacy. Cell-free systems, while highly customizable, are currently limited by high costs and low yields. However, ongoing research and technological advancements are steadily addressing these hurdles. For example, optimizing growth conditions for insect cells and developing more efficient extraction methods for plant-based systems are areas of active exploration.
In conclusion, the shift toward non-human and synthetic cells in vaccine manufacturing represents a paradigm shift in medical science. By harnessing the unique advantages of insect, plant, and cell-free systems, researchers are paving the way for more sustainable, scalable, and ethically sound vaccine production. As these technologies mature, they hold the potential to transform global health by ensuring rapid and equitable access to life-saving vaccines.
Whooping Cough Vaccine: Is a Single Dose Enough for Life?
You may want to see also
Explore related products






![]()
Regulatory Standards: Strict guidelines ensure safety and ethical sourcing of human cells in vaccines
Human cells used in vaccine production are subject to rigorous regulatory standards that prioritize safety, efficacy, and ethical sourcing. These standards are enforced by global health authorities such as the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), and the World Health Organization (WHO). For instance, cell lines derived from human tissues must be fully documented, with traceability back to the original donor. This ensures that cells used in vaccines, like the HEK 293 cell line, are free from contaminants and ethically obtained, often from consented medical procedures or historical samples.
One critical aspect of regulatory compliance is the prevention of adventitious agents—unintended pathogens that could compromise vaccine safety. Manufacturers must adhere to Good Manufacturing Practices (GMP), which include sterile handling, regular testing, and validation of production processes. For example, cell cultures are screened for viruses, bacteria, and fungi using methods like polymerase chain reaction (PCR) and next-generation sequencing (NGS). These measures ensure that vaccines, such as those for COVID-19 or influenza, meet purity standards before distribution.
Ethical sourcing is another cornerstone of regulatory guidelines. Human cells used in vaccines are typically derived from established cell lines rather than primary cells, reducing the need for ongoing tissue donation. However, when new cell lines are developed, informed consent from donors is mandatory. Regulatory bodies also prohibit the use of cells from vulnerable populations or those obtained through coercion. This ethical framework builds public trust and ensures vaccines are developed with respect for human rights.
Practical implementation of these standards involves a multi-step process. First, cell lines are characterized and banked under controlled conditions. Second, manufacturers conduct preclinical and clinical trials to demonstrate safety and efficacy, often involving thousands of participants across age categories (e.g., children, adults, and the elderly). Finally, post-market surveillance monitors adverse events, ensuring long-term safety. For example, the FDA’s Vaccine Adverse Event Reporting System (VAERS) allows healthcare providers and the public to report issues, triggering rapid regulatory response if needed.
In conclusion, regulatory standards for human cells in vaccines are not just bureaucratic hurdles but essential safeguards. They ensure that vaccines are safe, ethically sourced, and effective for diverse populations. By adhering to these guidelines, manufacturers and health authorities protect public health while fostering confidence in vaccination programs. Understanding these standards empowers individuals to make informed decisions about their health and the health of their communities.
Lichen Sclerosus and COVID-19 Vaccines: Prioritizing Skin Condition Concerns
You may want to see also
Frequently asked questions
The human cells used in vaccine production are typically derived from established cell lines, such as the HEK 293 (human embryonic kidney) or MRC-5 (human lung fibroblast) cell lines. These cell lines were originally obtained decades ago and have been continuously cultured in laboratories.
Some vaccines, such as certain rabies, chickenpox, and hepatitis A vaccines, were developed using fetal cell lines (e.g., WI-38 or MRC-5) derived from abortions performed in the 1960s. However, the vaccines themselves do not contain fetal tissue; the cells are used in the manufacturing process to grow viruses or produce proteins.
No, the human cells used in vaccine production are not capable of causing genetic changes in recipients. The cells are used to grow viruses or produce vaccine components, and they are thoroughly purified during the manufacturing process to ensure no intact cells remain in the final product.
Yes, alternatives to human cell lines include animal cell lines, insect cells, yeast, bacteria, and plant-based systems. However, human cell lines are often preferred for certain vaccines because they can more accurately replicate human viruses, ensuring the vaccine’s effectiveness and safety.